

Full Length Research Article
Risk factors for Beta-lactam and carbapenem-resistant bacteria causing post-burn infections
Muhammad Hayat Haider1, Amina Akram2,3, Maira Nasir1, Rehan Ahmad Khan Sherwani6, Muhammad Umair Shareef3, Muhammad Nauman Ali3, Saba Riaz1,4,5*
Adv. life sci., vol. 11, no. 4, pp. 733 -740, November 2024
*– Corresponding Author: Irina S. Agasyeva (irina-agasyeva@mail.ru)
Authors' Affiliations
2. Ameer-ud-Din Medical College/Post Graduate Medical Institute, Lahore – Pakistan
3. Jinnah Burn and Reconstructive Surgery Centre, Jinnah Hospital, Lahore – Pakistan
4. Citilab and Research Centre, 525-A Faisal Town Lahore – Pakistan
5. Centre for Clinical Microbiology, University College London – United Kingdom
6. College of Statistical and Actuarial Sciences University of the Punjab, Lahore – Pakistan
[Date Received: 11/12/2022; Date Revised:11/10/2023; Date Published: 15/10/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Burn patients are predisposed to infection because of the loss of skin barrier protection and low immunity. This study aims to evaluate the risk factors of post-burn infections due to beta-lactam and carbapenem-resistant bacteria (CR) isolated from a major burn unit.
Methods: The descriptive study was conducted at Jinnah Hospital Lahore’s Burn and Reconstructive Surgery Centre (JB & RSC) and the Institute of Microbiology and Molecular Genetics (MMG), University of the Punjab, Lahore. The clinical specimens of wound swabs, including the age, gender, socio-economic status, residence, occupation, hospital stay, wards, burn degree, total burnt surface area (TBSA%), etiology of burn, and other factors were recorded. Antimicrobial susceptibility testing (AST), ESBL and CR screening (Beta- lactam and carbapenem resistant bacteria) were performed using CLSI guidelines 2017.
Results: The most dominant strain was Pseudomonas spp. 26.5% (n=106), followed by 15% (n=60) Klebsiella spp., and 7.5% (n=30) Acinetobacter spp. with ESBL-producing strains. Compared to nosocomial infections, community-acquired infections were observed in 314 (78.5%) patients with more ESBL production. There was a significant relation between burnt people having an age of ≤ 29 years with ESBL (p=0.985) and carbapenemases (p=0.694) infections. None of the other factors, like low socioeconomic status and more hospital stays had a significant correlation (p > 0.05).
Concluded: It has been concluded that MDR gram-negative strains play a serious role in burn infections and demand suitable methods to decrease their number. Pseudomonas spp. was the most common post-burn infection causing bacteria. Unfortunately, a high frequency of burn infections was observed in the patients at a young age.
Keywords: Post burn infections; Gram negative; MDR; Beta- lactam; Carbapenem resistant
Introduction![]()
The most common cause of death in burn patients is post-burn-infections. In China, almost 38.7% of burn deaths were caused due to systemic infection. Burn patients are more exposed to infection because of less immunity and skin barrier removal. The infection is recognized by physical examination, infection biomarker detection and microbiological culture. Infection is controlled by using antibiotics and wound care. Burn infection is directly related to burning seriousness, like burn area, burn depth, inhalation injury, and burn severity scores. Therefore, multiple infection control and treatment methods should be employed with severe and non-severe burn patients [1-2]. Viruses, fungi, Gram-positive and Gram-negative bacteria (GN) are equally known to cause burn infections. But GN organisms pose a significant threat due to their multidrug resistance (MDR) nature and pathogenic factors [3-4]. Due to longer hospitalization duration, burn patients are prone to infection. Clinically significant MDR includes bacteria extended-spectrum-resistant Enterobacterales, carbapenem-resistant Enterobacterales (CRE), and MDR non-lactose-fermenting GN bacteria, such as Pseudomonas spp., Stenotrophomonas maltophilia, and Acinetobacter baumannii [4]. These clinical pathogens slow down the improvement in burn patients and lower their immune system. Besides Pseudomonas spp., Acinetobacter spp., are also evolving among burn infections in Iran [5]. The anatomical changes in burn patients depend on time and other factors like area, depth of the burn, time after burn, presence of infection, amount of moisture and level of serum proteins. When the fluid volume increases, it decreases the volume of drug distribution when a standard amount is allowed. The enhanced renal blood flow may cause more drug elimination and shorter clearance half-life. Infections are still responsible for 46-51% of deaths due to multi-organ failure, even though much care is taken of burn patients [6]. The World Health Organization (WHO) recorded approximately 200,000 deaths every year due to burns across the globe. The majority of these deaths have occurred in African regions. Here the death rate in children below age five is more. In Tanzania, a community-based study showed 16.3% of injuries were due to burns. In Iraq, the study reported a 37.7% relationship between wound infections and deaths. The common cause behind deaths was the misuse of antibiotics, followed by the infection that led to death. Further studies demonstrated post-burn infection as a prominent cause of death in Mozambique and Cameroon burn units [3]. A study in Korea reported a high frequency of cases associated with CRE [7].
