

Full Length Research Article
Establishing a classification of the stages of progression of the novel coronavirus infection to improve and facilitate morphologic diagnosis
Yevgeniy Sokharev1, Aliya Yskak2,3*, Kuanysh Zhumalynov2, Elizaveta Koneva4, Liudmila Babaskina4, Jamilya Nugmanova5, Khizir Bataev6, Shemia Chupanova7, Yerbol Isakaev2, Murat Nurushev8, Vadim Chashkov2, Gulnaz Yermoldina9, Andrey Baksheev10
Adv. life sci., vol. 11, no. 4, pp. 953-959, November 2024
*– Corresponding Author: Aliya Yskak (al.bugubaeva@gmail.com)
Authors' Affiliations
2. A. Baitursynov Kostanay Regional University, Kostanay – Kazakhstan
3. Lomonosov Moscow State University, Moscow – Russia
4. Sechenov First Moscow State Medical University – Russia
5. Asfendiyarov Kazakh National Medical University – Kazakhstan
6. Chechen State University – Russia
7. Dagestan State Medical University – Russia
8. Astana International University – Kazakhstan
9. Institute of Information And Computational Technologies – Kazakhstan
10. Voino-Yasenetsky Krasnoyarsk State Medical University – Russia
[Date Received: 24/06/2024; Date Revised: 14/09/2024; Date Published: 24/11/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: COVID-19, caused by SARS-CoV-2, has impacted over 264 million people and caused over 5 million deaths worldwide. Symptoms often include viral pneumonia, with complications like acute respiratory distress or sepsis, as well as myocarditis and kidney damage. The purpose of the study is to investigate the impact of COVID-19 on endocrine glands, as well as to develop a classification of stages of the course of COVID-19 to improve and simplify morphological diagnosis.
Methods: The studies conducted include systemic analysis of the para-clinical data of patients who died of COVID-19 (according to medical documentation); a macroscopic study assessing the size and weight of external manifestations of endocrine organ lesions in COVID-19 cases with statistical evaluation of the detected signs. Archive analysis covers para-clinical data and data on significant concomitant and background pathologies based on the medical histories of 780 deaths from COVID-19 in infectious diseases hospitals of the city of Kostanay (Kazakhstan) during the period from 2019 to 2022.
Result: Using pathomorphologic data from COVID-19 autopsies, we developed a scale for semi-quantitative analysis of each case. Medical data analysis suggests that the most notable endocrine changes are elevated blood glucose and low catecholamine levels due to adrenal hemosiderosis. No significant changes in sex or thyroid hormones were observed.
Conclusion: The obtained findings require further consideration, given that the studied patients make up a rather diverse group. Nevertheless, the study can serve as an additional source of information in the struggle against COVID-19.
Keywords: Coronavirus infection; Endocrine glands; Stage of disease
Introduction![]()
The novel coronavirus infection (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has affected over 264 million people and taken over 5 million lives in more than 200 countries [1]. Although COVID-19 can be asymptomatic, the primary manifestation in symptomatic patients is viral pneumonia, sometimes complicated by acute respiratory distress syndrome and/or sepsis [2, 3]. In addition, myocarditis and acute kidney damage have also been described in COVID-19 [4]. In contrast, the development of endocrinological disorders (de novo) in patients with COVID-19 has not yet been reported.
The pathogenesis of COVID-19 causes SARS-CoV-2 to enter the respiratory system and settle in the lung parenchyma [5]. It then uses angiotensin-transforming enzyme 2 (ACE2) as a receptor for penetration into host pneumocytes [4]. Furthermore, viral RNA has also been found in the plasma or serum of patients with the novel coronavirus infection, suggesting viremia [6, 7]. This means that, in addition to pneumocytes, the virus can interact with ACE2 expressed in other tissues [8].
There are many endocrine organs that express ACE2, namely the pancreas, the thyroid, testicles, ovaries, adrenal glands, and pituitary glands [9, 10]. Although adverse consequences for the endocrine system could be expected from the interaction of SARS-CoV-2 with the ACE2 expressed by these organs, there are yet no clinical or preclinical data indicating this. However, based on observations taken partly from studies relating to the previous SARS outbreak (2003) [11] and partly from animal models [12], we seek to investigate the possible effects of coronavirus infection on the endocrine system.
