

Full Length Research Article
Association of Celiac Disease and H. pylori Infection with ATG5 Polymorphism and Interleukin-33
Omar Atrooz1,2*, Sura Mumtaz3, Ahmed Abood4, Ansam Atrooz5
Adv. life sci., vol. 11, no. 4, pp. 849-855, November 2024
*– Corresponding Author: Omar M. Atrooz (omihandd@gmail.com)
Authors' Affiliations
2. Department of Biological Sciences, Mutah University, Mutah – Jordan
3. Department of Pathological Analyzes, Samarra University, Samarra – Iraq
4. Department of Biology, College of Education, Iraqi University, Baghdad – Iraq
5. Department of Pediatric, Pediatric Resident, Faculty of Medicine, Mutah University – Jordon
[Date Received: 31/03/2024; Date Revised: 09/07/2024; Date Published: 15/10/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Celiac disease (CD) is an inflammatory small intestine autoimmune disease. The study aims to investigate the association and the detection of ATG5 polymorphism between celiac disease (CD) and H. pylori infection, and the association with Interleukin-33 (IL-33).
Methods: The study groups included patients from Iraq, ages 4 to 35. Two primary patient groups were created: sixteen had positive H. pylori and celiac disease, and thirty had positive CD and negative H. pylori disease. The levels of tissue transglutaminase IgA (TTG IgA), H. pylori IgG, and IL-33 were measured using the ELISA method. The primers were amplified using PCR.
Results: With celiac disease, the patient group's TTG IgA levels increased dramatically. The test also showed significant variations (P=0.054) in the H. pylori IgG levels between the patient and control groups. The H. pylori seropositivity test showed a statistically significant difference (p ≤0.033) between seropositive and seronegative individuals, while the patient group's IL-33 levels did not significantly differ (P ≤0.299) from the control group.
Conclusions: Our results showed that CD is more common in women and occurs in the age range of 24-35 years. It also showed that the mutant variant of ATG5 is associated with CD, and the significance of H. pylori IgG serum levels in the patient group may indicate that the bacteria involved in CD. Furthermore, H. pylori infection is more strongly linked to serum IL-33 levels than CD.
Keywords: Celiac disease; H. pylori; PCR; IL-33; ATG5 polymorphism
Introduction![]()
CD is a chronic autoimmune disorder triggered by gluten in genetically predisposed individuals, specifically those with HLA DQ2 and/or DQ8 alleles [1-3]. CD is the most common inflammatory autoimmune disease affecting the intestines. Recent epidemiological research [3,4,5] shows that prevalence rates in emerging economies, especially in Africa, the Middle East, and India, are comparable to those in Europe. The current diagnosis guidelines for CD include demonstrating enteropathy in small intestine biopsies, determining the specific antibodies that are circulating, and doing historical investigations [1, 6]. Helicobacter pylori (H. pylori), a common stomach infection bacterium, is thought to infect over half of the world's population [7]. Infants are more likely to get H. pylori infection, which typically lasts until treatment. Although it can cause iron deficiency anemia, peptic ulcer disease, and chronic immunological thrombocytopenic purpura, the majority of infected children and adolescents do not exhibit any symptoms [8]. 95% specificity and sensitivity can be achieved by histologically identifying H. pylori in stomach tissues; however, suitable sampling and interpretation are required. A biological process known as autophagy governs the majority of cells. Numerous illnesses, including liver disease, heart disease, inflammatory and neurological disorders, and cancer, are associated with its process. Several cytokines have a significant impact on autophagy as a result of inflammatory and immunological reactions [9]. Autophagy, regulated by ATG genes like ATG5, is crucial for cellular homeostasis and is implicated in various diseases, including CD [10,11]. ATG5 polymorphisms have been linked to multiple autoimmune disorders [12,13].
IL-33 is a cytokine that promotes Th2 responses and is released by damaged cells, playing a significant role in immune regulation and potentially in CD pathogenesis [14,15].