Methods![]()
Study design
This cross-sectional study has been conducted in the Jinnah Burn and Reconstructive Surgery Centre (JB&RSC), Institute of Microbiology and Molecular Genetics (MMG), University of the Punjab, Citi Lab and Research Centre Lahore, Pakistan. The study was approved by the Ethical Review Board (ERB) of Allama Iqbal Medical College (AIMC) & Jinnah Hospital Lahore in its 40th meeting in August 2017. The clinical specimens were removed from this study that did not grow after 24-48 hours of incubation. The bacteria that were sensitive towards cephalosporins were excluded, whereas Beta-lactam and carbapenem-resistant GN bacteria were included in the study.
Sampling and data collection
All patient’s samples were taken since the time of admission recommended by the clinical officer. The purposive non-probability method was used for sampling from indoor/outdoor burn wards and intensive care units (ICU). The study recruited 400 bacterial strains from August 2018 to July 2020. A data form was designed to extract the following data: Demographic data (age, gender), clinical features (burn etiology, burn degree, TBSA%, sample sources, microbe type and antimicrobial resistance data.
Bacterial isolation and identification
All post burn samples were collected according to Standard Operating Procedure of hospital burn unit with the support of duty nurse and medical officer. After the collection of samples, these specimens were placed in trypticase soy broth (TSB) and transported to the Microbiology Laboratory (JB&RSC) for clinical processing. For the isolation of bacteria, the aerobic culturing method was utilized. After 24 hours of incubation at 37°C, the Blood agar and MacConkey’s agar were inoculated with specimens. Initially, identification of bacterial isolates was observed by colonial morphology, pigmentation, and changes in physical appearance in differential media and Gram stain reaction according to API-20E kit system (Bio-Merieux, France).
Antibiotics Susceptibility Testing (AST)
Antibiotic susceptibility testing of bacterial isolates was performed on Mueller Hinton agar by Kirby Bauer’s disc diffusion method according to Clinical Laboratory Standards Institute (CLSI) guidelines 2017 [8] Antibiotics tested were including (OXOID) penicillin’s [(piperacillin (PIP 100 µg), (amoxycillin/clavulanate (AMC 40 µg), ampicillin-sulbactam (SAM 10/10 µg), piperacillin-tazobactam (TZP 110 µg)], monobactams (aztreonam (ATM 30 µg)], cephalosporins [(ceftazidime (CAZ 30 µg), cephradine (CE 30 µg), cexime (CFM 30 µg), cefoperazone (CFP 30 µg), cefoperazone-sulbactam (SCF 110 µg), cefotetan (CN 100 µg), cefprozil (CPR 30 µg), ceftriaxone (CRO 30 µg), cefotaxime (CTX 30 µg), cefuroxime (CXM 30 µg), cefoxitin (FOX 30 µg), cefazolin (KZ 30 µg)], carbapenems [(doripenem (DOR 10 µg), ertapenem (ETP 10 µg), imipenem (IMI 10 µg), meropenem (MEM 10 µg)], aminoglycosides [(amikacin (AK 30 μg), gentamicin (GEN 30 μg), tobramycin (TOB 30 µg)], glycylcycline [(tigecycline (TGC 15 µg)], macrolide [(erythromycin (ERY 15 µg)], peptides [(polymyxin B (PB 10 µg), colistin (PE 10 µg)], fluoroquinolones [(ciprofloxacin (CIP 10 µg), (levofloxacin (LEV 5 µg), norfloxacin (NOR 10 µg), ofloxacin (OFL 10 µg)], quinolones [(nalidixic acid (NAL 30 µg)], and tetracyclines [(doxycycline (DC 30 µg), tetracycline (TET 30 µg)] [9].
