

Full Length Research Article
In Vitro Synergistic Activity of Ceftazidime-Avibactam and Aztreonam against New Delhi Metallo-β-Lactamase-Producing Clinical Enterobacterales Isolates
Naif Fahd AlAnazi1,2 £, Mohammad Marie1, Ali Mohammad Somily3,4, Khalifa Binkhamis3,4, Muhammad Arshad5,£, Akram A. Alfuraydi1, Muhammad Absar6, £ *
Adv. life sci., vol. 11, no. 4, pp. 871-877, November 2024
*– Corresponding Author: Muhammad Absar (mashwani82@gmail.com)
£. These authors contributed equally to this work
Authors' Affiliations
2. Department of Pathology & Laboratory Medicine, King Khalid University Hospital, King Saud University Medical City, King Saud University, Riyadh – Saudi Arabia
3. Department of Pathology, College of Medicine, King Saud University, Riyadh – Saudi Arabia
4. King Saud University Medical City, King Saud University, Riyadh – Saudi Arabia
5. Canberra, Australian Capital Territory – Australia
6. Department of Pathology and Laboratory Medicine, King Abdulaziz Hospital, Ministry of National Guard Health Affairs, AlAhsa – Saudi Arabia
[Date Received: 20/04/2024; Date Revised: 18/07/2024; Date Published: 15/10/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Carbapenemase-producing-Enterobacterales (CPE) infections are on the rise and associated with increased morbidity and mortality, due to a limited number of therapeutic options. The goal of this study was to assess the synergistic activity of ceftazidime-avibactam (CZA) and aztreonam (ATM) combination against phenotypically and genetically characterized blaMBL-producing Enterobacterales.
Methods: In this study, forty (n=40) non-repeat, CPE clinical isolates, including: n=35 Klebsiella pneumoniae, n=2 each of Escherichia coli and Klebsiella oxytoca, and n=1 Enterobacter cloacae isolates were identified and susceptibilities were assessed using the Vitek-II compact (bioMérieux, Inc., France) and Microscan Walkaway (Beckman Coulter) systems. Genotypic analysis of clinically relevant carbapenemases was performed by using Xpert-Carba-R assay on GeneXpert (Cepheid, USA). The minimum inhibitory concentrations (MICs) and synergy testing of CZA and ATM, were tested by the Etest fixed ratio method (bioMérieux, Inc., France). The fractional inhibitory concentration index (FICI) was calculated for each antibiotic.
Results: Our results showed that 97.5% of blaMBL-producing Enterobacterales isolates were susceptible to an in-vitro CZA + ATM combination regimen. The fractional inhibitory concentration index (FICI) ranged from 0.001 to 1.001. Among the tested CPE isolates, Synergy was observed in 36/40 (90%), an additive effect was observed in 5% (n=2)’ while two (5%) isolates showed indifference. There was no antagonism observed in our study.
Conclusion: Our study exhibited a potent activity of CZA and ATM combination synergy against clinical CPE metallo- β-lactamase producers. More extensive studies involving a variety of Gram-negative pathogens with different resistance mechanisms are required to determine the efficacy of this combination regimen.
Keywords: Synergy; Aztreonam; Ceftazidime-Avibactam; Carbapenem-Resistant Enterobacterales; Etest
Introduction![]()
Carbapenem-resistant Enterobacterales (CRE) infections are rising globally [1, 2]. Many countries report rising CRE cases [3]. High resistance and a lack of new antimicrobials limit therapeutic options and increase risk of morbidity and mortality [4]. Klebsiella pneumoniae and blaKPC dominate CRE [5]. A blaKPC epidemiology review includes global reports [6]. CREs have also been reported from Saudi Arabia, in contrast to other reports, blaNDM and blaOXA48 are the most common genotypes nationwide. A Majority of the CRE studies are reported from Riyadh, Saudi Arabia [3]. Alarmingly, the presence of CRE has also been documented in municipal wastewater from Jeddah [7]. T The mortality rate associated with CRE cases is 26-46% [3].
