

Full Length Research Article
Altered placental expression of genes related to Vitamin D Metabolism and their correlation with spiral artery remodeling in Preeclamptic Women
Pushpa Goswami*, Samreen Memon, Ikram Din Ujjan, Fahmida Gul
Adv. life sci., vol. 11, no. 4, pp. 756-760, November 2024
*– Corresponding Author: Pushpa Goswami (pushpa.goswami@lumhs.edu.pk)
Authors' Affiliations
[Date Received: 19/05/2024; Date Revised: 07/08/2024; Date Published: 15/10/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Several studies reveals the correlation of preeclampsia (PE) with low vitamin D (VD) level due to disturbed trophoblast invasion and failure of spiral artery remodeling. The metabolism of VD is regularized by it signaling molecules expressed by the placenta during pregnancy. Therefore, this study was designed to assess and compare the levels of VD and it signaling molecules in placentae from normotensive and preeclamptic pregnancies and their correlation with spiral artery remodeling.
Methods: This study was carried out at Department of Anatomy at Liaquat University of Medical & Health Sciences, Jamshoro after ethical approval on placentae of 122 parturients; 61 from normal and 61 from preeclampsia, data was collected on predesigned proforma and was analyzed on SPSS 23.
Results: The mean and standard deviation of maternal age, gestational age, and parity was 32.73±5.9 years, 37.3±3.6 weeks and 3±1 respectively. The wall thickness of SA and VD when compared in two groups found statically significant. Vitamin D signaling molecules were determined by immunostaining compared in two groups by applying Mann Whitney U test and Pearson’s correlation which reveals significant differences in preeclamptic versus controls.
Conclusions: Despite extensive research indicating a link between low levels of VD and its signaling molecules in the context of inadequate spiral artery remodeling, there is still a need for further investigation to fully understand the mechanisms underlying this association in preeclampsia.
Keywords: Preeclampsia; Remodeling; Spiral artery; Vitamin D; Vitamin D signaling molecules
Introduction![]()
Preeclampsia (PE) is a one of the pregnancies related hypertensive disorder, with highest fetomaternal morbidity and mortality globally. It is also associated with increased risk of heart diseases in advanced age as well. PE is defined as a new onset of hypertension with proteinuria, without proteinuria, it is manifested by functional impairment of vital organs; liver, kidneys and brain. It occurs after 20 weeks of pregnancy, more often near term [1, 2].
Even though considerable research on PE pathophysiology, its exact cause is still obscure. Although development of PE is closely linked with defective placentation resulting in uteroplacental insufficiency which in turn leads to oxidative stress and endothelial dysfunction, as disease advances it is manifested by clinical symptoms. The only available treatment of PE is removal of placenta by termination of pregnancy supports the notion of PE is a placental induced disorder [3].
Various studies reveal the strong correlation of PE development with vitamin D deficiency (VDD). Despite of unclear role of VD and pregnancy related comorbidities including PE, VD supplementation during pregnancy is recommended by many healthcare personals due to its deficiency globally among pregnant women [4, 5].
The placental expression of VD signaling molecules i.e. vitamin D receptor (VDR), vitamin D binding protein (VDBP), 25-hydroxylase (CYP2R1), 1α-hydroxylase (CYP27B1) and 24-hydroxylase (CYP24A1) ensures efficient VD metabolism during pregnancy. The mechanism of metabolism of placental VD and its impact on maternal circulation is still obscure. Regardless of unknown mechanism, various alterations in circulating concentrations of VD metabolites are observed in pregnancy for example, levels of circulating VD and VDBP rise by two folds in pregnancy. Substantial rise of CYP27B1 and VDR is observed in first half of normal pregnancy in placenta [6, 7].
In normal pregnancy uterine spiral arteries (SA) undergo physiological remodeling, by invasion of trophoblast, for proper placental development. Several studies also reveal the role of VD in this process via mechanism, which is still unknown precisely. These changes transform SA from smaller diameter and high resistance vessels to larger, dilated, funnel shaped vessels, ensuring adequate uteroplacental circulation. In PE abnormal remodeled vessels are frequently observed, contributing strikingly in uteroplacental insufficiency and negative consequences [8].
Considering the above observations, we postulated that expression of VD and it signaling molecules are altered in PE and contribute to its pathogenesis by abnormal SA remodeling. Therefore, present study was designed to evaluate and compare the VD signaling molecules; VDR, VDBP, CYP2R1, CYP27B1, and CYP24A1 in placentae from normotensive and preeclamptic pregnancies and their correlation with VD level and spiral artery remodeling.
