

Full Length Research Article
Neutropenic fever in patients with Hematologic Malignancies: Microorganisms and antimicrobial susceptibility
Huda A. Al-Shawy, Ali K. Jumaa*
Adv. life sci., vol. 12, no. 1, pp. 275-281, February 2025
*– Corresponding Author: Ali K. Jumaa (Email: alikj83@yahoo.com)
Authors' Affiliations
[Date Received: 16/06/2023; Date Revised: 24/11/2024; Date Published: 20/01/2025]
Editorial Expression of Concern:
18 May 2025: Following publication of this paper, the internal audit (consequent to concerns on quality raised by Web of Science) notified Advancements in Life Sciences about problems in use of English language and references. By this Editorial Expression of Concern, we alert the scientific community as we address the errors.
Editorial Note:
31 May 2025: You are viewing the latest version of this article having minor corrections related to the use of English language and in references section. Expression of concern is hereby revoked.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Neutropenic fever is a life-threatening complication for patients with hematological malignancies during the course of their management. Early and precise detection of causative microorganisms are crucial. The purpose of this study was to identify the spectrum of these microorganisms and antimicrobial susceptibility.
Methods: A total of 58 patients with proven hematological malignancies at The Basrah Center for Oncology and Hematology were included. Blood samples were inoculated into bottles of Bract/Alert blood culture system and sent to the reference lab for study. Culture from positive bottles were plated on appropriate media, and incubated at 37°C and 30°C for bacterial and fungal isolation, respectively. a bacterial suspension with a turbidity equivalent to 0.5 McFarland (1.5 × 108 CFU/mL) was prepared and used for the Vitec2 system (bioMerieux). Statistical analysis using SPSS software version 26 was used for statistical analysis.
Results: Among 58 patients with approved hematologic malignancies, 29.31% (n:17) samples established positive blood culture. Of them, 9 were gram-negative (15.52%) and 4 were gram-positive bacteria (6.89%), 1 was gram-positive bacillus facultative anaerobe (1.73) and, 3 patients (5.17%) showed fungemia.
Conclusion: Thirty- five % of the samples studied were culture-positive. The most frequent microorganisms were gram-positive bacteria. CRP is a useful predictor of mortality for febrile neutropenic patients.
Keywords: Neutropenic fever; Blood culture; Chemotherapy; hematologic malignancies
Introduction![]()
Chemotherapy-induced neutropenia (CIN) is a hematologic toxicity caused by the cytotoxic effects of chemotherapy that can result in neutrophil suppression [1]. Neutrophils are mature white blood cells produced in the bone marrow and released into the circulating blood as first line defense against infection. Neutrophils (also known as polymorphonuclear leukocytes) are phagocytes that play an important role in protecting the host against pathogens such as bacteria and fungi [2]. The absolute neutrophil count (ANC), usually ranges from 1500 to 7000 neutrophils/microliter in adults. Whereas a decrease in the absolute neutrophil count below 1500 is called neutropenia. As a result, a decrease in neutrophil counts below this threshold may weaken the body's immunity and increase susceptibility to infection, particularly in cancer patients [3,4].
Neutropenia is defined as a neutrophil count of <1500 cells/mL. Severe neutropenia is defined as having an absolute neutrophil count of <500 cells/mL or expecting an absolute neutrophil count of 500 cells/mL within the next 48 hours. The risk of infection increases as the neutrophil count decreases, and this risk increases further as the duration of neutropenia increase [5].
However patients with hematologic malignancies are predisposed to severe infections, especially during chemotherapeutic treatment. In these patients, the resulting neutropenia is a major cause of morbidity and mortality. Depending on the extent and duration of neutropenia, as well as additional cellular and/or humoral immunosuppression and disruption of skin and mucosal barriers, neutropenic cancer patients are at high risk of infectious complications [6].