The hydrolytic mechanism at the active site divides carbapenemases into serine- and metallo-carbapenemases [8]. Several Enterobacterales genes confer carbapenem resistance including blaKPC, blaNDM, blaOXA-48, blaVIM, and blaIMP. Metallo-beta lactamases (MBL) include blaNDM, blaVIM, and blaIMP, while blaKPC and blaOXA48 are serine carbapenemases [9]. Beta-lactamase inhibitors (BLIs) were developed to combat different beta-lactamases. First-line BLIs included clavulanic acid, tazobactam, and sulbactam. Their narrow spectrum of activity makes them ineffective against carbapenemases. New BLI like avibactam, relebactam, zidebactam, and nacubactam are active against serine carbapenemases but not metallo-carbapenemases [10]. The newly introduced beta-lactam/BLI combination CZA has successfully treated CRE infections. CZA is inactive against MBL producers. Aztreonam is resistant to MBL hydrolytic activity, but other hydrolytic enzymes produced in MBL-positive strains like ESBL, serine carbapenemases like blaOXA48, blaKPC, and other cephalosporinases inactivate ATM, making it generally unsuitable for MBL producing CRE infections [11].
Few studies have shown that CZA and ATM work synergistically to treat CRE infections [12, 13]. CZA and ATM combinational therapy treated successfully a CRE bloodstream infection in neutropenic patients, caused by K. pneumoniae. The synergistic testing resulted in a substantial decrease in MIC of aztreonam from >256 to 0.094 ug/mL [14]. CZA and ATM were successfully used as prophylactic therapy in a cancer patient undergoing a solid organ transplant with a previous blaNDM-producing K. pneumoniae infection [15]. Pragasam and colleagues tested CZA and ATM's synergistic activity against 12 K. pneumoniae isolates with blaNDM, blaOXA48-like, and co-producers of blaNDM + blaOXA48. In vitro CZA MIC ranged from 0.5 to >8 μg/ml, while ATM MIC was 64 to 2048 μg/ml. A >8-fold MIC difference (synergistic effects) was observed when CZA MIC was combined with ATM at 4 μg/ml using the checkerboard method [16]. Another study found that CZA alone or in combination with ATM synergistically killed twenty-eight (28) blaNDM and two (02) blaNDM/blaKPC-producing K. pneumoniae isolates in vitro. Notably, 90% (27/30) strains showed synergism, while 3.3% (1/30) showed additive effects. Synergy was stronger against the tested isolates [17]. ATM and other β-lactamase inhibitors have shown synergistic activity against Enterobacterales isolates in vitro. The studies found 86%, 50%, and 20% of clinical isolates susceptible to CZA, amoxicillin-clavulanic acid, and ceftolozane-tazobactam [18]. To the best of our knowledge, no Saudi Arabian study examined CZA+ATM combination therapy for such cases. However, CZA and ATM have treated CRE infections in other countries. CZA + ATM combination therapy successfully treated blaNDM in the US [13]. French researchers also reported two successful CZA + ATM combinations in two isolates with blaNDM and blaOXA genotypes in the same year [12].
To find efficacious drug combinations that specifically combat high-level resistance due to New Delhi metallo-beta-lactamase-producing clinical Enterobacterales, we conducted an in-vitro study to evaluate the synergistic effects of CZA and ATM against Enterobacterales harboring blaNDM.
Methods![]()
Microorganisms, Identifications, and Susceptibilities:
A total of forty (n=40) blaNDM-positive Enterobacterales clinical isolates from inpatients, were isolated from a tertiary care hospital, King Khalid University Hospital in Riyadh, Saudi Arabia, between January 2017 and December 2019. The institutional review board of the hospital granted approval for the study. Carbapenem-resistant isolates were subjected to full identification and susceptibilities testing by using the VITEK®2 system (bioMérieux, Inc., France) and Microscan Walkaway system (Beckman Coulter, USA). All study isolates were stored at -80˚C in skimmed milk with 10% glycerol (SPML, Saudi Arabia). Before the experiment, isolates were revived by subculturing on sheep blood agar (SPML, Saudi Arabia). Antimicrobial testing was conducted using Mueller-Hinton agar plates (SPML, Saudi Arabia).
Institutional Review Board Statement:
The Institutional Review Board of the Faculty of Medicine, King Khalid University Hospital, King Saud University Medical City, Riyadh, Saudi Arabia, approved the study by the Declaration of Helsinki guidelines (approval number: Ref #: 20/0118/IRB).
Genotypic Analysis:
The genotypic analysis of carbapenem-resistant Enterobacterales isolates was conducted using the Xpert-Carba-R assay on the GeneXpert system (Cepheid, USA).