Methods![]()
Patients:
This study was conducted in Department of Anatomy, Liaquat University of Medical and Health Sciences (LUMHS), Jamshoro. A total of 122 pregnant women with pregnancy of more than 36 weeks and one alive fetus, 61from normal as controls and 61 from preeclampsia from maternity ward. The sample size was calculated with prevalence-based formula using Epitools epidemiological calculator (Available at: http://epitools.ausvet.com.au.) and the sampling technique was purposive non-probability [9].
Assessment of Vitamin D:
Maternal Vitamin D was assessed on sample of 5cc drawn before delivery by chemiluminescence micro particle immunoassay (CMIA) at Diagnostic and Research Laboratory (D&R), LUH [10].
Placental tissue sampling:
Placentae were collected with 5cm of umbilical cord away from its site of insertion immediately after normal vaginal or caesarian section delivery. Placental membranes were trimmed after washing with phosphate saline buffer (PBS). A morphological examination of placenta was performed then each placenta was sectioned into two halves with sterile blade. Two sections of placental tissue (2x2x1 cm) were excised randomly and fixed in 10% formalin for 48 hours after labeling and processed in D&R, LUH at Hyderabad [11].
Tissue processing for Microscopy:
Formalin fixed paraffin embedded tissue (FFPE) was processed by automatic tissue processor, (Leica TP1020) and sectioned on rotatory microtome, placed on Amino-propyl-tri-ethoxy-silane coated slides (APEC) for staining [12].
Hematoxylin and Eosin staining:
After deparaffinization in xylene and rehydration in graded alcohol, were stained with hematoxylin for 3 minutes, then by eosin for half an hour after washing. After washing slides were dehydrated with graded alcohol and mounted with DPX [13].
Immunohistochemistry (IHC) staining of VD signaling molecules:
Vitamin D signaling molecules; VDR, VDBP, CYP2R1, CYP27B1 and CYP24A1 were assessed by immunostaining. The FFPE tissue sections of 5 μm thickness were processed on standard (IHC) staining procedure. Concisely, sections were dewaxed in xylene and rehydrated through a series of ethanol. Antigen unmasking was performed with Tris HCl in steamer then washing with PBS three times. Endogenous peroxidase activity was blocked with 3% hydrogen peroxide. After cooling for 30 minutes, tissue sections were incubated with the primary antibodies. Primary antibodies were diluted in PBS; VDR (1:500 dilutions), VDBP (1:200 dilutions), CYP27B1 (1:750 dilutions), CYP2R1 (1:750 dilutions), and CYP24A1 (1:500 dilutions) were applied with pipette in marked area of slide and incubated for an hour. After washing thrice with PBS, secondary antibody (Horseradish peroxidase) was applied and kept for half hour in dark. Diaminobenzidine (DAB) was applied for 05 minutes, followed by washing in PBS thrice. Sections were counterstained with hematoxylin and dried and mounted with Dibutyl phthalate Polystyrene Xylene (DPX) for nuclei before microscopy [14, 15].
Microscopy and imaging:
Slides were observed at 20X and 40X magnification; images were saved as jpeg files. The wall thickness of spiral arteries was observed on H&E stained slides. The wall thickness of SA was calculated by measuring difference in external diameter and internal diameter of the SA on image J software (version 1.46r). Immunostained cells were counted on image J to count IHC positive DAB stained brown & IHC negative hematoxylin-stained blue nuclei obtained results were saved for analysis [16].
Data analysis:
Data was analyzed using the Statistical Package of Social Sciences (SPSS) IBM, SPSS version 23.0. The numerical data was presented as mean and standard deviation. Distribution of data was measured by normality (Shapiro-wilk) test. Normally distributed numerical data is compared by applying independent t test while not normally distributed is compared by applying Mann Whitney U test. Numerical variables were correlated with each other by applying Pearson correlation. Results were considered significant when p < 0.05 in all analyses [17].
Results![]()
The mean and standard deviation of maternal age, gestational age, and parity was 32.73±5.9 years, 37.3±3.6 weeks and 3±1 respectively. The remodeling of spiral artery was assessed by mean wall thickness of spiral arteries was 38.11µm, when compared in two groups found statically significant (table1). Vitamin D is found to be deficient in both groups, but the preeclamptic parturient shows significant deficiency when compared with controls (table1).