Phenotypic screening of extended-spectrum β-lactamases (ESBLs)
The confirmatory tests for ESBLs detection as Double disk synergism test (DDST) and combination disc test (CDT) were performed for all study strains. ESBLs-producing isolates were screened on Mueller-Hinton’s (MH) agar by Kirby Bauer’s disk diffusion method, as previously reported by Chen et al [10].
Statistical analysis
For statistical analysis, Statistical Package for Social Sciences (SPSS) version 23 was utilized. The demographic characteristics were expressed in the form of the percentage value in the descriptive analysis. Continuous variables such as age and TBSA % were resolved by standard deviation (mean ± SD) values. Chi-square test and probability values were used to examine the association of risk factors with the type of infection (MDR/Non-MDR). The level of statistical significance was p-value < 0.05.
Results![]()
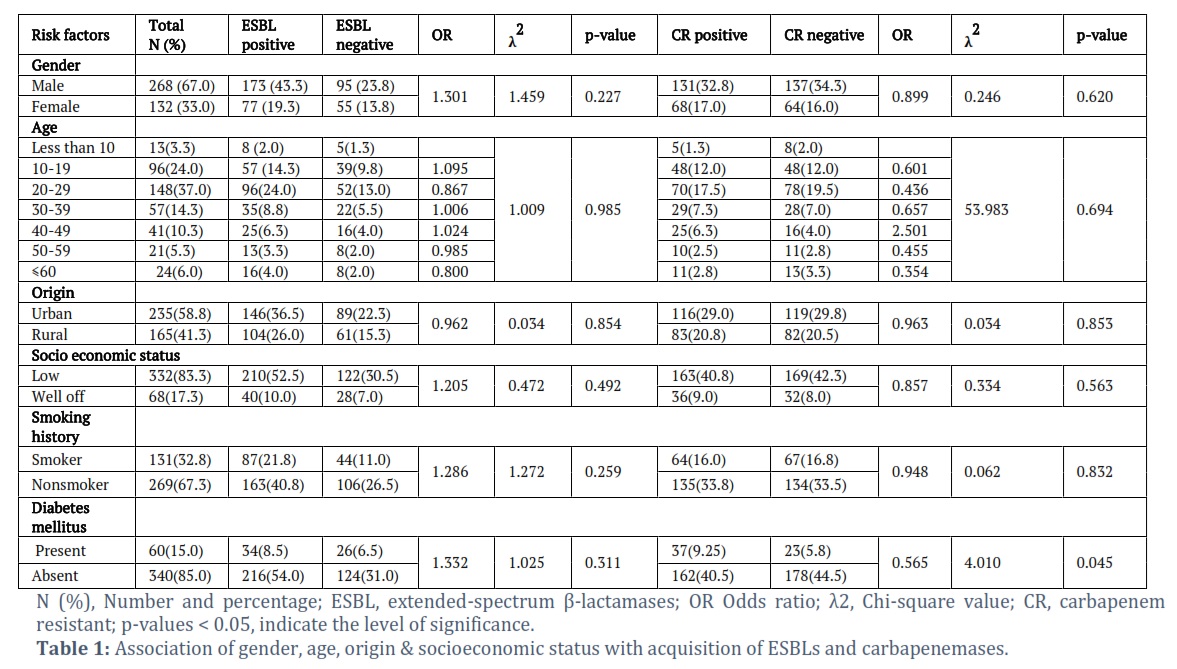
A total of 400 cultures were proceeded during two years of study to assess the risk factors associated with ESBLs and Carbapenemases producing bacterial infections in burn patients. Burn infections were common in males 268 (67.0%) than females 132 (33.0%). Young adults (20-29 years) and people from urban areas were predominantly infected with percentages of 48 (37.0%) and 235 (58.8%), respectively. Most burn infections suffered by 332 (83.3%) belonged to low socio-economic status. Cases of non-smokers and non-diabetic patients were high in number (Table 1). In hospitalization factors, indoor patients 255 (63.8%) with intravascular lines intubation 191 (47.8%) were dominant. The infection rate was high due to delay in hospital admissions after burn injury 227 (56.8%). Hospital stays of less than one week increased the patients’ survival rate 170 (42.5%) and 386 (96.5%) respectively. Among burn parameters, there were most cases that had second burn degree, TBSA (Less than 10%), Flame burns and Non-occupational Types of injury 160 (40.0%), 193 (48.3%), 185 (46.3%) and 287 (71.8%) respectively. Most of the bacteria were isolated from wound swabs 304 (76.0%). Three main isolates were Pseudomonas aeruginosa, Klebsiella pneumoniae and Acinetobacter baumannii 167 (41.8%), 99 (24.8%) and 52 (13.0%).