The goal of the study is to research the impact of COVID-19 on endocrine glands and to develop a classification of stages of the course of COVID-19 to improve and simplify morphological diagnosis. To clarify and detail the purposes of the study, the following research objectives are set:
1. To conduct an analysis of clinical diagnostic markers of endocrine dysfunction among patients who died of COVID-19.
2. To identify the main pathomorphologic changes in the internal organs of those who died of COVID-19 at different times from the onset of the disease, with the determination of their informativeness.
3. To examine the connection between pre-existing endocrine gland pathologies to the rate and time of death (thyroid disease, diabetes mellitus, pancreatitis, adrenal adenoma).
4. To examine the relationship between the onset of symptoms and the time of death and their relationship to the main morphological manifestations of COVID-19.
Based on the above, to develop conceptions about the phases of development of COVID-19 in adults.
Methods![]()
Research Design
The materials and methods employed for the study include systemic analysis, macroscopic study, histological study in accordance with the primary goal and objectives of the study, we conducted the analysis of archival, clinical, and histological materials.
Archive analysis covered para-clinical data and data on significant concomitant and background pathologies based on the medical histories of 780 deaths from COVID-19 in infectious diseases hospitals of the city of Kostanay (Kazakhstan during the period from 2019 to 2022.). Ethical approval for the use of these materials was obtained from the Institutional Review Board of the infectious diseases hospitals in Kostanay, Kazakhstan. All patient data was anonymized, and the study complied with the ethical guidelines for retrospective research
Research Stages
Pathomorphologic research was carried out in several stages:
1. In the first stage, to examine the frequency and structure of mortality due to COVID-19, we analyzed the results of autopsies of the bodies of the deceased, received by the pathology bureaus, and forensic examination of the city of Kostanay in the indicated time period, with the diagnosis of coronavirus infection and viral pneumonia in the number of 90 people.
2. The second stage consisted of a systemic morphological and morphometric examination of fragments of internal organs (glands of internal secretion). The procedure of histological material extraction from organs and tissues was as follows: during the autopsy, a bioptat of 1×1 cm was collected, after which the material was fixed in 10% buffered formalin, and then underwent dehydration and additional fixation through alcohols of rising strength, according to the standard method; the prepared pieces were then placed into paraffin wax and fixed the paraffin-filled histological material to the substrate, manufacturing a histological block (block-preparation).
The degree of fixation readiness of the histological material was controlled visually by applying a colored 10% buffered formalin. Food colorant E120*(carmine) was chosen as the dye (Figure 1).
After this, the histological block was microsectioned: the block preparation on the substrate is tightly fixed in the microtome holder, and with a series of translational movements of the microtome blade, thin slices of a certain thickness are cut off the surface of the paraffin block. The serial 4-6 μm thick microtome sections are deparaffinized in warm distilled water, and the resulting slices are fixed on test glasses precharged with an electric charge.
Then, according to the standard technique, the sections were stained with histological dyes:
● hematoxylin (first stage);
● eosin with buffering in a standard solution of aluminum-based alums (second stage).
Following this, the stained samples were placed in standard BioMount medium and covered by coverslips.
3. The final stage was the pathomorphologic assessment of the manifestation of histological changes.
Data Analysis
The volume shares of the specified structural components were determined by the method of point counting using G.G. Avtandilov's 100-point grid.
Calculations were performed in ten random fields of vision in ten histological sections of internal organs (endocrine secretion glands).
The quantitative indicators obtained in this way were processed statistically with the calculation of average statistical indicators with an average error. Data processing was performed according to the method of variation statistics using readily available software (Excel).
Based on the obtained values and the number of observations, the probability of reliable differences between the compared values was determined using Student's criterion. The differences were deemed reliable starting from P values less than 0.05, i.e., when the probability of difference between the indicators was equal to or exceeded 95%.
The frequency characteristics of qualitative indicators were compared using non-parametric methods with Yates correction (for small groups) and Pearson's test with one and two-sided Fisher's tests.
To identify the degree of informativeness of features, for semi-quantitative analysis and their quantitative expression, we applied Kullback-Leibler divergence.