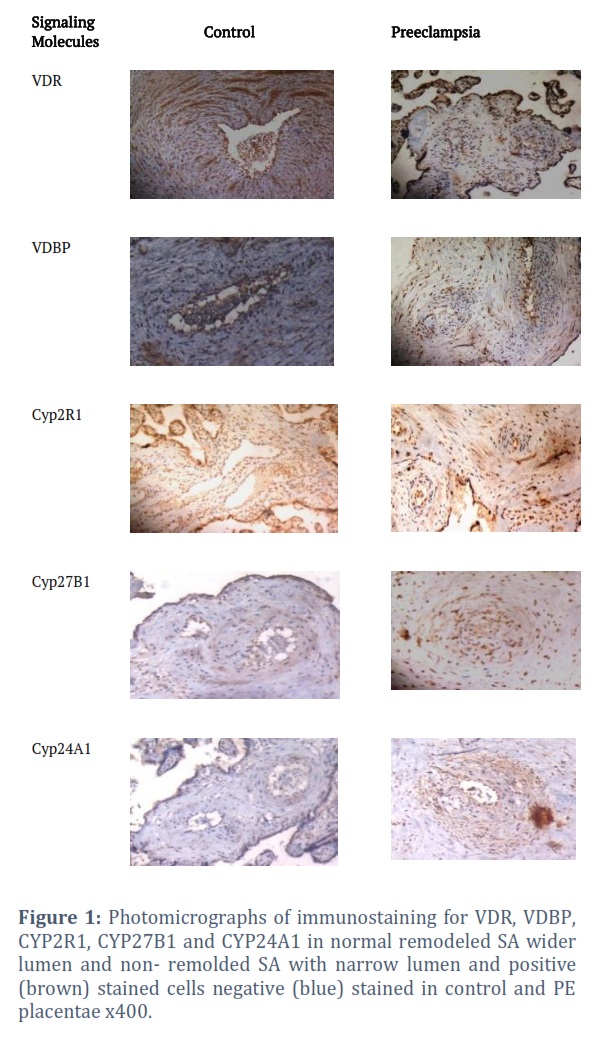
The vitamin D signaling molecules; VDR, VDBP, CYP2R1, CYP27B1 and CYP24A1 when compared in two groups by applying Mann Whitney U test which reveals substantial differences in preeclamptic versus controls (table 2).
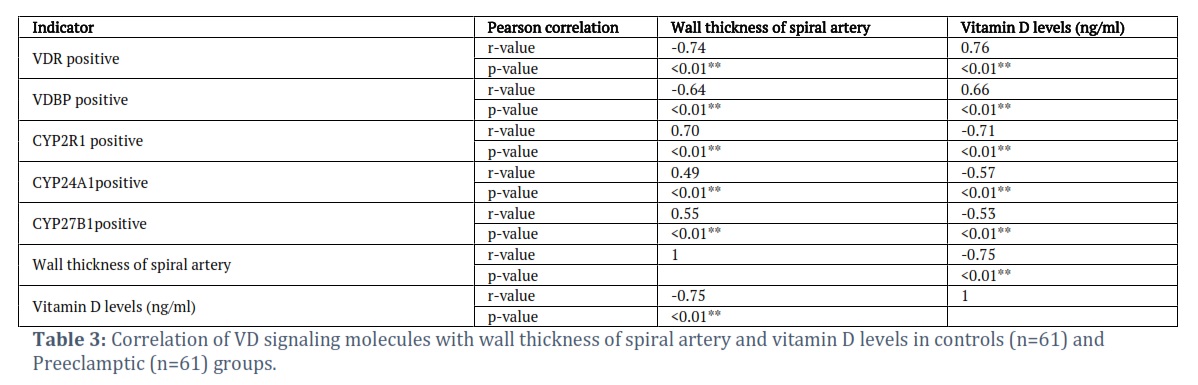
Pearson’s correlation of VD signaling molecules with wall thickness of spiral artery and VD reveals VDR positive and VDBP positive are negatively correlated with spiral artery thickness and positively correlated with levels of VD. While CYP24A1, CYP2R1 and CYP27B1 are positively correlated with spiral artery thickness and negatively correlated with VD levels. Wall thickness of spiral arteries and vitamin D level are also negatively correlated with each other shown in (table 3).
Figures & Tables


Placenta is the most vital organ of pregnancy, growing concurrently with embryo and fetus with significant impact on its development. Thus, meticulous studies of placenta are helpful in understanding the pathogenesis of placenta related pregnancy disorders common most PE [18].
The positive correlation of VDD with PE was observed by the wall thickness of spiral artery. In this study we found a significant difference in wall thickness in controls versus PE. These findings are in line with studies conducted in Pakistan by Hamza and Baloch et al with difference in methodology [19, 20].
Vitamin D acts as a moderator of genes required for placental development, suggestive of strong association of VDD and development of PE by several studies. This study also reveals the significant difference of VD level in controls and preeclamptic, similar findings are reported by Sana Shahid. Another Study conducted by Murat and Salih in Turkey also reports significant difference in normotensive and preeclamptic similar to this study [21, 22].