Neutropenic fever is a serious side effect of cytotoxic chemotherapy treatment in cancer patients. When absolute neutrophil count is 500 cells/mm3 or a count of <1,000 cells/mm3 with a predicted decline to <500 cells/mm3, for which an oral temperature of ≥ 38.3 °C or ≥38 °C for more than 1 hour is considered an increased risk of infection and mortality. In cancer patients, fever may be the only symptom of underlying infections following chemotherapy treatment [7].
It is critical to recognize neutropenic fever early and to initiate a proper empiric systemic antibacterial therapy promptly in order to avoid progression to a sepsis syndrome and possibly death, which requires thorough knowledge of the causative microorganisms and antimicrobial sensitivity [8].
Methods![]()
The current study included 58 cases of Neutropenic fever in 58 adult leukemia patients who underwent chemotherapy and were enrolled in the Basrah Center for Oncology and Hematology from October 2021 to June 2022.
This study conducted according to the approvals of the Iraqi Ministry of Health / Basra Health Department No 58/2021 as of date 24/10/2021, task facilitation to Al-Sader Teaching Hospital and Basrah Center for Oncology and Hematology No 749 as of date 24/10/2021.
The patients were informed about the purpose of blood sampling that was to be sent for CBC and culturing to demonstrate the underlying pathogen behind their fever. They were 41 (70.7%) males and 17 (29.3%) females; the patient ages ranged from 14 and 80 years. All of these cases suffered from hematological malignancy. Patients with hematologic malignancies with neutropenic fever were divided into four groups according to absolute neutrophil count (mild neutropenia: ANC < 1500/mm3, moderate neutropenia: ANC < 1000/mm3, severe neutropenia: ANC < 500/mm3, very severe neutropenia: ANC < 200/mm3).
Inclusion criteria in this study include all adult patients with hematological malignancy undergoing chemotherapy who presented with neutropenic fever, body temperature of ≥ 38.3 °C on one occasion, or ≥ 38 °C that sustained over 1 hour, with absolute neutrophil count of <1500/mm3.
Blood collection, CBC and BacT/ Alert system
Each patient had a venous blood sample of 12 mL taken intravenously. After skin cleaning, 10ml of collected blood was utilized to inoculate the blood bottle according to usual procedure. In a BacT/ALERT blood culture system (BacT/Alert FA Plus, bioMerieux SA, France), the infected bottles of blood were incubated at 35± 2°C. Bottles of BACT/Alert that exhibited signs of growth were agitated. All samples were submitted to the Al-Sadr Teaching Hospital, Clinical and Special Laboratory right away and incubated in a BacT/Alert blood system at 35±2°C. 2 mL of the leftover blood was transferred to the CBC container, which also contained EDTA, and delivered to the hospital laboratory.
Bacterial identification and antimicrobial susceptibility testing (AST) using VITEC 2 system
To use this technique we need pure bacterial cultures. So, all affirmatively alarmed BacT/Alert system bottles were sub-cultured on 5% sheep blood culture, MacConkey agar, and Sabouraud dextrose agar (SDA) for bacterial and fungus growth, respectively, at 37°C and 30°C.
Bacterial identification and antibiotic susceptibility testing (AST) was done using automated VITEC2 system (bioMerieux, France). In order to choose suitable identification (ID) and AST cards, basic identification tests such as Gram staining, catalase and oxidase tests were done according to standard bacteriology protocol on all positive blood agar and MacConkey agar plates.
A bacterial suspension was made from each pure culture with a turbidity of 0.5 McFarland (1.5×108 CFU/ml) based on VITEC2 construction. All of the prepared bacterial suspensions, as well as specific ID and AST cards, were simultaneously placed into the VITEC2 system apparatus. Following identification, the minimum inhibitory concentration (MIC) for each antibiotic was calculated. All antibiotics were chosen using the CLSI guidelines [9].