The study aimed to investigate the association between CD and H. pylori infection. In addition, find out the difference in the levels of antibodies against H. pylori in patients and investigating the association of H. pylori IgG with CD diagnostic markers (TTG IgA). Furthermore, to study the genetic polymorphism of ATG5 in celiac patients in the presence or absence of H. pylori infection. Finally, to investigate the association of IL-33 with CD diagnostic markers (TTG IgA) and H. pylori infection (H. pylori IgG).
Methods![]()
Sample size and study groups
From January 28, 2021, to September 1, 2021, 70 participants—46 females and 24 males—were divided into study groups. The participants' ages ranged from 4 to 36 years old. The patients provided some information by answering a questionnaire that the researchers had created, which included the following information: personal information, presence of autoimmune diseases, inflammatory diseases, antibiotics intake within the last two weeks, gastric treatment, family history, histological test, and the using of nonsteroidal anti-inflammatory drugs (NSAIDs): aspirin, naproxen, indomethacin, etc. A total of 46 CD patients who had been diagnosed by specialists at Iraqi hospitals were included in the study, along with 24 visitors to the hospital who appeared healthy on the outside (control group).
Inclusion criteria, exclusion criteria, and limitations
This cross-sectional study included patients with celiac disease of any age or gender, with or without H. pylori infection. Patients with inflammatory or autoimmune illnesses, those who had used antibiotics during the previous two weeks and those who used NSAIDs, proton pump inhibitors, or other medications that targeted the stomach were not included in the study.
The period of coronavirus restrictions presented significant limitations for our research. We faced a low number of celiac cases referred to the hospitals, as well as curfews and travel restrictions that made it difficult to recruit participants. Additionally, taking blood samples from apparently healthy individuals during the coronavirus pandemic was also challenging, and contributed to a lower overall sample size. Notwithstanding these drawbacks, we think that our research offers insightful information about the risk factors and prevalence of CD in our community. We have taken steps to address the lower sample size, including conducting sensitivity analyses to ensure that our results are robust and providing detailed information on the recruitment challenges faced during the study.
Specimen’s collection
Five to ten milliliters of blood were drawn from each patient. For the Polymerase Chain Reaction (PCR) test, each sample was split into two tubes: an EDTA tube and a blank tube. The blank tube was allowed to coagulate before the serum was separated using a 10-minute centrifugation. In addition, the serum was divided among three Eppendorf tubes and kept cold (–20 °C) until the ELISA analyses were completed. On the same day, the leftover blood is used for the H. pylori rapid test.
Ethical consideration
Patients or their families provided ethical authorization, which was received from the Medical City Department and the Research Committee of the Baghdad Health (Al-Rusafa Department). The purpose of collecting the sample was explained to the patients.
ELISA analysis
The analysis and determinations of TTG IgA (DE7720, Demeditec Diagnostics GmbH, Germany), H. pylori IgG (0322 REF HPG, INSCAGG, CE, Dia. Pro Diagnostic Bio probe, SrI, Italy), and IL-33 (SEB980Ra, Cloud Clone Corporation, Belgium) were done by kit protocols of ELISA technique.
Gene detection and sequencing
After amplification, the data was analyzed using the generous program to ascertain the sequencing variance between samples of a particular gene (ATG-5). DNA extraction, PCR amplification, sequencing, and assembly are all steps in the process. The ABIO pure Extraction technique was followed when extracting DNA.
Lyophilized primers rs510432-F and rs510432-R (detailed below) (Macrogen Company, Korea) were dissolved in nuclease-free distilled water to obtain 100 pmol/µl of stock solution. The primer working solution was prepared by adding 10 µl of the stock solution to 90 ml of nuclease-free distilled water to have a solution of 10 pmol/µl. PCR amplification (Thermal Cycler, Bio-Rad, USA) and thermal cycling were performed as illustrated by instructions and protocol.
|
Primer name |
Sequence |
|
rs510432-F |
5′-TGTAAAACGACGGCCAGTTTAGTCCAACTCCAAGAAGA-3′ |
|
rs510432-R |
5′-CAGGAAACAGCTATGACCAAACCTCTCCAAGTTCATAG-3′ |
The automated DNA sequencer (ABI3730XL, Macrogen Corporation, Korea) was used to perform Sanger sequencing on the PCR products after they were transmitted to Macrogen Corporation Company. Geneious software was used to examine the results that were acquired.