Antimicrobial Agents and MIC Determination:
We used ATM and CZA Etest strips from bioMérieux, Inc. in France. Klebsiella pneumoniae ATCC 70063 and Escherichia coli ATCC 25922 were used for quality control testing. Using gradient diffusion Etest strips, the MICs for CZA and ATM were found (bioMérieux, Inc., France). For these calculations, the manufacturer's recommendations were adhered to. For CZA and ATM, the range of antibiotic concentrations on an Etest strip was 0.016 to 256 μg/ml. The results were interpreted according to the breakpoints in CLSI 2020 [19]. The tested antibiotics' resistance thresholds were as follows: ATM = 16 μg/ml; CZA = 16 μg/ml. Minimum inhibitory concentration 50 (MIC50) and minimum inhibitory concentration 90 (MIC90) were defined as antibiotic concentrations at which 50% and 90% of the tested isolates were inhibited.
Etest Fixed Ratio Synergy Method:
The individual MICs and synergistic activity of CZA and ATM against CRE isolates were determined by inoculating Mueller-Hinton agar (MHA) plates with 0.5 McFarland suspension of test isolates. When testing synergy, (combination setups), the antibiotics under study were applied to the bacterial lawn one after the other using Etest strips. After five minutes of incubation at room temperature, the first Etest strip (ATM) was taken out and preserved as a scale for determining the minimum inhibitory concentration (MIC). The impression of the first Etest strip, ATM, was immediately covered by the second Etest strip (CZA). To make it easier to read the ATM MIC when CZA is present, the ATM strip was then positioned on top of CZA. The plates were kept for 18 hours at 36°C. Each Mueller-Hinton agar plate contained two Etest strips. The point at which all growth was completely inhibited was observed to determine the MIC of individual drugs and drug combinations. The Etest strip's inhibition zone intersection with the scale was used to calculate the minimum inhibitory concentration (MIC) [12].