A table was developed for a semi-quantitative score-based method of analysis of identified microscopic signs using the scale:
● 1+ weak sign,
● 2 + moderate sign,
● 3 + strong sign,
● 4 + very strong sign
A robust conclusion about the presence or absence of reliable change was formulated in cases of essentially uniform results across the entire set of criteria applied.
Results![]()
Analysis of changes in para-clinical indicators
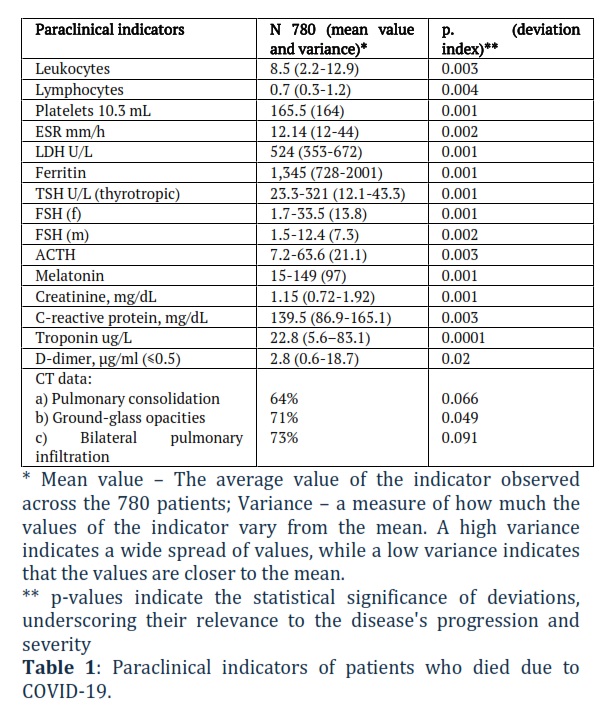
In the analysis of changes in para-clinical parameters and hormonal background, of note are the subnormal leukocyte counts and lymphopenia observed in most patients. Table 1 lists those paraclinical indicators, including leukocytes, melatonin and creatinine.
This table presents the paraclinical (laboratory and diagnostic) indicators observed in COVID-19 patients, specifically those who died due to the infection. It includes various blood parameters, imaging findings, and other clinical indicators, with statistical significance (p-values) highlighting deviations from the normal range. The values are given as mean and variance for each indicator.
A sharp increase in plasma ferritin, as well as an increase in ESR in conjunction with hormonal disorders, some increase in aminotransferase activity, troponin concentration, and creatinine, in particular with metabolic disturbances as a reduction in basic indices, overall indicate a rather high degree of infectious-inflammatory process with inadequate immune response, and an increasing imbalance in the functioning of endocrine systems as an outcome of the stressor influence of tissue hypoxia factors. This process is most clearly manifested in brain tissue damage since this organ is the least sensitive to hypoxia. The hypoxia appeared in marked edema and hemorrhage of brain tissue when examining all its sections.
Analyzing the data obtained in the study of the comorbid background of patients who died from COVID-19, we can conclude that the incidence of arterial hypertension (AH), diabetes, and obesity is quite high in this group of patients. In contrast, the incidence of chronic obstructive pulmonary disease (COPD), bronchial asthma (BA), chronic pyelonephritis, and various malignant tumors (onco) is comparable with that in patients who passed without COVID-19. This gives reason to assert that the probability of death from COVID-19 is directly related to the presence of unfavorable comorbid background, including endocrine system pathology.
The analysis of medical records from patients in Kostanay revealed the following comorbid diseases (absolute numbers) in persons who died from COVID-19: AH – 663; CIHD – 324; Type 2 diabetes – 321; CVA – 84; Obesity – 435; COPD – 56; BA – 13; ONCO – 8; liver diseases – 9; kidney disease – 16.
Pathomorphologic changes of endocrine system organs with the degree of informativeness of morphologic signs at death from COVID-19
To determine the frequency of occurrence of a symptom, we analyzed autopsy results and histological studies of 90 cadavers. The frequency of occurrence of pathomorphologic signs was evaluated using the following scoring system: I>0.5–1 – low informativeness of the sign, I<1.5-2 – moderate informativeness, I<2-7 – high informativeness.