Placenta produces all VD signaling molecules and altered levels of VD and it signaling molecules were observed in PE placentae when compared with controls. This study reveals significant lower levels of VDR in PE which is similar with study by Hutabert although their methodology was semiquantitative. While Xiao et al. observed higher placenta VDR mRNA expression and low VD in women with PE versus controls, assumed by authors as compensatory mechanism of placenta for VDD [23, 24].
Low level of VDBP is reflector of low levels of VD in PE placentae. This study reveals higher levels of VBPB in normotensive versus PE on immunostaining, which is in coherence with immunostudy conducted by Ma et al [25].
CYP2R1 and CYP27B1 are hydroxylases which convert cholecalciferol to an active form of VD. Alterations in expression of these hydroxylases alter the levels of VD. CYP2R1 in the liver converts calciferol to calcidiol and CYP27B1 in kidneys convert calcidiol to calcitriol. In pregnancy placental expression of these hydroxylases increases levels of VD for several functions. This study reveals higher expression of both gene proteins in PE placentae as compared with controls similar is reported by Justyna Magiełda, although we concluded on immunohistochemistry while Justyna studied on quantitative real time PCR. The study conducted by Ghorbani on genotypes of CYP27B1 also reveals two folds raised levels in PE placentae when compared with normal [26, 27].
While study conducted by Ma et al found CYP2R1 proteins lower in PE contrary to our study, although CYP27B1 is higher in PE similar to this study. Inconsistent results were expected as an effect of oxidative stress on metabolism of VD in with PE where reduction of CYP2R1 is supposed to be overruled by increase of CYP27B1. CYP24A1 is the major catabolizing protein which converts calcitriol into calcitroic acid inactive form of VD to prevent its toxicity. We reveal lower expression of CYP24A1 in controls and higher in women with PE. Rong Ma also reported the same suggestion of increased degradation of VD in PE by mechanism still uncertain [25].
This is the first study examining the correlation between PE and VD and its signaling molecules, with remodeling of the SA in the local population. We found that low levels of VD and signaling molecules hinder the process of SA remodeling, contributing to the pathogenesis of preeclampsia; hence, the role of VD in preventing PE is essential. Therefore, VD may be supplemented to prevent PE by enhancing spiral artery remodeling.
Acknowledgements
This study is funded by Liaquat University of Medical and Health Sciences, Jamshoro, Sindh, Pakistan.
Author Contributions
Pushpa Goswami: Data collection and interpretation and drafting of the manuscript. Corresponding author
Samreen Memon: Concept and design, in-charge of data collection, final approval of the manuscript.
Ikram Din Ujjan: Critical review and approval of manuscript
Fahmida Gul: Data collection and assembly of data
The author declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- McDonald SD, Malinowski A, Zhou Q, Yusuf S, Devereaux P. Cardiovascular sequelae of preeclampsia/eclampsia: A systematic review and meta-analyses. American Heart Journal, (2008); 56: 918–930.
- ACOG. ACOG Practice Bulletin No. 202: Gestational Hypertension and Preeclampsia. Obstetrics and Gynecology, (2019); 133:e1–e25.
- Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy F, et al. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Hypertension, (2018); 72:24-43.
- Poniedziałek CE, Mierzyński R. Could Vitamin D Be Effective in Prevention of Preeclampsia? Nutrients, (2021); 13(11):3854.
- Akbari S, Khodadadi B, Ahmadi SA, Abbaszadeh S, Shahsavar F. Association of vitamin D level and vitamin D deficiency with risk of preeclampsia: A systematic review and updated meta-analysis. Taiwan Journal of Obstetrics and Gynecology, (2018); 57: 241–247.
- Pike JW, Meyer MB. Fundamentals of vitamin D hormone-regulated gene expression. The Journal of steroid Biochemistry and Molecular Biology, (2014); 144: 5-11.
- Wei SQ, Audibert F, Hidiroglou N, Sarafin K, Julien P, et al. Longitudinal vitamin D status in pregnancy and the risk of pre-eclampsia. British Journal of Obstetrics and Gynecology, (2012); 19 (7): 832-839.
- Zhang JY, Wu P, Chen D, Ning F, Lu Q, et al. Vitamin D Promotes Trophoblast Cell Induced Separation of Vascular Smooth Muscle Cells in Vascular Remodeling via Induction of G-CSF. Frontiers in Cell and Developmental Biology,(2020) 8:601043. doi: 10.3389/fcell.2020.601043
- Ezeigwe CO, Okafor CI, Eleje GU, Udigwe GO, Anyiam DC. Placental Peripartum Pathologies in women with Preeclampsia and Eclampsia. Obstetrics and Gynecology International, (2018): 9462938. doi: 10.1155/2018/9462938.