Data Storage and Analysis:
IBM SPSS software version 20.0 was used to conduct the statistical analysis (IBM Corp.; Armonk, NY). The qualitative data were described using numbers and percentages. The findings were considered significant at a level of 5% (p < 0.05). The chi-square test was used to compare categorical groups, and Fisher's exact was used to adjust the chi-square test when more than 20% of the cells had an expected value of less than 5. The following formula was used to determine the fractional inhibitory concentration index (FICI) for each antibiotic in the combination: FICA + FICB equals FICI. FICA represents the MIC of ATM in combination divided by the MIC of ATM alone, and FICB represents the MIC of CZA in combination divided by the MIC of CZA alone. The FICIs have been interpreted as follows: Synergy = FICI ≤0.5, Additivity = FICI >0.5 to ≤1, No interaction (indifference) = FICI >1 to ≤4, and Antagonism = FICI >4.
Results![]()
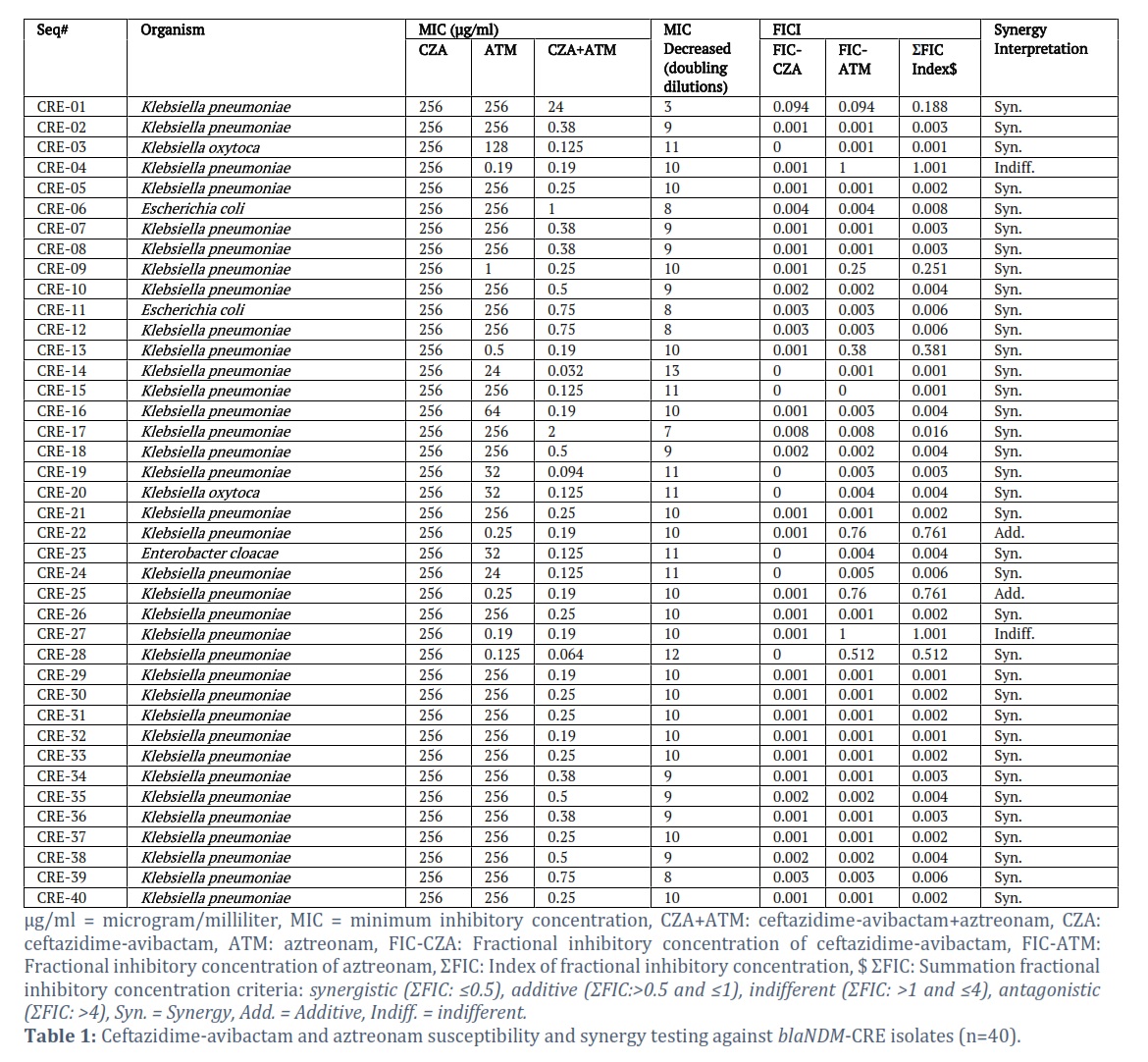
Using the agar-based Etest fixed ratio method, the recent study assessed the in vitro synergy between CZA and ATM against 40 Enterobacterales isolates, blaNDM. K. pneumoniae (n=35, 87.5%), E. coli, and K. oxytoca (n=2, 5%) each (Total= 10%), respectively, and 2.5% (n=1) E. cloacae were the main isolates (data not shown here). Table 1 displays the MIC distributions by Etest for CZA, ATM, and CZA+ATM, besides this, fractional inhibitory concentration index values for each tested isolate are shown along with interpretation Test results for all 40 isolates showed CZA resistance (100%) when tested alone, while 17.5% of isolates exhibited aztreonam resistance alone (n=7). In 90% of the tested isolates (n=36/40), the combination of CZA and ATM demonstrated synergistic effects. The decrease in MIC after CZA and ATM synergy is displayed in Table 1, the lowest and highest MIC decreases were observed to be 3 and 13 doubling dilutions, respectively (Table 1).