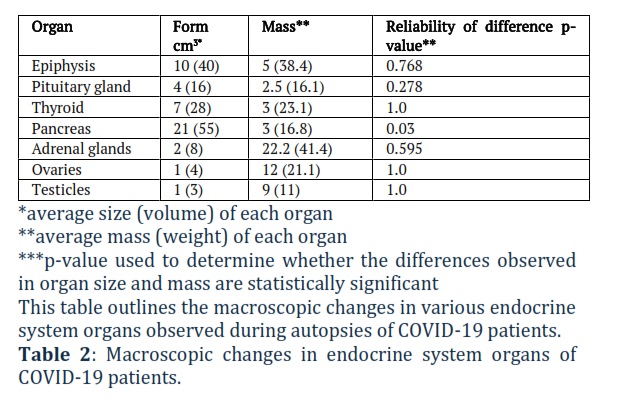
Table 2 lists macroscopic changes in endocrine system organs with reliability of difference considered.
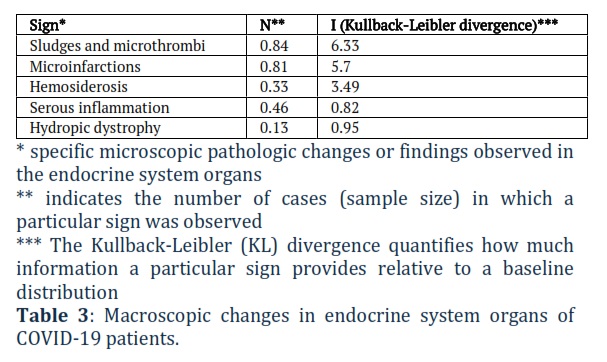
Table 3 all the while lists signs of microscopic changes in endocrine system organs.
Proceeding from the data in Tables 2 and 3, we find that the most informative signs of microscopic changes in the internal secretion glands in the course of COVID-19 are serious desquamative inflammation, the hemosiderosis of adrenal tissues and pancreas and disturbance of microvascular rheology in internal secretion glands.
Pathomorphologic changes of internal organs in COVID-19 deaths
The conducted research reveals an inextricable direct and indirect connection of endocrine organs with the activity of other organs of the human body. At the macroscopic level in the brain, there was a pronounced edema and sharp plethora of the soft cerebral membrane, and sharp plethora of the brain matter on the section, with pinkish-colored liquor in the brain ventricles as a manifestation of acute disturbance of peripheral blood rheology against the background of general hypoxic influences. Histologic examination of brain tissue taken from different sections shows signs of acute circulatory disorder expressed in irregular plethora of vessels, erythrostasis in the capillary lumen and full-fledged thrombi, and perivascular and pericellular cerebral edema of varying severity.
Cortical neurons appear mostly swollen, their nuclei enlarged and hyperchromic. There is wrinkling and deformation of single neurons with moderate microglial reaction, with phenomena of neurolysis and neurophagia of individual neurocytes. In the pathomorphologic examination of lung tissue, we detected signs of a sharp increase in the mass of lung tissue with a moderate increase in volume. The lungs are dense to touch, with sharply pronounced pointed edges of the lobes. In part of the studies, the lung tissue on the section is of a dense elastic consistency, with scanty serosanguineous discharge from the section surface. Partially, the lung tissue is dense and elastic with scanty discharge, according to the type of lacquered lung. In the case of secondary infection, there is foci of purulent inflammation, as well as areas of organization of pulmonary infarction with the presence of dystelectasis. The lung changes are overall macroscopically consistent with the generally accepted concept of shock lungs.
Extremely specific and the most characteristic changes are found in the pulmonary vascular system, expressed in the presence of thrombi in arteries and veins of various diameters, as well as single thromboemboli. Fibrinous and fibrinopurulent pleurisy is rarely encountered, more often in case of secondary infection. In the histological study of lung tissue, we note the presence of changing phases of pathomorphologic changes depending on the age of the disease course. At the first stages, there is diffuse alveolar damage with pronounced rheologic disturbance by the type of acute hemorrhagic edema of alveolar septa with a weak degree of serous inflammatory infiltration. Inside the alveoli, there are signs of sloughing and damage of alveolocytes with fibrin deposition and the formation of hyaline membranes. Further, we observe phagocytosis of hyaline membranes with the appearance of quite specific viral giant-cell transformation of second-order alveolocytes, proliferation of fibroblasts, and phagocytosis of hyaline membranes by alveolar macrophages.