Data analysis
The statistical program SPSS (Version 28) was used for statistical analysis. Based on its nature and type, the raw data was categorized. Various statistical tests, both parametric and non-parametric, were employed based on how well the requirements were met.
Results![]()
Study group samples for infected CD
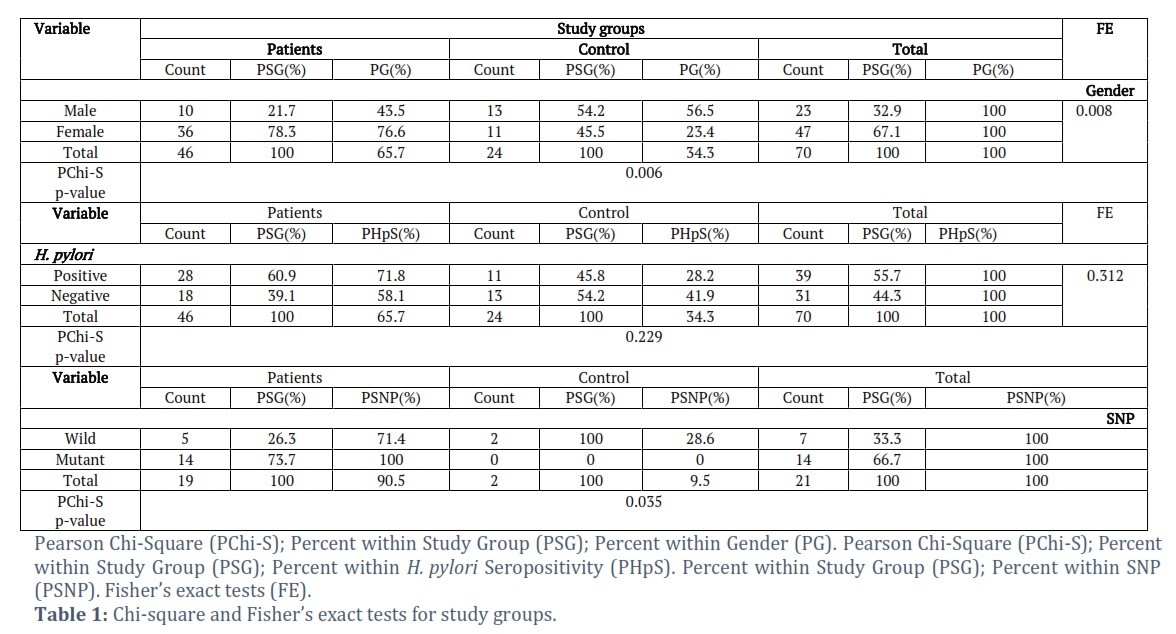
There were 70 samples in total; 46 patients (65.7%) and 24 control subjects (34.3%) made up the patient group. The study's focus was on the age ranges of 5 to 35 years old, with a total of 23 (32.9) men and 47 (67.1%) females in this age range (Table 1).
Age groups
The study's cases were divided into three age groups (G): G1 (ages 5 to 14), G2 (15 to 24), and G3 (ages 25 to 35). According to Table 1, the most common infection among patients was G3, with G3 = 19 (8.74%) being greater than G1 = 16 (7.36%) and G2 = 11 (5.06%).
Celiac disease
The ELISA test was used to perform diagnostic tests for CD. The study's findings show that the patients' mean ± SD serum TTG IgA concentration was 23.67389± 6.658566 U/ml, compared to 1.86750± 1.191908 U/ml in the control group (Table 2). When compared to the control group's serum levels, the TTG-IgA levels in the patient's serum were statistically considerably higher (P<0.001) in the current study.