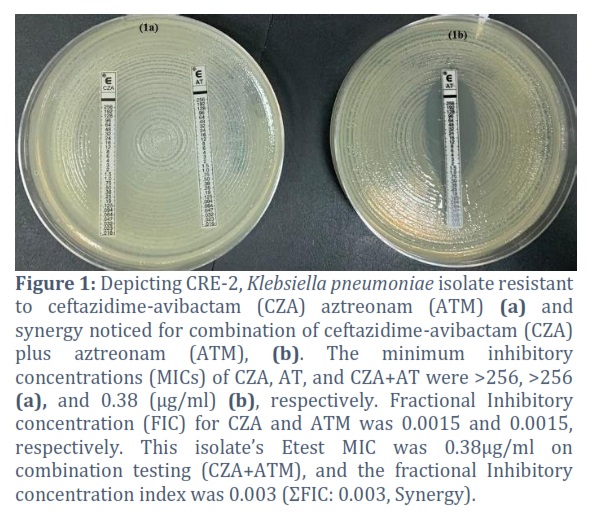
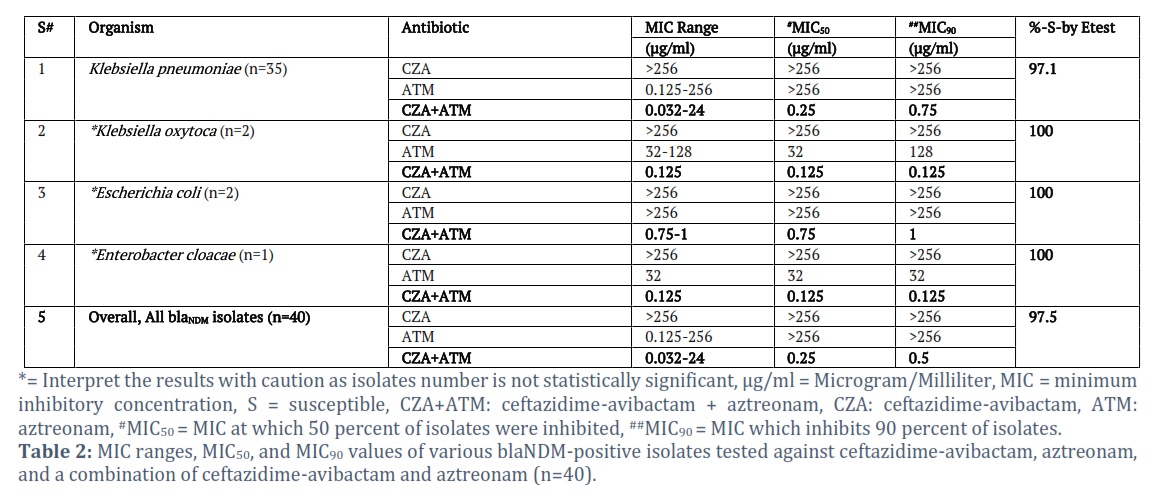
K. pneumoniae (n=35), MIC range, MIC50, MIC90 against CZA+ATM: 0.032-24, 0.25, and 0.75, respectively. Out of the 35 tested K. pneumoniae isolates, 97.1% of isolates were susceptible to the combination Etest method. Overall, all tested isolates exhibited very satisfactory results against CZA+ATM, as shown by the MIC range, MIC50, and MIC90 of 0.032-24, 0.25, and 0.5, respectively (Table 2). Figure 1 shows susceptibility testing of CRE-2, K. pneumoniae isolate showing resistance to CZA and ATM, however, synergy is noticed for the combination of CZA+ATM.
This isolate’s combination Etest value was 0.38µg/ml. The fractional Inhibitory concentration index was 0.003 (ΣFIC: 0.003, Synergy).
Figures & Tables
Carbapenem-resistant Enterobacterales strains pose a significant and widespread risk to public health worldwide. The production of serine and metallo-beta lactamases, such as KPC, NDM, VIM, IPM, and OXA-48-like enzymes, is the primary cause of resistance to carbapenems that are used as a last resort in this species. Metallo-β-lactamases (MBL) production in gram-negative bacteria is a well-known trait, causing deadly infection worldwide, with a potential to disseminate quickly [20, 21]. From 2007 to 2016, the rate of carbapenem resistance among K. pneumoniae in Saudi Arabia increased from 0% to 33.3%, making it the most resistant Enterobacterales species [22]. K. pneumoniae isolates from Saudi Arabia are resistant to carbapenems due to their acquisition of OXA-48-like and NDM carbapenemases, with few recent studies detecting KPC carbapenemases [23, 24]. Our results corroborate previous microbiological studies indicating the higher prevalence of blaMBL in K. pneumoniae than any other member of Enterobacterales [25]. Due to the coexistence of numerous carbapenemases and co-resistance to tigecycline, β-lactams, aminoglycosides, quinolones, and colistin, few treatment options are available, which poses a significant therapeutic challenge. Hospitalizations, morbidity, and death rates related to pan-drug-resistant (PDR) K. pneumoniae infections that are resistant to traditional treatment have surged worldwide in recent times. [26]. Several studies are reporting the effectiveness of CZA + ATM therapy in comparison with other active antibiotic groups [27]. The Infectious Disease Society of America (IDSA) has recommended the use of CZA with ATM for the management of clinical infections due to MBL producers. Other treatment options for MBL producers include ATM in combination with meropenem-vaborbactam, cefiderocol, polymyxin B (in combination therapy for non-UTI infections), and polymyxin E (colistin) for UTI only. It is imperative to contact the microbiology laboratory for in vitro testing of the synergy between CZA+ ATM [28]. This study investigated ATM and CZA synergy against Enterobacterales that produce blaMBL. All isolates were CZA-resistant due to blaMBL. However, synergy against all isolates was observed when tested in synergy with ATM. Numerous studies [29-31] have documented the synergy between CZA and ATM.
