

Full Length Research Article
The Relationship of CXCL12 with Sperm Agglutination and Anti-Sperm Antibody Among Infertile Men
Fahad Dhamin Oleiwi1*, Mousa J. Mohammed2, Chatin I. Ali3
Adv. life sci., vol. 11, no. 4, pp. 785-790, November 2024
*– Corresponding Author: Fahad Dhamin Oleiwi (fahad.d.oleiwi.bio1210@st.tu.edu.iq)
Authors' Affiliations
2. Biology Department, College of Science, Tikrit University- Saladdin Governorate – Iraq
3. College Of Dentistry, Tikrit University- Saladdin Governorate – Iraq
[Date Received: 12/08/2024; Date Revised: 13/03/2024; Date Published: 15/10/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: It is known that structural elements like the ‘blood-testis barrier’ (BTB) and local & systemic tolerance mechanisms help to maintain testicular homeostasis, which shields germ cells and mature sperms from immune attack. Any damage to this barrier could result in immune attack and may cause infertility.
Methods: The most important goal of this study was to find the vital connection between male infertility and immunological factors (CXCL12 and anti-sperm antibody). During the months of October 2021 and July 2022, a total of 144 samples were taken from patients who sought to have infertility tested. Semen and blood samples were taken from the subjects to assess seminal plasma CXCL12 levels and the prevalence of anti-sperm antibody (ASA) in their serum. Alternatively, research on sperm function parameters, sperm agglutination risk, and its relationship to ASA and CXCL12.
Result: statistically there was no ‘significant’ difference in CXCL12 levels across study groups in this investigation. The prevalence of sperm agglutination was 23.61% across all patients under study, the majority of whom had asthenozoospermia. In contrast, 60% of the samples from ASA-positive patients were agglutinated. The results revealed a relatively weak positive link that may call for additional research even if there was no significant statistical correlation in the relationship between CXCL12 and sperm functions and ASA.
Conclusion: The findings of this study suggest that ASA affects seminal fluid parameters, which in turn affects male fertility, and that a weak, non-significant association between CXCL12 and sperm function could impair sperm function by reducing sperm motility. Sperm agglutination could be a sign of immunological infertility. ASA can impact male fertility in a number of ways. Others had to do with sperm agglutination.
Keywords: CXCL12; Anti-sperm antibody; ASA; Sperm agglutination; Sperm function
Introduction![]()
According to the World Health Organization (WHO), infertility is a disorder condition of the human male or female reproductive system that is characterized by the inability of the couple to conceive after 12 months or more of frequent, unprotected sexual activity. Male infertility refers to any condition that makes it more difficult to conceive and can be brought on by problems with sperm function or obstructions that inhibit ejaculation. Its incidence and progression are influenced by a variety of circumstances, including disease, trauma, chronic morbidity, and lifestyle decisions [1, 2].
The homeostatic ‘CXC chemokine stromal cell-derived factor-1’ (SDF-1), commonly known as CXCL12, has seven distinct isoforms. It controls hematopoietic cell ‘trafficking’ and the secondary lymphoid tissues architecture by being secreted mainly in a variety of different tissues by stromal cells, fibroblasts, and epithelial cells [3]. According to Mao et al., CXCL12 has a particular receptor known as the ‘C-X-C motif chemokine receptor 4’ (CXCR4)[4]. The second receptor for ‘CXCL12’ is the ‘C-X-C motif chemokine receptor 7’ (CXCR7), according to numerous studies. Extracellular CXCL12 activates several signal transduction pathways by binding to CXCR4 or CXCR7 on the cell surface to control cell activity [5].
Since 1954, when Philip R. Umke in the Netherlands and ‘Leo Wilson’ in the USA first discovered the presence of ASAs in the blood and sperm of infertile men, researchers have concentrated on these compounds [6]. Due to the identification of ASAs as a direct cause of infertility and the finding that infertile men have greater levels and incidence of ASAs than healthy men [7], a type of immunological form of human infertility has gained more attention in recent decades. ASAs are recognized immunological indicators for the evaluation of compromised male fertility since there is currently a belief that a pathologically elevated auto-reactive immune response to the antigens of the reproductive system might cause infertility [8]. 10% of infertile men have ASAs, and 4.5-15% of populations experience the immunological manifestation of infertility [9].