Burn patients related factors
For ESBLs production, rates of infections were high in males 173 (43.3%) than females 77 (19.3%). Burn injuries were more common in young individuals 96 (24%) aged between 20 and 29 years. There were 146 (36.5%) patients from urban areas and 104 (26.0%) rural areas A total of 400 cultures were proceeded during two years of study to assess the risk factors associated with ESBLs and Carbapenemases producing bacterial infections in burn patients. Burn infections were common in males 268 (67.0%) than females 132 (33.0%). Young adults (20-29 years) and people from urban areas were predominantly infected with percentages of 48 (37.0%) and 235 (58.8%), respectively. Most burn infections suffered by 332 (83.3%) belonged to low socio-economic status. Cases of non-smokers and non-diabetic patients were high in number (Table 1). In hospitalization factors, indoor patients 255 (63.8%) with intravascular lines intubation 191 (47.8%) were dominant. The infection rate was high due to delay in hospital adm, who had ESBLs infections. Burn patients of lower or poor socio-economic backgrounds, 210 (52.5%) had more ESBLs associated wound infections compared to the infections in well-off patients 40 (10%). The proportion of infected patients with diabetes 60 (15.0%) was low. No parameter was evaluated in correlation with acquiring antimicrobial resistance (p > 0.05). Carbapenemases screening revealed male patients 131 (32.8%) having age group of 20-29 years 70 (17.5%) were with a higher frequency as compared to other age groups. Most of the patients were from rural areas at 83 (20.8%) and poor socio-economic backgrounds 163 (40.8%). Few patients infected have diabetes 37 (9.25%) and smoking history. Diabetes mellitus was notably associated with the carbapenemases producing strains isolated from burn patients (Table 1).
Hospital associated factors
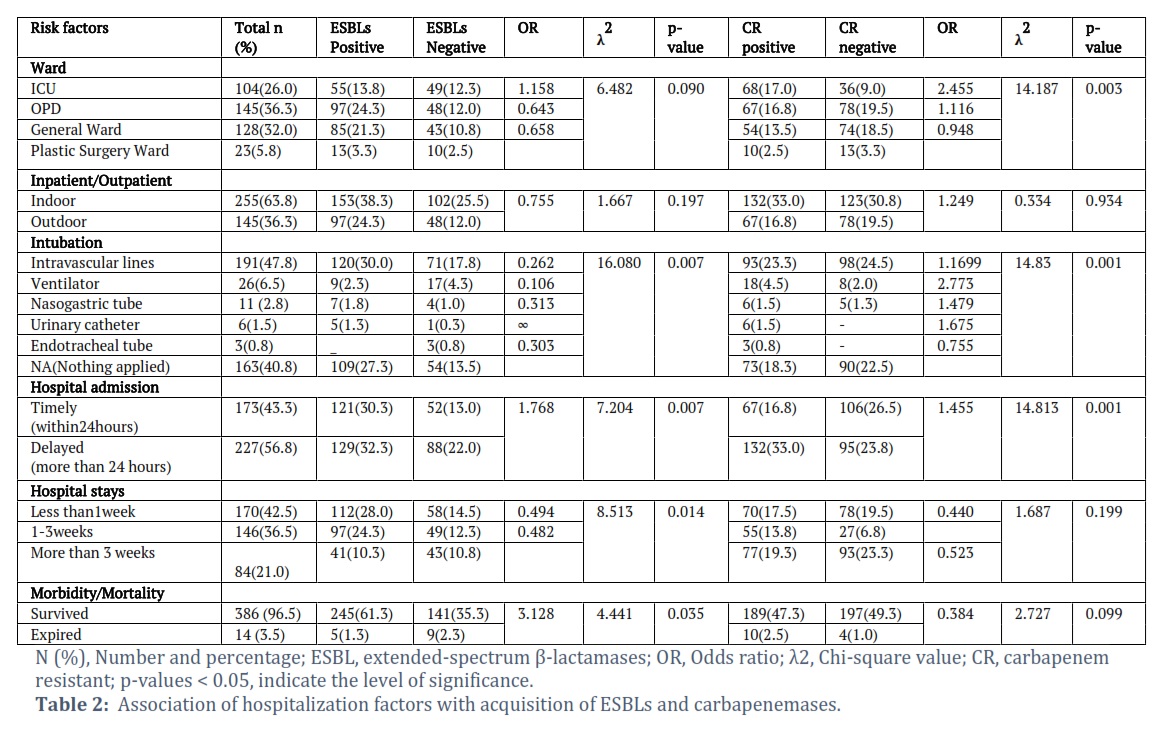