We used the fixed ratio method and found it efficient for calculating synergies between two antimicrobials. Various studies have been performed using the Etest synergy method and researchers have found these methods useful, reliable, and comparable to agar dilution and broth dilution methods. [32, 33]. The interpretation of synergy by fractional inhibitory concentration index showed synergy in 90% of the isolates. Among the remaining, 5% of the isolates showed an additive effect while the other 5% showed no interaction. No antagonism was observed, thus it may be safer to use this antimicrobial regimen, however, further extensive studies are warranted to further understand this aspect and it could be interesting to test these combinations on strains with additional resistance mechanisms, such as blaVIM and blaIPM-producing strains. The addition of ATM to CZA decreased the CZA MIC from 3 folds to 13 folds among various isolates.
Consider these points when interpreting our findings: First, these experiments only used Enterobacterales isolates with K. pneumoniae predominance. Second, the study excluded non-fermenter bacteria like P. aeruginosa. Given the lack of agents that kill blaNDM-producing Enterobacterales, we wanted to show that CZA and ATM work together and suggest it as a treatment [26]. The results should be interpreted with caution, as all studies of this type need more work to characterize CZA with ATM's effectiveness against blaMBL-producing Gram-negative pathogens. Although this study had many K. pneumoniae isolates, only two blaNDM-producing Klebsiella oxytoca, two E. coli, and one E. cloacae were tested. We suggest further research into blaNDM-producing Enterobacterales isolates and non-Enterobacterales isolates, particularly those with co-occurring β-lactamases. The findings may not apply to Enterobacterales isolates with other blaMBL like blaVIM or blaIMP. The results may not apply to other blaMBL-producing pathogens like P. aeruginosa and A. baumannii, which have more intrinsic, acquired, and adaptive resistance mechanisms than K. pneumoniae and E. coli. Finally, these combination regimens need human clinical efficacy and safety testing.
Taken together, blaMBL-producing pathogens remain a major challenge despite recent advancements in the treatment of carbapenem-resistant organisms. ATM can resist the blaMBL-mediated hydrolysis, but co-harbored serine beta-lactamases (KPC, OXA-48, and ESBL) make ATM ineffective, requiring combination therapy. Our study showed that CZA and ATM synergistically inhibited blaNDM-producing Enterobacterales isolates. Similar to all studies of this type, more extensive experiments against a variety of Gram-negative pathogens with different blaMBLs with different hydrolytic capabilities and other resistance mechanisms are needed to determine the efficacy of this combination regimen. Finally, CZA and ATM clinical efficacy and safety must be established in clinical trials, and current use should be based on a risk versus benefit model.
Author Contributions
Absar M, Marie M, and Arshad M conceived the research idea and designed the experiment.
AlAnazi N, Alfuraydi A run the experiment
Absar M, Arshad M collected and analyzed the data, and wrote the manuscript draft.
S Ali and Marie M, Binkhamis K, Arshad M revised and edited the manuscript.
All authors read and approved the final version of the manuscript.
The author declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- Jean SS, Gould IM, Lee WS, Hsueh PR. New Drugs for Multidrug-Resistant Gram-Negative Organisms: Time for Stewardship. Drugs, (2019); 79: 705-714.
- Wang B, Pan F, Wang C, Zhao W, Sun Y, et al. Molecular epidemiology of Carbapenem-resistant Klebsiella pneumoniae in a paediatric hospital in China. International Journal of Infectious Diseases, (2020); 93: 311-319.
- Alotaibi F. Carbapenem-Resistant Enterobacteriaceae: An update narrative review from Saudi Arabia. Journal of Infection and Public Health, (2019); 12(4): 465-471.