H. pylori seropositivity
The results of the study group's H. pylori seropositivity (positive and negative) patients were 28 (60.9%), and 18 (39.1%), respectively, compared to the control group's 11 (45.8%) and 13 (54.2%). No significant differences were found in either the Pearson Chi-Square or Fisher's Exact Tests (Table 1).
Interleukin-33
The serum IL-33 concentrations in the patients (1.00727±2.445775 pg/ml) and the control group (0.73347±.904229 pg/ml) are shown in Table 2 as the mean ± SD.
ATG5 polymorphism analysis
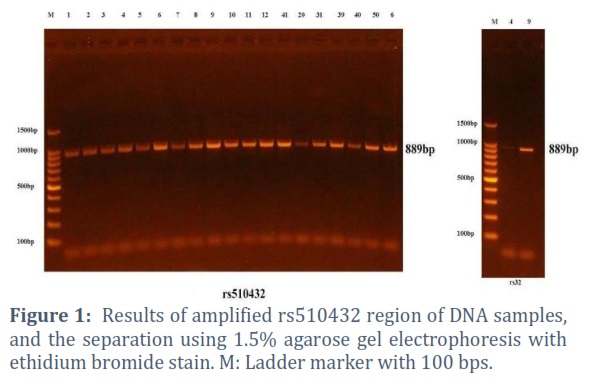
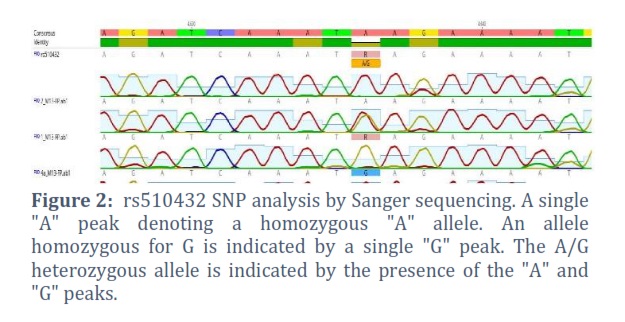
Twenty-one samples—nine from the patient’s group and two from the control group—were used in the genetic polymorphism study. Seven have wild-type AA and fourteen have mutant-type AG according to the data of rs510432. Significant findings (p=0.035) are shown in Figures 1 and 2 and Table 1. Patients of the wild and mutant types (26.3% and 73.7%, respectively), as well as the control wild and mutant types (100.0% and 0.0%, respectively), comprise the study group.
Correlation between study variables
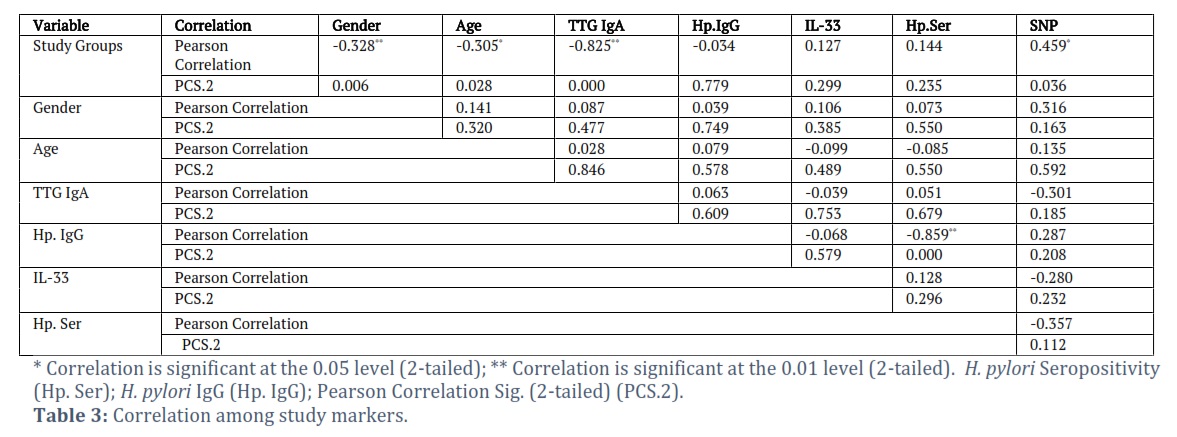
The research group and gender, age, and SNP showed a statistically significant low negative connection (p-value = -0.328, 0.006; -0.305, 0.028; -0.459, 0.036) (Table 3).