There was a large proportion of burn injuries in OPD 97 (24.3%) and indoor 153 (38.3%) in ESBLs infected group that were not significantly associated with ESBLs infections. ESBLs positive strains isolated from patients with intravascular lines were 120 (30%). There were 129 (32.3%) patients with ESBL-producing strains admitted after a delay of more than 24 hours. Hospital-associated factors were strongly associated with ESBLs-producing strains, including the use of intravascular lines 120 (30.0) (λ2=16.1, p=0.007), more than 24 hours delay in hospital admission 129 (32.3) (λ2=7.2, p=0.007), and more extended hospital stay for the treatment 41 (10.3) (λ2=8.5, p=0.014). There were 132 (33%) indoor burn patients and 67 (16.8%) patients in OPD wards infected with carbapenemase-positive strains. There were 68 (17%) ICU patients, 54 (13.5%) general ward, and 10 (2.5%) plastic surgery ward patients. In intubation methods, carbapenemase-producing strains were mostly isolated from patients applied with intravascular lines.
Ventilators were used for 26 (6.5%) patients, where 18 (4.5%) were infected with carbapenemase-positive strains. Carbapenemase production was observed in 132 (33%) patients admitted after a delay of more than 24 hours. There were 77 (19.3%) burn patients infected with carbapenemase-positive strains having a hospital stay of more than three weeks. The death rate was 14 (3.5%). Hospital-associated factors were remarkably associated with carbapenemase production, including ICU treatments (λ2=14.187, p=0.003), administering the intravascular lines (λ2=14.831, p=0.001), and delayed hospital admission (λ2=14.813, p=0.001) in burn patients (Table 2).
Burns-associated factors
ESBLs producing isolates from first-degree burn patients were 106 (26.5%). In 123 (30.8%) patients having ESBL infection, the TBSA was less than 10%. The major source of burns was flame observed in 116 (29%) patients with ESBLs infections. Mainly the burn infections were caused by ESBLs than carbapenemases. There was no significant association of burn-related parameters with burn infections (p >0.05) due to ESBL producing bacteria (Table 3). Carbapenemases-producing isolates from second-degree burn patients were 76(19%). 89 (22.3%) patients suffering from carbapenemase infections had a TBSA of less than 10%. For carbapenemases infection, the major source of the burn was also flame observed in 93(23.3%) patients. Second-degree burns were the particular cause of carbapenemase infections in 76 (19%) patients (λ2=9.192, p=0.01).