Fungi identification and antifungal susceptibility testing (AST)
Fungal identification and antibiotic susceptibility testing (AST) was done using automated VITEC2 system (bioMerieux, France). In order to choose suitable identification (ID) and AST cards. Methylene blue was used to microscopically evaluate all Sabouraud dextrose agar (SDA) plates that indicated fungal colonies.
A fungal suspension was made from each pure culture with a turbidity of (1.80-2.20) McFarland based on VITEC2 construction. All of the prepared fungal suspensions, as well as specific ID and AST cards, were simultaneously placed into the VITEC2 system apparatus. Antifungal agents including; the following treatments: amphotericin B, voriconazole, caspofungin, fluconazole, itraconazole and micafungin have been used in antifungal susceptibility testing.
Statistical Analysis
The analysis was done using the SPSS software, version 26. For descriptive purposes, frequencies and percentages were used for qualitative data and mean± standard deviation with median, minimum and maximum values were used for quantitative data. Shapiro-Willk and Kolmogorove-Smirnov tests were used to investigate quantitative data parametry. Mann Whitney U Test and Fisher's Exact Test were used to investigate the statistical significance of any difference/ association appeared in the comparisons made.
Results![]()
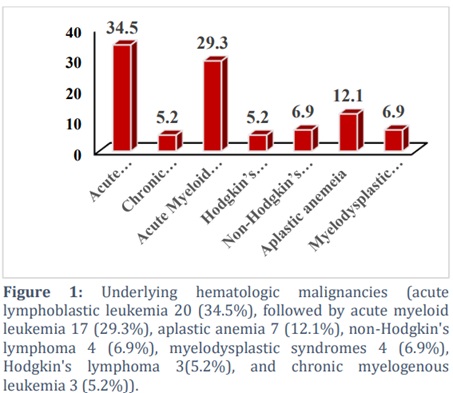
Patients' ages ranged between (14-80 year), at Basra Center for Oncology and Hematology during the period from October 2021 to June 2022. The ratio of males to females was 2.41:1. The majority of patients had Acute Lymphocytic Leukemia (34.5%) and Acute Myeloid Leukemia (29.2%) (Fig 1).
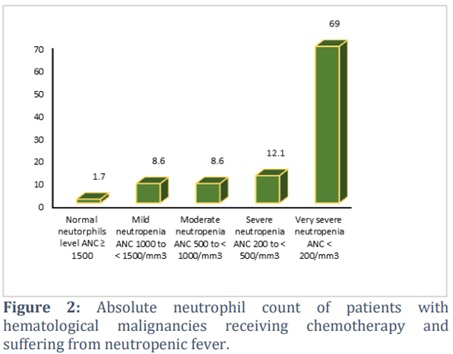
All patients received chemotherapy. The absolute neutrophil count for patients had: ANC ≥1500/mm3 (1.7%), ANC 1000 to <1500/mm3 (8.6%), ANC 500 to <1000/mm3 (8.6%), ANC 200 to <500/mm3 (12.1%), ANC <200/mm3 (69.0%) (Fig 2).
Frequency of the detectable microorganisms among the studied population
All of these episodes found a positive culture with a single pathogen. The pathogenic microorganisms that were isolated from the patients were gram-negative bacteria (n = 9, 15.52%), gram-positive bacteria (n = 4, 6.89%), fungi (n = 3, 20%), Anaerobic Bacteria (n = 1, 1.73 %). From gram-positive bacteria, Staphylococcus aureus and Staphylococcus hominis were identified using a VITEC2 gram-positive ID card. Isolated gram-negative bacteria, Escherichia coli and Klebsiella pneumoniae were detected using VITEC2 with a gram-negative ID card. Facultative anaerobic bacteria Bacillus cereus has been identified in vitro.
Identification of Fungal species by VITEK 2 system (BioMerieux)
After the appearance of growth on the culture plate (Sabouraud Dextrose Agar) and sending the isolates to a laboratory for fungal diagnosis using the VITEK 2 system (BioMerieux), the following results were obtained: Rhodotorula glutinis /mucilaginosa 1(1.7%), Candida dubliniensis 1 (1.7%), Candida parapsilosis 1 (1.7%).