There is a change in the interstitium and in the lumen of alveoli with fibrin deposition, small thrombi appear in the lumen of pulmonary capillaries. Further, there is a thickening of fibrin masses with their resorption and metaplasia of bronchiolar epithelium by the type of signs of bronchiolization of alveolar epithelium, with proliferative restructuring of alveolar epithelium presenting as proliferation of immature alveolocytes of the second order.
In the pathomorphologic study of the heart, tissue reveals acute ischemic changes on the background of focal or diffuse non-glandular cardiosclerosis, focal coronary sclerosis, petechial and confluent subepicardial hemorrhages are characteristic.
In thrombosis of coronary arteries (in the absence of unstable atherosclerotic plaques or atherosclerosis in general), some of the deceased developed small-focal, less often transmural myocardial infarctions, as well as foci of serous myocarditis.
The examination of the kidneys was of great interest to us because of the high involvement of this organ's systems in the pathogenetic links of development and decompensation of the functions of the vascular system in the unfolding of COVID-19 pathogenesis. Pathomorphologic examination of the kidneys reveals hypoxic and acutely dystrophic changes. In the preparations, the tubules are distributed in the cortex mostly evenly. Renal tubules show hyperemia, some are hypercellular and edematous. Part of the tubules is sclerosed. Proximal and distal tubules are dilated, and the epithelium of part of the tubules is necrotized. Vessels are plethoric, with hyalinized walls.
Pathomorphologic changes in the gastrointestinal tract are important because of the presence of symptoms of primary GI involvement in patients with COVID-19 [20]. Upon examining the esophagus and stomach, attention is drawn to the presence of acute erosive esophagitis and gastritis, with hemorrhagic impregnation of the gastric wall and clear signs of rheology disturbance in the microvasculature vessels, probably caused by acute hypoxia.
In the organs of the immune system, at the initial stages of the disease, most cases demonstrate abnormal hypoplasia, in both lymph nodes and the spleen. Lymph nodes in all sections are not enlarged, small, and slightly pinkish on the section. The histological examination notes hypoplasia with the washout of mature lymphocytes against the background of an acute disorder of rheology in the microvasculature vessels. Splenic tissue at the first stages of the disease is also mostly intact, at the histological level, there are signs of lymphoid exhaustion in the white pulp and pronouncedly plethoric red pulp. Subsequently, upon the accession of secondary infection, a pattern of lymphoid hyperplasia is observed with the deposition of large amounts of hemosiderin. At late stages, spleen tissue infarctions are common.
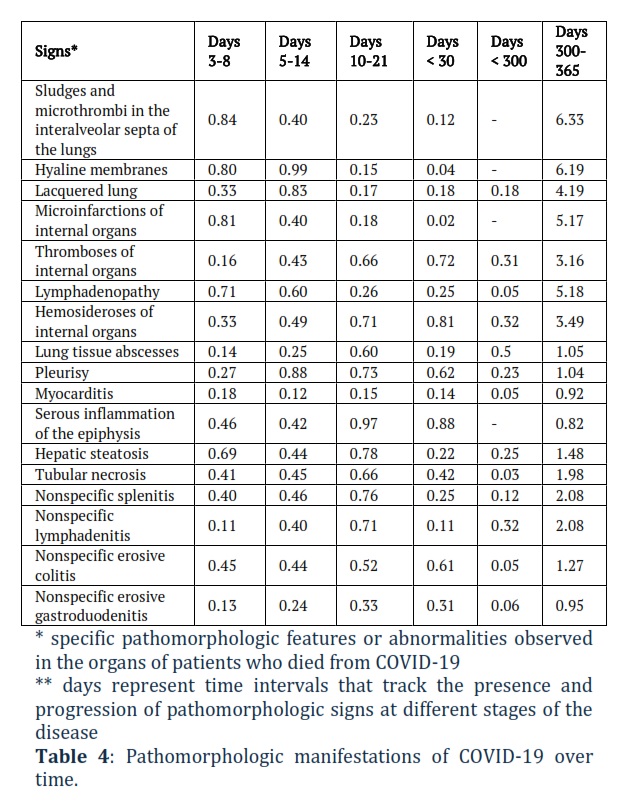
Based on the data from pathomorphologic examination of the organs and tissues of patients who succumbed to COVID-19, we developed a scale for semi-quantitative analysis of the occurrence of the pathomorphologic feature of each case described on autopsy. Based on this scale, we compiled a summary table (Table 4) of the main pathomorphologic manifestations of COVID-19 at different periods from the time of onset to the time of death, with an assessment of the statistical reliability of the sign. Signs with a low level of reliability were not included in the summary table.