Post-burn infection-related factors
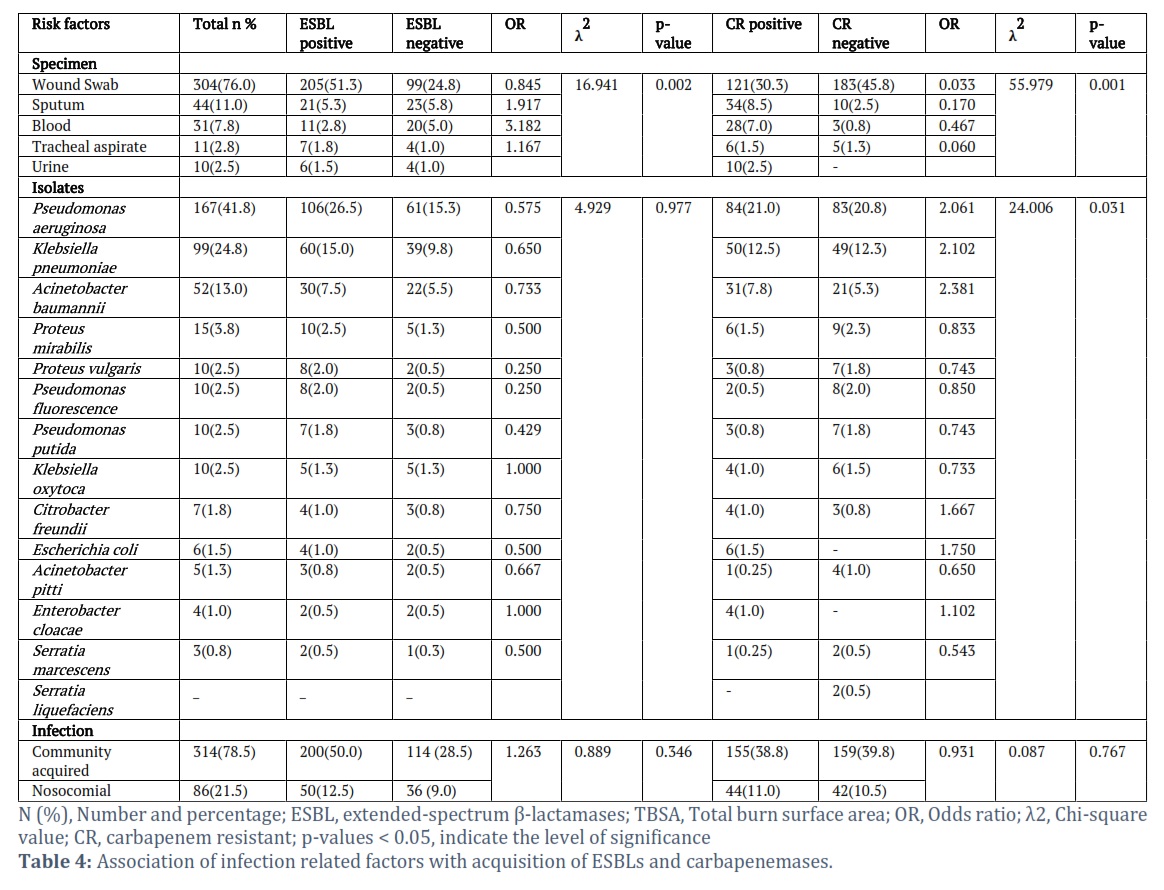
Mostly ESBLs-producing isolates were isolated from burn wound swabs specimens from 205 (51.3%) patients. Compared to nosocomial infections, community-acquired infections were observed in 314 (78.5%) patients were observed. The higher degree of community-acquired infections was associated with ESBLs positive strains in 200 (50%) burn patients. The nosocomial infections resulted from ESBLs positive strains in 50 (12.5%) burn patients. The most dominant ESBL strain was P. aeruginosa isolated from 106 (26.5%) burns patients. There was ESBLs positive K. pneumonia isolated from 60 (15%) and A. baumannii from 30(7.5%) burn patients. Among infection-related factors, wound specimens were significantly associated with ESBL-producing strains (λ2=16.9, p=0.002). Carbapenemases-producing isolates were also commonly isolated from 121 (30.3%) burn wound swab specimens. The higher proportion of community-acquired infections was associated with carbapenemase-positive strains in 155(38.8%) burn patients. The nosocomial infections resulted from carbapenemase-positive strains in 44 (11%) burn patients. The most common carbapenemase strain was P. aeruginosa isolated from 84(21%) burns patients. There were carbapenemase-positive K. pneumoniae isolated from 50 (12.5%) and A. baumannii from 31(7.8%) burn patients. In infection-related factors, wound swab was mainly associated with burn infections due to carbapenemases producing bacteria (λ2=24.006, p=0.031) by P. aeruginosa (Table 4).
Figures & Tables

Burn injuries are one of the major health problems because they degrade the skin of the human body. Multiple factors are involved in various epidemiology of burn wound injury. But bacterial infections are the leading cause of mortality in burn patients.
In the present study, 400 bacterial isolates from burn patients (with their clinical history) were obtained and screened for ESBLs and Carbapenemases production. Out of 400 burn isolates, there were 250 (62.5%) strains producing ESBLs and 199 (50%) carbapenemases. For further analysis, association of various factors with the prevalence of ESBLs and Carbapenemases production was assessed.