Figures & Tables

Gluten is a trigger for the disease CD, which is influenced by environmental factors as well as a human genetic predisposition. Less than 2.0% of people in the general population have CD [16]. Within study groups, the proportion of females affected by CD was found to be higher than that of males; in the patients’ group, this was 78.3% of the total, whereas, in the control group, this was 45.8% of the total, with males making up 54.2%. These findings are consistent with [17], where the authors noted that the frequency of CD was twice as high in females (68.75%) as it was in males (31.25%) and that the immunoregulation mechanisms linked to varying hormone levels across genders explained this discrepancy. Our results were not in line with the findings of the Seattle Children’s Hospital study by Dickerson et al., [18], which reported that 55% of patients were male and 45% were female. The size of the study sample and differences in ethnic groups may be the source of this gender discrepancy in the patients.
Additionally, the age group analysis results agreed with Khatoon et al., [19] study, which found that about 75% of CD patients were at an age less than 40 years old, and the highest percentage of prevalence (11.81%) was the age group between 20 and 30 years old. This finding may be due to the presence of 88.3% of patients who have iron deficiency anemia [17]. However, our findings contradict the findings of the Khan et al., [19] study, which indicates that all positive indicators were detected in patients younger than 15 years old, possibly as a result of their predominantly wheat-based diet.
The results of TTG IgA concentrations are in agreement with Abdullah and Al-Bhawani [20], who observed that there was a higher proportion of TTG IgA patients (38%) as compared to the control group (0.0%). However, the findings of Ertekin et al., [5], who studied 1263 Turkish children on a wheat-based diet, disagree, with the finding that only 11 of the children had positive TTG IgA with seropositivity of 0.87%. There may be differences between our study and earlier research because of the patient sample size, the study population, the groups that were chosen, and the symptoms of the patients.
Antibodies against H. pylori in human serum are indicators of infection. Reports from several nations have confirmed the diagnosis of positive H. pylori IgG findings with high sensitivity and specificity. Nonetheless, the outcomes vary among nations, particularly between wealthy and poor nations. These discrepancies could result from various ideal cut-off values for IgG levels as opposed to the cut-off established by the supplier of the H. pylori antibody serologic test kit. For different populations or subgroups, the manufacturer's optimal cut-off value might not always be appropriate. The manufacturer's recommended IgG cut-off point was 0–5 IU/mL, as per the instructions provided. Significant differences (p=0.054) in H. pylori IgG were found between the patient and control groups based on statistical analysis and a non-parametric test (Table 1). According to Bayrak et al., [21], there is low evidence of a link (P<0.01) between H. pylori infection and CD patients. Our results conflict with those of Simondi et al., [22], who found that compared to controls (41%), there was a 36% correlation between CD patients and H. pylori and a 19% correlation between CD patients and patients with duodenal intraepithelial lymphocytosis. Our findings indicate that there is no discernible difference between CD patients and controls and those with H. pylori infection. However, Obaidat et al., [23] found that there is a significant seroprevalence (88.6%) in the Jordanian population.
When compared to the control group, the serum levels of IL33 in the patients did not differ significantly (P≤0.299). This finding is consistent with the findings of Abaas et al., [24], but it is at odds with the findings of López-Casado et al., [25], who found that the serum levels of IL-33 in celiac patients were significantly higher than in the control group (p=0.05). A statistically significant difference (p ≤0.033) was found between seropositive and seronegative participants when IL-33 serum levels were analyzed in connection with H. pylori seropositivity (Asymptotic Sig., two-sided test). Our findings were consistent with a prior study that found that patients with peptic ulcers had a considerably higher amount of IL-33 in their serum compared to the uninfected group (P = 0.001) [26].