In table 4 can be found a summary of the main pathomorphologic manifestations of the novel coronavirus infection.
This table summarizes the key pathomorphologic signs at different stages of COVID-19 progression, from early disease (3–8 days) to long-term (300-365 days). The information highlights how different organs and tissues react over time and the statistical reliability of each observation.
Figures & Tables
The obtained findings are consistent with other sources describing endocrine system disorders. Hemosiderosis of adrenal tissue and pancreatic tissue disrupts the function of cellular respiration and glucagon positive cells, which in turn entails decreased pancreatic function and exacerbates the course of diabetes mellitus, as well as hyperglycemia [13-15]. Accumulation of free iron and hemosiderin in the zona fasciculata of the adrenal cortex causes corticosteroid deficiency, which is evident in the clinical picture of hypocortisolism in the convalescence period [16]. The so-called chronic fatigue syndrome is highly likely to result from adrenal dysfunction, one of the triggers of which is adrenal hemosiderosis.
The pathomorphologic changes found in testicular tissue are marked by an acute impairment of rheology, which in turn correlates with decreased testicular function and low levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH), as well as testosterone [17]. A striking manifestation of the latter is suppression of the spermatogenic epithelium with a decrease in the total number of spermatozoa per unit area of the microscopy field.
The pathomorphologic changes found in thyroid tissue are chiefly distinguished by the high expression of ACE2, which is manifested by an increase in the mass and volume of the thyroid gland and by microscopic dystrophic changes of thyrocytes, while the thyroid tissue remains within subnormal values. This indicates a stage-by-stage involvement of the thyroid tissue and the absence of direct cytopathic action of the virus on the gland tissue [18, 19].
Pathomorphologic changes in pituitary and epiphysis tissue are characterized by signs of nonspecific acute inflammatory serous lesions of the tissues of these organs.
Medical documentation data and its analysis give reason to conclude that the most indicative of lifetime changes in endocrine function is a disorder of carbohydrate metabolism in the form of elevated blood glucose levels, as well as low catecholamine levels due to adrenal hemosiderosis. Clear disturbance of any other indicators of the patient's endocrine background, such as decreased levels of sex hormones or thyroid hormones, is not detected in our investigation. Due to the small sample size in this study, the analysis of melatonin and serotonin metabolic disturbances requires further elaboration.
The rather small number of observations obtained makes it difficult to judge unequivocally the extent to which endocrine dysfunction influences the course of the 2019-nCoV infection. According to our findings, it has an aggravating effect in active coronavirus infection, especially in severe stages of COVID-19 (widespread lung lesions in grades 3-4, according to a CT study). Concerning the immediate influence of 2019-nCoV on the endocrine system, it is mediated through hypoxic and toxic effects on the target cells of the endocrine glands. The obtained data require further reflection, as the studied patients constitute a rather heterogeneous group. Nevertheless, this study may serve as an additional source of information in the struggle against COVID-19.
Author Contributions
Yevgeniy Sokharev: Conceptualization, Data Curation, and Writing – Original Draft.
Aliya Yskak: Project Administration, Supervision, and Writing – Review & Editing.
Kuanysh Zhumalynov: Methodology, Investigation, and Formal Analysis.
Elizaveta Koneva: Data Curation and Visualization.
Liudmila Babaskina: Writing – Original Draft and Resources.
Jamilya Nugmanova: Supervision, Writing – Review & Editing.
Khizir Bataev: Methodology and Formal Analysis.
Shemia Chupanova: Investigation and Validation.
Yerbol Isakaev: Software and Data Curation.
Murat Nurushev: Resources and Writing – Review & Editing.
Vadim Chashkov: Conceptualization and Investigation.
Gulnaz Yermoldina: Visualization and Writing – Original Draft.
Andrey Baksheev: Supervision and Project Administration
The author declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- Khurshid A, Amin R, Aziz A, Ahmed O, Abdel-Haliem MEF. Decipher the potential therapeutic intervention points of 2019-nCoV: a pharmacological perspective. Advancements in Life Sciences, (2022); 9(4): 412-429.