Young people aged 20-29 years are more exposed to ESBL 96 (24%) and carbapenemases 70 (17.5%) infections. In contrast, Shalabh et al., reported most cases in ages 31-40 years (27.5%). Here, males 173(43.3%) are more exposed to ESBL infections than females 77(19.3%). Similar findings were reported of a higher frequency of male patients being infected (60.7%) [11]. In this study, more frequency of 235 (58.8%) of burnt patients was residing in urban areas. In contrast, Anvarinejad et al., discussed most of the cases from rural areas [12]. We observed 52.5% of patients with poor economic status. The finding agrees with Chamania et al, which shows a strong relationship between MDR infections and people with low financial levels [13]. Here we observed a high frequency of patients admitted indoors, and 42.5% stayed in the hospital for less than one week. No significant association of MDR infections with an extended hospital stay was observed. This finding was in contrast to Fadeyibi et al., who has reported a significant association of 50% of patients with MDR infections [14]. Melake et al., also investigated the association of 52% bacterial infection with a hospital stay of more than three weeks [15] 26.00% of burnt patients were observed for treatment in the ICU and showed no association with MDR infections. On the other hand, Leseva et al., reported most of the patients in ICU with MDR infections [16].
A high frequency of burnt patients was observed, with 26.5% first and 19% second-degree burns. 30.8% of patients arrived with less than 10% TBSA. Contrary to this, Vural et al., mainly discussed cases of second-degree burns. Most patients came with less than 30% TBSA [17]. In the present study, 29% of patients died from flame burns. However, Vural et al. discussed scalds 55% as the prominent cause of burns [17]. Fadeyibi et al. reported flame was responsible for most of the burns in 60% of cases [14]
The patients admitted after a delay of 24 hours are more exposed to ESBL 32.3% and carbapenemases 19.3% producing strains. This finding was consistent with Fadeyibi et al. Our study demonstrated that the mortality rate of patients with ESBLs and carbapenemases infection is 3.5%. In contrast to this Fadeyibi et al reported 14% of cases died due to multi-organ failure and septicemia [14]. A high frequency of community-acquired infections 314 (78.5%) was recorded with ESBLs. P. aeruginosa 106 (26.5%) was prevalent, followed by K. pneumoniae 60 (15%) and A. baumannii 30 (7.5%). Similarly, Kabanangi et al., and Tchakal-Mesbahi also reported the predominance of P. aeruginosa (39.0%) [3-18]. Post-burn Infections are the foremost cause of death out of which, burn unit infections are the leading cause of death in burn units [19]. Therefore, suitable antibiotics must be given to lessen the colonization with MDR strains [20].
This study found a high frequency of multidrug-resistant gram-negative (MDR-GN) bacteria associated with post-burn infections. MDR-GN is the leading cause of death among post-burn patients, especially Pseudomonas spp. Young adults were immensely infected by burn injuries. In Pakistan, facilities in burn units are limited. Therefore, proper monitoring and care are required. There is a dire need to introduce the latest medical technologies to detect ESBL and CR strains rapidly. Early diagnosis will identify the bacteria, and burn injury can be supervised accurately. More work is required on this critical issue that will limit the complications and mortality of patients with post-burn infections.
Author Contributions
All performed experimental work and the study were supervised by Saba Riaz. MHH and AA were involved in study design and conducting the project. All authors read and approved the final manuscript. All named authors have read the journal's authorship agreement and have reviewed and approved the manuscript. The authors declare that this work was done by the members in the list of authors. They are responsible for all the contents in this article.
The author declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- Gong Y, Y Peng, X Luo, C Zhang, Y Shi, et al. Different infection profiles and antimicrobial resistance patterns between burn ICU and common wards. Frontiers in cellular and infection microbiology, (2021). 11: 1-14.
- Hu Y, D Li, L Xu, Y Hu, Y Sang, et al. Epidemiology and outcomes of bloodstream infections in severe burn patients: A six-year retrospective study. Antimicrobial Resistance & Infection Control, (2021). 10(1): 1-8.
- Kabanangi F, EJ Nkuwi, J Manyahi, S Moyo, M Majigo. High level of multidrug-resistant gram-negative pathogens causing burn wound infections in hospitalized children in dar es salaam, tanzania. International journal of microbiology, (2021); 2021: 1-8.