Antimicrobial susceptibility of the gram- negative bacteria
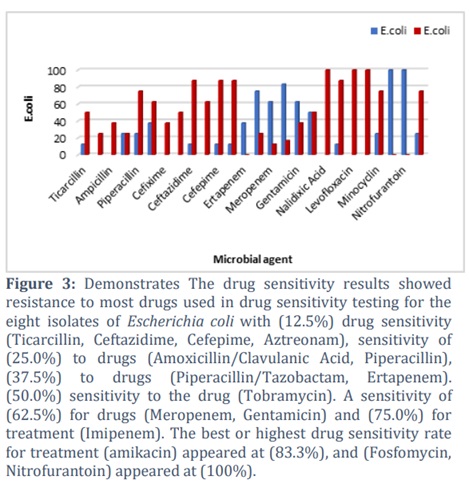
The results of antibiotic susceptibility testing for gram-negative bacteria were eight isolates of Escherichia coli, shown in (Fig 3), and only one isolate of Klebsiella pneumoniae was resistant to all drugs. Use the drug sensitivity to (26 treatments) according to the results of the VITEK 2 (BioMerieux) regimen.
One isolate of Echerichia coli that showed resistance to standard antibiotics, so we tried to test for Tigecycline, a broad-spectrum antibiotic, and the results were as follows:
The drug was not sensitive to Escherichia coli bacteria, as the drug was tested on three bacterial isolates, including the resistant one, none of which showed a response to treatment. While the response to Klebsiella pneumoniae had the best drug-sensitivity diameter (38 cm), the resistant isolate was not the one diagnosed as completely resistant to treatment. A sample of Enterobacter bacteria was also used, and the response to treatment was good sensitivity, with a diameter of (45 mm). These types of bacteria were used in the test as stated in the prescription that accompanies the treatment.
Antimicrobial susceptibility of the gram-positive bacteria
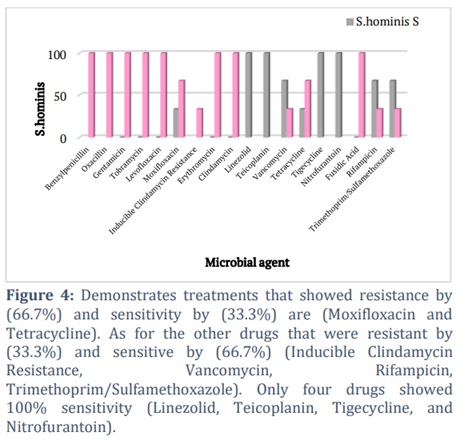
The results of the antimicrobial susceptibility test for gram-positive bacteria were according to the results of the VITEK2 (BioMerieux) system. Three isolates of Staphylococcus hominis showed sensitivity and drug resistance as shown in (Fig 4), and only one isolate of Staphylococcus aureus was sensitive to all drugs.
Antimicrobial susceptibility of the Fungal
The results of antimicrobial susceptibility testing for fungi were for three isolates of Rhodotorula glutinis /mucilaginosa, Candida dubliniensis, and Candida parapsilosis.
The drug sensitivity of Rhodotorula glutinis /mucilaginosa isolates has not been recognized using the VITEK 2 (BioMerieux) system due to the lack of Cards for Antimicrobial Susceptibility Testing (AST) for this type of yeast. Therefore, In vitro drug sensitivity was tested for five antifungal agents (Fluconazole, Voriconazole, Caspofungin, Amphotericin B and Itraconazole). The results were as follows: drug sensitivity to treatments (Caspofungin, Amphotericin B) and drug resistance to others.
While for Candida dubliniensis isolate, a VITEK 2 (BioMerieux) system was used to demonstrate drug sensitivity and was sensitive to drugs (Voriconazole, Amphotericin B, and Flucytosine).