- Lee CR, Lee JH, Park KS, Kim YB, Jeong BC, et al. Global Dissemination of Carbapenemase-Producing Klebsiella pneumoniae: Epidemiology, Genetic Context, Treatment Options, and Detection Methods. Frontiers in Microbiology, (2016); 7: 895.
- Wang Z, Ma K, Chen Z, Guo Z, Zhao G, et al. Successful Treatment of Early Post-Transplant Bloodstream and Pulmonary Infection Caused by Carbapenem-Resistant Klebsiella pneumoniae With a Combination of Ceftazidime-Avibactam and Carbapenem: A Case Report. In Transplantation Proceedings, (2020); 52(9): 2742-2746.
- Munoz-Price LS, Poirel L, Bonomo RA, Schwaber MJ, Daikos GL, et al. Clinical epidemiology of the global expansion of Klebsiella pneumoniae carbapenemases. The Lancet Infectious Diseases, (2013); 13(9): 785-796.
- Mantilla-Calderon D, Jumat MR, Wang T, Ganesan P, Al-Jassim N, et al. Isolation and Characterization of NDM-Positive Escherichia coli from Municipal Wastewater in Jeddah, Saudi Arabia. Antimicrobial Agents and Chemotherapy, (2016); 60(9): 5223-5231.
- Bush K, Jacoby GA. Updated functional classification of β-lactamases. Antimicrobial Agents and Chemotherapy, (2010); 54(3): 969-976.
- Bush K. Past and Present Perspectives on β-Lactamases. Antimicrobial Agents and Chemotherapy, (2018); 62(10): e01076-18.
- Bush K. A resurgence of β-lactamase inhibitor combinations effective against multidrug-resistant Gram-negative pathogens. International Journal of Antimicrobial Agents, (2015); 46(5): 483-493.
- Kazmierczak KM, Bradford PA, Stone GG, de Jonge BLM, Sahm DF. In Vitro Activity of Ceftazidime-Avibactam and Aztreonam-Avibactam against OXA-48-Carrying Enterobacteriaceae Isolated as Part of the International Network for Optimal Resistance Monitoring (INFORM) Global Surveillance Program from 2012 to 2015. Antimicrobial Agents and Chemotherapy, (2018); 62(12): e00592-18.
- Davido B, Fellous L, Lawrence C, Maxime V, Rottman M, et al. Ceftazidime-Avibactam and Aztreonam, an Interesting Strategy To Overcome β-Lactam Resistance Conferred by Metallo- β-Lactam resistance conferred by metallo-β-lactamases in Enterobacteriaceae and Pseudomonas aeruginosa. Antimicrobial Agents and Chemotherapy, (2017); 61(9): e01008-17.
- Marshall S, Hujer AM, Rojas LJ, Papp-Wallace KM, Humphries RM, et al. Can Ceftazidime-Avibactam and Aztreonam Overcome β-Lactam Resistance Conferred by Metallo-β-Lactamases in Enterobacteriaceae? Antimicrobial Agents and Chemotherapy, (2017); 61(4): e02243-16.
- Bocanegra-Ibarias P, Camacho-Ortiz A, Garza-González E, Flores-Treviño S, Kim H, et al. Aztreonam plus ceftazidime-avibactam as treatment of NDM-1-producing Klebsiella pneumoniae bacteraemia in a neutropenic patient: Last resort therapy? Journal of Global Antimicrobial Resistance, (2020); 23: 417-419.
- Rosa R, Rudin SD, Rojas LJ, Perez-Cardona A, Aragon L, et al. Application of "Precision Medicine" Through the Molecular Characterization of Extensively Drug-Resistant Klebsiella pneumoniae in a Multivisceral Transplant Patient. Clinical Infectious Diseases, (2017); 65(4): 701-702.
- Pragasam AK, Veeraraghavan B, Shankar BA, Bakthavatchalam YD, Mathuram A, et al. Will ceftazidime/avibactam plus aztreonam be effective for NDM and OXA-48-Like producing organisms: Lessons learnt from In vitro study. Indian journal of medical microbiology, (2019); 37(1): 34-41.
- Zhang W, Guo Y, Li J, Zhang Y, Yang Y, et al. In vitro and in vivo bactericidal activity of ceftazidime-avibactam against Carbapenemase-producing Klebsiella pneumoniae. Antimicrobial Resistance and Infection Control, (2018); 7: 142.