- Diagnostics R (2011). Package insert for vitamin D total (25-Hydroxyvitamin D) quantitative determination. Sandhofer Strasse 116, D- 68305
- Goswami P, Lata H, Memon S, Khaskhelli LB. Excessive Placental Calcification Observed in PIH Patients and its Relation to Fetal Outcome. Journal of Liaquat University of Medical and Health sciences, (2012); 11(3): 144-148.
- Chlipala E, Bendzinski CM, Chu K, Johnson JI, Brous M, et al. Optical density-based image analysis method for the evaluation of hematoxylin and eosin staining precision. Journal of histotechnology, (2020); 43(1): 29-37.
- Feldman AT, Wolfe D (2014). Tissue processing and hematoxylin and eosin staining. Methods in molecular biology 1180: 31-43.
- Hou H, Zhang J,Y, Chen D, Deng F, Morse A.N, Qui X et al. Altered decidual and placental catabolism of vitamin D may contribute to the etiology of spontaneous miscarriage. Placenta, (2020); 92:1–8.
- Schacht V, Kern JS. Basics of immunohistochemistry. The Journal of investigative dermatology, (2015); 135(3): 1-4.
- Fulawka. L, H. Proliferation index evaluation in breast cancer using imagej and immunoratio applications. Anticancer research, (2016); 36: 3965-3972.
- Knabl J, Huttenbrenner R, Hutter S, Gunthner-Bille M, Riedel C, et al. Gestational Diabetes Mellitus up regulates Vitamin D receptor in extravillous trophoblasts and fetoplacental Endothelial Cells. Reproductive Sciences, (2015); 22(3): 358-366
- Madan A, Kaur K, Shergill HK, Neki NS. The Morphological and Histopathological changes in placenta in hypertensive pregnant mothers – A Prospective study. International Journal of current Research in Biology and Medicine, (2018); 3(3): 75-81.
- Hamza S. Complication of gestational preeclampsia and the differences between tunica media and internal area of spiral artery by image J. Pakistan Journal of Medical and Health Sciences, (2021);15(3): 1093-1097.
- Baloch GKR, Khan BW, Siddiqui RA, Borges KJJ, Shah SNN, et al. Quantitative morphometric analysis of uterine spiral artery in normal and preeclamptic placentae via fluorescence microscopy. Journal of Peoples University of Medical and Health Sciences, (2021); 01: 73-79.
- Shahid S, Ladak A, Fatima SS, Zaidi F, Farhat S. Association of vitamin D levels with preeclampsia. Journal of Pakistan Medical Association, (2020); 70(12): 2390-2393.
- Bakacak M, Serin S, Ercan O, Köstü B, Avci F, et al. Comparison of Vitamin D levels in cases with preeclampsia, eclampsia and healthy pregnant women. International Journal Clinical and Experimental Medicine,(2015);8(9):16280-6.
- Hutabarat M, Wibowo N, Obermayer-Pietsch B, Huppertz B. Impact of vitamin D and vitamin D receptor on the trophoblast survival capacity in preeclampsia. PloS one, (2018); 13(11): e0206725.
- Xiao JP, Lv JX, Yin YX, Jiang L, Li,WS, et al. Lower maternal and fetal vitamin D status and higher placental and umbilical vitamin D receptor expression in preeclamptic pregnancies. International Journal of Clinical and Experimental Pathology, (2017); 10: 10841–10851.
- Ma R, GuY, Zhao S, Sun J, Groome L J, WangY. Expressions of vitamin D metabolic components VDBP, CYP2R1, CYP27B1, CYP24A1, and VDR in placentas from normal and preeclamptic pregnancies. American Journal of Physiology, Endocrinology and Metabolism, (2012); 303(7): E928-935.
- Magiełda-Stola. J, Kurzawińska. G, Ożarowski. M, Bogacz. A, Wolski. H, Drews. K, et al. Placental mRNA and Protein Expression of VDR, CYP27B1 and CYP2R1 Genes Related to Vitamin D Metabolism in Preeclamptic Women. Applied Sciences, (2021); 11(24): 11880.
- Ghorbani Z, Shakiba M, Rezavand N, Rahimi Z, Vaisi-Raygani, et al. Gene variants and haplotypes of Vitamin D biosynthesis, transport, and function in preeclampsia. Hypertension in Pregnancy,(2021); 40: 1-8.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0![]()