Candida parapsilosis isolate showed sensitivity to drugs (Fluconazole, Voriconazole, Caspofungin, Micafungin, Amphotericin B, and Flucytosine).
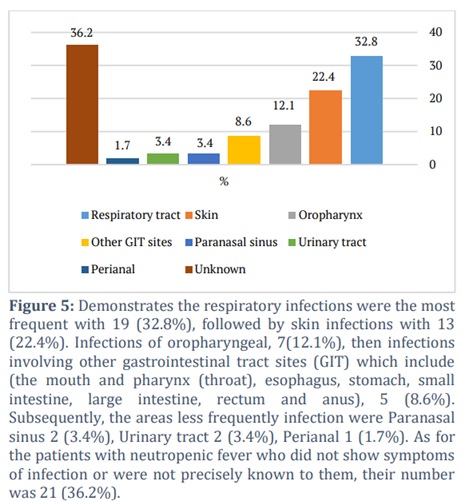
Site of infection
Fig 5 demonstrates the most common areas of infection among patients with hematological malignancies with neutropenic fever who are undergoing chemotherapy. Where the highest rate of infection was found in the respiratory system, followed by skin and soft tissues, and then the digestive system.
Figures & Tables
To effectively treat infections in patients with neutropenic fever, hematologic malignancies after receiving chemotherapy, it is critical to understand potential pathogens as well as local sensitivity patterns to antibiotics and antifungals in treatment centers.
Neutropenic fever is a single oral temperature of ≥38.3º C or a temperature of ≥38.0º C sustained for more than 1 hour in a patient with neutropenia. Bloodstream infection is a major cause of increased morbidity and mortality among neutropenic patients, who have hematologic malignancies. Both bacterial and fungal germs are associated with bloodstream infection among this type of patients [7, 10]
Gram-negative bacilli were the most common causative agents of BSI in patients with cancer and neutropenia in studies conducted worldwide during the 1960s and 1970s. Gram-positive cocci (30-70 %) predominated over the next two decades [11, 14]. In our hospital, where Gram-negative bacteria predominated, this substitution was not observed. It was found that the majority of infections causing pathogens were gram-negative bacteria (15.52%), followed by gram-positive bacteria (6.89%). Escherichia coli was the predominant isolate in general (13.8%), Klebsiella pneumoniae accounted for (1.7%), Staphylococcus hominis (coagulase-negative) (5.2%), followed by Staphylococcus aureus (coagulase-positive) (1.7%).). Similar to what was found in the Iranian research; gram-negative bacteria (63.3%) were detected more frequently than gram-positive bacteria (36.7%). Escherichia coli was the most common Gram-negative organism (47%), followed by coagulase-negative Staphylococcus (CoNs) and was the most common pathogen isolated among Gram-positive bacteria (54.6%)[15]. These Escherichia coli isolates showed different antibiotic susceptibility: Imipenem (75%), Meropenem (62.5%), Amikacin (83.3%), Gentamicin (62.5%), Tobramycin (50%), Fosfomycin (100%), and Nitrofurantoin (100%). These results were close to the Iranian research, which showed additional sensitivity to Tigecycline, while in our research; this sensitivity did not appear in Escherichia coli [16].
Klebsiella pneumoniae, was found in one case in a patient suffering from aplastic anemia at the age of 17 years, suffering from severe neutropenic fever. He died due to a bloodstream infection with Klebsiella pneumoniae, which showed resistance to all kinds of drugs according to the results shown by the drug sensitivity VITEK 2 (BioMerieux) system. Klebsiella pneumoniae is one of a few bacteria that have developed a high rate of antibiotic resistance due to changes in the organism's core genome [17].