- Emeraud C, Escaut L, Boucly A, Fortineau N, Bonnin RA, et al. Aztreonam plus Clavulanate, Tazobactam, or Avibactam for Treatment of Infections Caused by Metallo-β-Lactamase-Producing Gram-Negative Bacteria. Antimicrobial Agents and Chemotherapy, (2019); 63(5): e00010-19.
- Wayne PA. Performance standards for antimicrobial susceptibility testing 30th ed. 2020; 294. Clinical and Laboratory Standards Institute
- Logan LK, Bonomo RA. Metallo-β-Lactamase (MBL)-Producing Enterobacteriaceae in United States Children. In Open forum infectious diseases. (2016); 3(2): ofw090.
- Padhi S. New Delhi metallo-beta-lactamase: a weapon for the newly emerging drug-resistant bacteria. Indian Journal of Medical Sciences, (2011); 65(8): 317-320.
- Balkhy HH, El-Saed A, Alshamrani MM, Alsaedi A, Al Nasser W, et al. Ten-year resistance trends in pathogens causing healthcare-associated infections; reflection of infection control interventions at a multi-hospital healthcare system in Saudi Arabia, 2007-2016. Antimicrobial Resistance and Infection Control, (2020); 9(1): 1-12.
- Alghoribi MF, Binkhamis K, Alswaji AA, Alhijji A, Alsharidi A, et al. Genomic analysis of the first KPC-producing Klebsiella pneumoniae isolated from a patient in Riyadh: A new public health concern in Saudi Arabia. Journal of Infection and Public Health, (2020); 13(4): 647-650.
- Hala S, Antony CP, Alshehri M, Althaqafi AO, Alsaedi A, et al. First report of Klebsiella quasipneumoniae harboring bla (KPC-2) in Saudi Arabia. Antimicrobial Resistance and Infection Control, (2019); 8: 1-8.
- van Duin D, Doi Y. The global epidemiology of carbapenemase-producing Enterobacteriaceae. Virulence, (2017); 8(4): 460-469.
- Karakonstantis S, Kritsotakis EI, Gikas A. Pandrug-resistant Gram-negative bacteria: a systematic review of current epidemiology, prognosis and treatment options. Journal of Antimicrobial Chemotherapy, (2020); 75(2): 271-282.
- Falcone M, Daikos GL, Tiseo G, Bassoulis D, Giordano C, et al. Efficacy of Ceftazidime-avibactam Plus Aztreonam in Patients With Bloodstream Infections Caused by Metallo-β-lactamase-Producing Enterobacterales. Clinical infectious diseases, (2021); 72(11): 1871-1878.
- Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, et al. Infectious Diseases Society of America 2023 Guidance on the Treatment of Antimicrobial Resistant Gram-Negative Infections. Clinical infectious diseases, (2023); ciad428.
- de Jonge BL, Karlowsky JA, Kazmierczak KM, Biedenbach DJ, Sahm DF, et al. In Vitro Susceptibility to Ceftazidime-Avibactam of Carbapenem-Nonsusceptible Enterobacteriaceae Isolates Collected during the INFORM Global Surveillance Study (2012 to 2014). Antimicrobial Agents and Chemotherapy, (2016); 60(5): 3163-3169.
- Li H, Estabrook M, Jacoby GA, Nichols WW, Testa RT, et al. In vitro susceptibility of characterized β-lactamase-producing strains tested with avibactam combinations. Antimicrobial Agents and Chemotherapy, (2015); 59(3): 1789-1793.
- Gomez-Simmonds A, Nelson B, Eiras DP, Loo A, Jenkins SG, et al. Combination Regimens for Treatment of Carbapenem-Resistant Klebsiella pneumoniae Bloodstream Infections. Antimicrobial Agents and Chemotherapy, (2016); 60(6): 3601-3607.
- Hellmark B, Unemo M, Nilsdotter-Augustinsson A, Söderquist B. In vitro antimicrobial synergy testing of coagulase-negative staphylococci isolated from prosthetic joint infections using Etest and with a focus on rifampicin and linezolid. European Journal of Clinical Microbiology & Infectious Diseases, (2010); 29: 591-595.
- Wenzler E, Deraedt MF, Harrington AT, Danizger LH. Synergistic activity of ceftazidime-avibactam and aztreonam against serine and metallo-β-lactamase-producing gram-negative pathogens. Diagnostic Microbiology and Infectious Disease , (2017); 88(4): 352-354.
![]()