- Shlyakhto EV, Konradi AO, Arutyunov GP, Arutyunov AG, Bautin AE, Boytsov SA et al. Guidelines for the diagnosis and treatment of circulatory diseases in the context of the COVID-19 pandemic. Russian Journal of Cardiology, (2020); 25(3): 1-21.
- Ye M, Wysocki J, William J, Soler MJ, Cokic I, Batlle D. Glomerular localization and expression of Angiotensin-converting enzyme 2 and Angiotensin-converting enzyme: implications for albuminuria in diabetes. Journal of the American Society of Nephrology, (2006); 17(11): 3067-3075.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet, (2020); 395(10223): 497-506.
- Islamova YK, Bataev KM. Epidemiological aspects and prevention of coronavirus infection (COVID-19). Bulletin of the Medical Institute, (2023); 1(22): 42-46.
- Soldevila B, Puig-Domingo M, Marazuela M. Basic mechanisms of SARS-CoV-2 infection. What endocrine systems could be implicated? Reviews in Endocrine and Metabolic Disorders, (2021); 23: 137-150.
- Wan Y, Shang J, Graham R, Baric RS, Li F. Receptor recognition by novel coronavirus from Wuhan: an analysis based on decade-long structural studies of SARS. Journal of Virology, (2020); 94(7).
- Li MY, Li L, Zhang Y, Wang XS. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infectious Diseases of Poverty, (2020); 9(1): 45.
- Kuba K, Imai Y, Rao S, Gao H, Guo F, Guan B et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury. Nature Medicine, (2005); 11(8): 875-879.
- Liu F, Long X, Zou W, Fang M, Wu W, Li W et al. Highly ACE2 expression in pancreas may cause pancreas damage after SARS-CoV-2 infection. medRxiv, (2020).
- Morse JS, Lalonde T, Xu S, Liu WR. Learning from the past: possible urgent prevention and treatment options for severe acute respiratory infections caused by 2019-nCoV. Chembiochem, (2020); 21(5): 730-738.
- Rehman S, Nnabuike UE, Abbas A, Rahman A, Malik U, Effendi MH, Hussain K, Raza MA. A study on the Impacts of COVID-19 on health, Economy, Employment and Social Life of People in Indonesia. Advancements in Life Sciences, (2022); 9(3): 340-6.
- Mao Y, Xu B, Guan W, Xu D, Li F, Ren R et al. The adrenal cortex, an underestimated site of SARS-CoV-2 infection. Frontiers in Endocrinology, (2021); 11: 593179.
- Müller JA, Groß R, Conzelmann C, Krüger J, Merle U, Steinhart J et al. SARS-CoV-2 infects and replicates in cells of the human endocrine and exocrine pancreas. Nature Metabolism, (2021); 3: 149-165.
- Wu CT, Lidsky PV, Xiao Y, Lee IT, Cheng R, Nakayama T et al. SARS-CoV-2 infects human pancreatic beta cells and elicits beta cell impairment. Cell Metabolism, (2021); 33: 1565-1576.
- Leow MK, Kwek DS, Ng AW, Ong KC, Kaw GJ, Lee LS. Hypocortisolism in survivors of severe acute respiratory syndrome (SARS). Clinical Endocrinology. (2005); 63(2): 197-202.
- Ma L, Xie W, Li D, Shi L, Ye G, Mao Y et al. Evaluation of sex-related hormones and semen characteristics in reproductive-aged male COVID-19 patients. Journal of Medical Virology, (2021); 93(1): 456-462.
- Clarke SA, Abbara A, Dhillo WS. Impact of COVID-19 on the endocrine system–a mini-review. Endocrinology, (2021); 163(1): bqab203.
- Wang W, Su X, Ding Y, Fan W, Zhou W, Su J et al. Thyroid function abnormalities in COVID-19 patients. Frontiers in Endocrinology, (2021); 19(11): 623792.
- Ghazanfar H, Kandhi S, Shin D, Muthumanickam A, Gurjar H, Qureshi Za et al. Impact of COVID-19 on the gastrointestinal tract: a clinical review. Cureus, (2022); 14(3): e23333.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0![]()