Gram-positive bacteria, Staphylococcus hominis (coagulase-negative), and Staphylococcus aureus (coagulase-positive) have been found to cause infections in the bloodstream that can travel from the skin in their usual place to the blood in which they become pathogenic. Possible explanation may be due to the continuous use of intravenous catheters when the patient is undergoing a long course of chemotherapy or when experimental therapies are used in anticipation of possible infection in patients with neutropenia, as well as it can pass from the hands of hospital staff to the patient with neutropenia as he/ she suffers of weak immunity. This interpretation agrees with what was mentioned in a research that took place in Baghdad Teaching Hospital. Gram-positive bacteria responsible for microbiologically proven infections are responsible for 60-70% of infections. This percentage could be attributed to the widespread use of quinolones or the use of broad-spectrum antibiotics for empirical antimicrobial therapy for Gram-negative bacteria [18].
In our study, Staphylococcus hominis (coagulase- negative) was isolated from 3 cases. This bacterium was sensitive to the following antibiotics: Linezolid, Teicoplanin, Vancomycin, Tigecycline, Nitrofurantoin, Rifampicin, and Trimethoprim/Sulfamethoxazole.
Regarding drug sensitivity to Staphylococcus aureus (coagulase-positive), one case was sensitive to most drugs except for one treatment (Rifampicin).
This study also showed convergence in the results where, the majority of coagulase-negative staphylococci (94%) were susceptible to linezolid, and more than 80% were susceptible to (Teicoplanin, Rifampicin, Chloramphenicol and Vancomycin) [15]. A similar study was found to our results for Staphylococcus aureus , which showed sensitivity to most of the drugs used and no resistance to any treatment used (Gentamicin, Levofloxacin, Moxifloxacin, Erythromycin, Clindamycin, Vancomycin, Linezolid, Tetracycline, Tigecycline, Rifampicin, Trimethoprim/Sulfamethoxazole) [16].
Bacillus cereus, a Gram-positive facultative anaerobic bacterium, was isolated from only 1 case, a multiple myeloma patient. It is believed that infection of the bloodstream with this type of bacteria is due to the patient undergoing a long period of treatment. The infection may be from a central venous catheter or from having had abdominal surgeries, or from being infected by eating food, because immunocompromised due to chemotherapy or use much empirical antibiotics. This is consistent with research conducted in Switzerland; there were three cases of Bacillus cereus infection in the bloodstream from all 10 patients with blood diseases who had neutropenia at the time of infection. It is believed that the bloodstream sources were the intestinal tract (50%) and the central venous catheter (50%) [19, 20].
Three fungal isolates were also found in patients with neutropenic fever: Rhodotorula glutinis /mucilaginosa, Candida dubliniensis, and Candida parapsilosis.
One isolate of Rhodotorula glutinis / mucilaginosa, showed drug sensitivity to Caspofungin and Amphotericin B. This sensitivity was similar to a case report from Turkey [21].
Candida dubliniensis was isolated from a patient with acute lymphoblastic leukemia admitted to the intensive care unit suffering from neutropenic fever, and it was sensitive to Voriconazole, Amphotericin B, and Flucytosine. In a Korean study, a neutropenic man with multiple myeloma had a polymicrobial bloodstream infection with C. albicans and C. dubliniensis, from an infected central venous catheter, and these microbes were sensitive to Amphotericin B and Itraconazole [22].
Candida parapsilosis was isolated, which showed drug sensitivity to all drugs used in the test (Fluconazole, Voriconazole, Caspofungin, Micafungin, Amphotericin B, and Flucytosine). In a study conducted at the Catholic University of Rome, an increase in cases of Candida caused by C. parapsilosis was reported. It was found that candidiasis is the most common cause of candida infection in intensive care patients and patients with hematological malignancies. Drug sensitivity was tested against antifungal agents and exhibited sensitivity (Flucytosine, Fluconazole, Itraconazole, and Voriconazole) [23].