The study of ATG5 polymorphisms revealed that 7 had wild-type AA and 14 had mutant-type AG. Results from a prior study indicated that genotypes (AA+GA) bearing rs510432 allele A were independently linked to cirrhosis compared to chronic hepatitis viral infection without HCC [27]. The ATG5 rs510432 A allele frequency was found to be significantly higher in severe sepsis shock than in mild sepsis in another study [28]. This suggests that the rs510432 G allele, rather than the A allele, within the promoter of the ATG5 gene influences the progression of sepsis from mild to severe sepsis shock.
Lastly, a modest negative connection was found between the study group and SNP, gender, and age in the correlation analysis of the research variables. A variant in the gene that distinguishes patients from healthy individuals may be the cause of the association between the SNP and the study groups. Furthermore, there was a statistically significant negative connection (Pearson connection, p-value = -0.825, 0.000) between the TTG antibody levels and the research groups. The patients are interacting with the control group in a downward direction.
Our research showed that CD is more common in women and has the highest frequency in the 24- to 35-year-old age range. Our study highlights the significant association of ATG5 polymorphism with CD and suggests that H. pylori infection may play a role in CD pathogenesis. Further research into larger sample sizes is warranted to confirm these findings.
Author Contributions
The data collection and experiments were done by Sura Mumtaz. Ahmad Abood and Ansam Atrooz did all the statistical analysis and formulated the ideas, research goals, and aims. Omar Atrooz supervised the research and prepared, revised, and edited the article.
Acknowledgements
The authors express their gratitude to all the affiliated staff members who made any kind of contribution to this research.
The author declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- Serena G, Lima R, Fasano A. Genetic and environmental contributors to celiac disease. Current Allergy and Asthma Reports, (2019); 19(9): 1-10.
- Tokgöz Y, Terlemez S, Karul A. Fat-soluble vitamin levels in children with newly diagnosed celiac disease, a case-control study. BMC Pediatrics, (2018); 18(1): 1-5.
- Lionetti E, Catassi C. New clues in celiac disease epidemiology, pathogenesis, clinical manifestations, and treatment. International reviews of immunology, (2011); 30(4): 219-231.
- Abu-Zekry M, Kryszak D, Diab M, Catassi CF. Prevalence of celiac disease in Egyptian children disputes the east-west agriculture-dependent spread of the disease. Journal of pediatric gastroenterology and nutrition, (2008); 47(2): 136-140.
- Ertekin V, Selimoglu MA, Kardas F, Aktas E. Prevalence of celiac disease in Turkish children. Journal of clinical gastroenterology, (2005); 39(8): 689-691.
- Tye-Din JA, Galipeau HJ, Agardh D. Celiac disease: a review of current concepts in pathogenesis, prevention, and novel therapies. Frontiers in pediatrics, (2018); 6: 350.
- Guevara B, Cogdill AG. Helicobacter pylori: a review of current diagnostic and management strategies. Digestive Diseases and Sciences, (2020); 65(7): 1917-1931.
- Crowe SE. Helicobacter pylori infection. New England Journal of Medicine, (2019); 380(12): 1158-1165.
- Ge Y, Huang M, Yao YM. Autophagy and proinflammatory cytokines: interactions and clinical implications. Cytokine & growth factor reviews, (2018); 43: 38-46.
- Nikseresht M, Shahverdi M, Dehghani M, Abidi H, Mahmoudi R, et al. Association of single nucleotide autophagy‐related protein 5 gene polymorphism rs2245214 with susceptibility to non–small cell lung cancer. Journal of Cellular Biochemistry, (2019); 120(2): 1924-1931.
- Ye X, Zhou XJ, Zhang H. Exploring the role of autophagy-related gene 5 (ATG5) yields important insights into autophagy in autoimmune/autoinflammatory diseases. Frontiers in immunology, (2018); 9: 2334.