- Ruegsegger L, J Xiao, A Naziripour, T Kanumuambidi, D Brown et al. Multidrug-Resistant Gram-Negative Bacteria in Burn Patients. Antimicrobial agents and chemotherapy, (2022); 66(9): 00622-00688.
- Javanmardi F, A Emami, N Pirbonyeh, M Rajaee, G Hatam, et al. Study of multidrug resistance in prevalent Gram-negative bacteria in burn patients in Iran: a systematic review and meta-analysis. Journal of Global Antimicrobial Resistance, (2019); 19: 64-72.
- Corcione S, AD’Avolio, RC Loia, A Pensa, FV Segala, et al Pharmacokinetics of meropenem in burn patients with infections caused by Gram-negative bacteria: Are we getting close to the right treatment. Journal of global antimicrobial resistance, (2020); 20: 22-27.
- Park JJ, YB Seo, YK Choi, D Kym, J Lee. Changes in the prevalence of causative pathogens isolated from severe burn patients from 2012 to 2017. Burns, (2020); 46(3): 695-701.
- Richcane A, CT Samuel, A Pius, F Enoch, KG Thomas, et al Bacteriological profile of burn wound isolates in a burns center of a tertiary hospital. Journal of acute disease, (2017); 6(4): 181-186.
- Magiorakos AP, A Srinivasan, RB Carey, Y Carmeli, M Falagas, et al Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clinical microbiology and infection, (2012); 18(3): 268-281.
- Chen Z, H Niu, G Chen, M Li, M Li, Y Zhou. Prevalence of ESBLs-producing Pseudomonas aeruginosa isolates from different wards in a Chinese teaching hospital. International journal of clinical and experimental medicine, (2015); 8(10): 19400-19405.
- Jauhari S, S Pal, M Goyal, R Prakash, D Juyal. Bacteriological and antimicrobial sensitivity profile of burn wound infections in a tertiary care hospital of uttarakhand. Int J Curr Res, (2020); 12: 30-36.
- Anvarinejad M, A Japoni, N Rafaatpour, J Mardaneh, P Abbasi, et al. Burn patients infected with metallo-Beta-lactamase-producing Pseudomonas aeruginosa: Multidrug-resistant strains. Archives of trauma research, (2014); 3(2): 1-5.
- Chamania S, N Hemvani, S Joshi. Burn wound infection: Current problem and unmet needs. Indian Journal of Burns, (2012); 20(1): 18-22.
- Fadeyibi IO, MA Raji, NA Ibrahim, AO Ugburo, S Ademiluyi. Bacteriology of infected burn wounds in the burn wards of a teaching hospital in Southwest Nigeria. Burns, (2013). 39(1): 168-173.
- Melake NA, NA Eissa, TF Keshk, AS Sleem. Prevalence of multidrug-resistant bacteria isolated from patients with burn infection. Menoufia Medical Journal, (2015); 28(3): 677-684.
- Leseva M, M Arguirova, D Nashev, E Zamfirova, O Hadzhyiski. Nosocomial infections in burn patients: etiology, antimicrobial resistance, means to control. Annals of burns and fire disasters, (2013); 26(1): 5-11.
- Vural MK, U Altoparlak, D Celebi, MN Akcay. Comparison of surface swab and quantitative biopsy cultures dependent on isolated microorganisms from burn wounds. The Eurasian Journal of Medicine, (2013); 45(1): 34-38.
- Tchakal-Mesbahi A, M Abdouni, M Metref. Prevalence Of Multidrug-Resistant Bacteria Isolated From Burn Wounds In Algeria. Annals of burns and fire disasters, (2021); 34(2): 150-156.
- Vickers ML, E Malacova, GJ Milinovich, P Harris, L Eriksson, JM Dulhunty, MO Cotta. Modifiable risk factors for multidrug‐resistant Gram‐negative infection in critically ill burn patients: a systematic review and meta‐analysis. ANZ Journal of Surgery, (2019); 89(10): 1256-1260.
- Costescu Strachinaru, DI, JL Gallez, PM François, D Baekelandt, MS Paridaens, et al. Epidemiology and etiology of blood stream infections in a Belgian burn wound center. Acta Clinica Belgica, (2022); 77(2): 353-359.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0![]()