Regarding the site of infection in the scope of our study, 32.8% suffer from inflammation in the respiratory system. 22.4% have inflammation of the skin that may be in the soft tissues of the skin or ulcers in skin area. 12.1% suffer from infections, in the oropharynx. 8.6% infection in the gastrointestinal tract. 3.4% inflammation in the paranasal sinus, and 3.4% inflammation in the urinary tract.1.7% inflammation in the Perianal region, 36.2% in addition to the presence of cases suffering from neutropenic fever, but they did not show clear symptoms indicating the presence of inflammation or infection. What was found in our study was consistent with findings reported by Naji, et al. in a study he conducted on neutropenic patients suffering from malignant hematomas in Baghdad Teaching Hospital, in which it was found that 52% had respiratory gas infection, 18% urinary tract infection, 16% infection in the perianal area, 12% inflammation in the sinuses, 12% inflammation in the digestive system, 12% presence of inflammation in the skin, mucous membrane and canola sites, and 2% infection of the nervous system [18,10].
Neutropenic fever is a direct cause for morbidity and mortality of patients with hematological malignancies. About 65% of our patients were culture-negative; however, the use of Meropenem or Imipenem in combination with Aminoglycoside was effective in majority of cases. Early administration of broad-spectrum antimicrobials after obtaining a sample for blood culture is crucial in way of management.
C-reactive protein is a useful biomarker for diagnosis and prognosis as it could be a predictor for mortality.
Recommendation
Early diagnosis and management of patients with febrile neutropenia. Early obtaining of a blood sample for culture and sensitivity to ensure precise detection of microorganism and appropriate antimicrobial use. Underpin hygienic measures during medical care service to decrease transmission of nosocomial infections. Further evaluation and deeper analysis of culture-negative sample to help in detection of causative microorganisms.
Acknowledgement
The authors extend their appreciation to the Deputyship for Research & Innovation, “Ministry of Education” in Saudi Arabia for funding this research work through the project number (IFKSUDR_ F121).
Author Contributions
AKJ conceived the idea. HA designed the experiment and performed the experiments. All authors contributed to the article and approved the submitted version.
The authors declare that there is no conflict of interest.![]()
References
- Al‑Shammary, EH, Mohammed, DJ. Chemotherapy induced Neutropenia after Initial and Subsequent Chemotherapy Cycle of Non‑Hodgkin Lymphoma. Mustansiriya Medical Journal, (2020); 19(1): 16-16.
- Hidalgo A, Chilvers ER, Summers C, Koenderman L. The neutrophil life cycle. Trends in immunology, (2019); 40(7): 584-597.
- Krish P, Howard W. Febrile Neutropenia. JAMA Oncology, (2017); 3(12): 1751.
- Tahir N & Zahra F. Neutrophilia. (2021). Retrieved from https://europepmc.org/article/nbk/nbk570571, date [5/11/2024].
- Carvalho AS, Lagana D, Catford J, Shaw D, Bak N. Bloodstream infections in neutropenic patients with haematological malignancies. Infection, Disease & Health, (2020); 25(1): 22-29.
- Çalık Ş, Arı A, Bilgir O, Cetintepe T, Yis R, et al. The relationship between mortality and microbiological parameters in febrile. The relationship between mortality and microbiological parameters in febrile neutropenic patients with hematological malignancies. Saudi medical journal, (2018); 39(9): 878.
- Wright WF, Auwaerter PG. Fever and fever of unknown origin: review, recent advances, and lingering dogma. In Open forum infectious diseases, (2020); 7(5): ofaa132.
- Wingard JR. Treatment of neutropenic fever syndromes in adults with hematologic malignancies and hematopoietic cell transplant recipients (high-risk patientsUp To Date. (2018). Retrieved from https://www.uptodate.com/contents/treatment-of-neutropenic-fever-syndromes-in-adults-with-hematologic-malignancies-and-hematopoietic-cell-transplant-recipients-high-risk-patients, date [5/11/2024].
- Sahu C, Jain V, Mishra P, Prasad KN. Clinical and laboratory standards institute versus European committee for antimicrobial susceptibility testing guidelines for interpretation of carbapenem antimicrobial susceptibility results for Escherichia coli in urinary tract infection (UTI). Journal of laboratory physicians, (2018); 10(03): 289-293.