- van Beek N, Klionsky DJ, Reggiori F. Genetic aberrations in macroautophagy genes leading to diseases. Biochimica et Biophysica Acta (BBA)-Molecular Cell Research, (2018); 1865(5): 803-816.
- Zhang Y, He X, Li J, Yang W, Cui Y, et al. Functional genetic variant in ATG5 gene promoter in acute myocardial infarction. Cardiology Research and Practice, (2020); 2020 (1): 9898301.
- Perez F, Ruera CN, Miculan E, Carasi P, Dubois-Camacho K, et al. IL-33 alarmin and its active proinflammatory fragments are released in small intestine in celiac disease. Frontiers in immunology, (2020); 11: 581445.
- Cayrol C, Girard JP. Interleukin‐33 (IL‐33): a nuclear cytokine from the IL‐1 family. Immunological reviews, (2018); 281(1): 154-168.
- Valitutti F, Cucchiara S, Fasano A. Celiac disease and the microbiome. Nutrients, (2019); 11(10):2403.
- Khatoon S, Ahmed A, Yousaf S. Iron deficiency anemia in Pakistan: Celiac disease an underlying cause. Journal of Ayub Medical College Abbottabad, (2018); 30(3): 372-376.
- Dickerson JA, Lee D, Pacheco MC. Deamidated gliadin peptide in pediatric patients with moderately increased tissue transglutaminase; does it help? Clinica Chimica Acta, (2019); 492: 20-22.
- Khan A, Ahmad W, Kamran M. Celiac Disease in Different Age Groups and Genders in Pakistan. Journal of Rawalpindi Medical College, (2018); 22(3): 244-247.
- Abdullah H, Thawani A. Association of celiac disease with HLA-DRB1 and HLADQB1 alleles in a sample of Iraqi patients. Iraqi Journal of Biotechnology, (2012); 11: 529-36.
- Bayrak NA, Tutar E, Volkan B, Sahin AB, Polat E, et al. Helicobacter pylori infection in children with celiac disease: Multi‐center, cross‐sectional study. Helicobacter, (2020); 25(3): e12691.
- Simondi D, Ribaldone DG, Bonagura GA, Foi S, Sapone N, et al. Helicobacter pylori in celiac disease and in duodenal intraepithelial lymphocytosis: Active protagonist or innocent bystander? Clinics and Research in Hepatology and Gastroenterology, (2015); 39(6):740–745.
- Obaidat MM, Roess AA. First nationwide seroepidemiology and risk factors report of Helicobacter pylori in Jordan. Helicobacter, (2019); 24(3): e12572.
- Abass EA. Relationship Between Interleukin-33 (IL-33) and C-Reactive Protein in Iraqi Women Patients with Celiac Disease. Ibn AL-Haitham Journal for Pure and Applied Science, (2017); 27(1): 288-296.
- López-Casado MA, Lorite P, Palomeque T, Torres MI. Potential role of the IL-33/ST2 axis in celiac disease. Cellular & molecular immunology, (2017); 14(3): 285-292.
- da Silva EA, da Silva NM, Rodrigues RR, Adad SJ, de Lima PS, et al. Arginase-1 and Treg profile appear to modulate inflammatory process in patients with chronic gastritis: IL-33 may be the alarm cytokine in H. pylori-positive patients. Mediators of Inflammation, (2019); 2019 (1): 25336781.
- Li NF, Wang X, Deng H, Zhang K, Zhang X, et al. Autophagy-related 5 gene rs510432 polymorphism is associated with hepatocellular carcinoma in patients with chronic hepatitis B virus infection. Immunological Investigations, (2019); 48(4): 378-391.
- Shao Y, Chen F, Chen Y, Zhang W, Lin Y, et al. Association between genetic polymorphisms in the autophagy-related 5 gene promoter and the risk of sepsis. Scientific reports, (2017); 7(1): 9399.
![]()