- Hadi DA. Study of Bacterial Infections and the Role of some Host Biomarkers in Early Detection among Febrile Pediatric Cancer Patients under Chemotherapy in Basrah Province- Iraq. University of Basrah. (2020).
- Fortún J, Sanz MÁ , Madero L, López J, de la Torre J, et al. Update on bacteraemia in oncology and hematology. Enfermedades Infecciosas Y Microbiología Clínica, (2011); 29: 48-53.
- Gudiol C, Bodro M, Simonetti A, Tubau F, González-Barca E, et al. Changing aetiology, clinical features, antimicrobial resistance, and outcomes of bloodstream infection in neutropenic cancer patients. Clinical Microbiology and Infection, (2013); 19(5): 474-479.
- Ruhnke M, Arnold R, Gastmeier P. Infection control issues in patients with haematological malignancies in the era of multidrug-resistant bacteria. The Lancet Oncology, (2014); 15(13): e606-e619.
- Trecarichi EM, Pagano L, Candoni A, Pastore D, Cattaneo C, et al. Current epidemiology and antimicrobial resistance data for bacterial bloodstream infections in patients with hematologic malignancies: an Italian multicentre prospective survey. Clinical Microbiology and Infection, (2015); 21(4): 337-343.
- Amanati A, Sajedianfard S, Khajeh S, Ghasempour, S, Mehrangiz S, et al. Bloodstream infections in adult patients with malignancy, epidemiology, microbiology, and risk factors associated with mortality and multi-drug resistance. BMC infectious diseases, (2021); 21(1): 1-14.
- Khodashahi R, Hakemi-Vala M, Mardani M, Abolghasemi S, Lotfali E, et al. Blood culture and antimicrobial susceptibility pattern of bacteria and fungi isolated from febrile neutropenic patients treated with chemotherapy at Taleghani hospital, Tehran. Iranian Journal of Microbiology, (2019); 11(2): 90.
- Ashurst JV, Dawson A. Klebsiella pneumonia, (2018). Retrieved from https://europepmc.org/article/nbk/nbk519004, [5/11/2024].
- Naji A, SarKo S, Atta S. Current Sites of Infections and Types of Microorganisms in Patient with Febrile Neutropenia in Hematological Wards–Single Center Study. Open Access Macedonian Journal of Medical Sciences, (2022); 10(B): 489-500.
- Tusgul S, Prod'hom G, Senn L, Meuli R, Bochud PY, Giulieri SG. Bacillus cereus bacteraemia: comparison between haematologic and nonhaematologic patients. New microbes and new infections, (2017); 15: 65-71.
- Jumaa AK, Al-Shammari HHJ, Qasim ZR. The Frequency and Spectrum of Bacterial Contamination of Packed Red Blood Cells and Platelet Concentrate Units from a Sample of Iraqi Blood Donors. ASM Science Journal, (2021); 15: 1-4.
- Ayaz CM, Gülmez D, Arıkan Akdağlı S, Uzun Ö. A Rare Yeast: Cases of Rhodotorula mucilaginosa Infection Followed Up in a Tertiary University Hospital [A Rare Yeast: Cases of Rhodotorula mucilaginosa Infection Followed Up in a Tertiary University Hospital]. Microbiology bulletin, (2021); 55(1): 91–98.
- Kim SH, Choi JK, Cho SY, Lee HJ, Park SH, et al. Risk factors and clinical outcomes of breakthrough yeast bloodstream infections in patients with hematological malignancies in the era of newer antifungal agents. Medical Mycology, (2018); 56(2): 197-206.
- Sun M, Chen C, Xiao W, Chang Y, Liu C, Xu Q. Increase in Candida parapsilosis candidemia in cancer patients. Mediterranean journal of hematology and infectious diseases, (2019); 11(1): e2019012.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0