It is well recognized that testicular inflammation (orchitis), which can have both infectious and non-infectious causes [10], can lead to autoimmunity to sperm. Non-infectious orchitis frequently develops after traumas (20–30% of instances involve vasectomy, invasive operations, and biopsy, among others). In general, any injury to the testis is linked to the development of immunological infertility. The “danger hypothesis” of P. Matzinger’s Viewpoint, which is based on the notion that the immune system is more concerned with harmful organisms than with foreign ones, describes a model of immunity based on this theory [11].
Additionally, for a very long time, the anatomical blood-testis barrier was mistakenly credited as the cause of local injury, which was therefore seen as a factor damaging the testis's "immune privilege." In actual fact, this opinion is vanishing because of the "barrier" is now thought to be an informational type of barrier created by local paracrine/juxtacrine action of anti-inflammatory cytokines that are produced in the testis and down-regulation of autoimmunity responses by androgens rather than an anatomical obstacle for antibodies. The reproductive system may suffer major repercussions as a result of local inflammation, which also disrupts relative immunological tolerance [12].
Immunoglobulins called anti-sperm antibodies interact with spermatozoa AGs to impair the role of the male gamete, which affects the fertility state of the man [13]. It is now unable to say with certainty that the etiology of ASA has been thoroughly defined, despite the possibility of its significant relevance. It is widely acknowledged that ASA can manifest as a result of weakening, injury, or disruption to the BTB, as well as developmental anomalies in BTB formation [14]. In fact, the research of ASA-mediated male infertility has drawn attention to numerous diseases that are, at least in part, connected with the integrity of the BTB and can potentially be potential risk factors for ASA development, as we will describe in more detail. Furthermore, although it hasn’t been well studied, it’s also likely that ASA is made at the epididymal level [15].
In actuality, sperm maturation and storage are made possible by the ‘blood-epididymal barrier’ (BEB), which guards the male reproductive epididymis and controls the luminal-microenvironment. The damage of BEB function or the loss of its integrity, which is thought to be less durable than BTB, can similarly make sperm cells more susceptible to the immune system, leading to the formation of ASA [15]. However, the formation of naturally arising ASA appears to have an idiopathic origin in the great majority of instances [16].
Male fertility may be impacted by antisperm antibodies in a variety of ways. Acrosome reaction, sperm-egg interaction, sperm motility reduction, sperm agglutination, impaired sperm ability to penetrate cervical mucus, or inhibition of sperm capacitation are the effects that have received the most attention [17].
Methods![]()
A prospective study was conducted between October 2021 and July 2022. It involved gathering 144 subjects who accepted to participate in this research by signing the informed consent of this study which was approved ethically from tikrit university authorities. The serum and seminal plasma (SP) were collected for testing CXCL12 and anti-sperm antibodies, respectively. The SP was separated by centrifuging the whole seminal fluid at 3000 rotations per minute (Rpm) for fifteen minutes after liquefaction and seminal fluid analysis for all seminal fluid samples, and the SP were stored at -36°C until analysis.
Seminal fluid analysis: Immediately following the liquefaction of the semen sample, the concentration and motility of sperms were evaluated together with the other sperm function parameters to limit the detrimental effects of sperm dehydration, pH fluctuations and the temperature variations on sperm motility and viability. In this study five fields present away from the edge of the cover-slip, the quantity of sperms and the motility of spermatozoa were counted and recorded automatically. The number of progressive, non-progressive, and immotile spermatozoa on each slide was counted, and the sperms were divided into progressive, non-progressive, and immotile categories in accordance with (WHO, 2021) standards [18].
Evaluation of ASA & CXCL12: Serum ASA and seminal plasma CXCL12 were prepared and measured by using enzyme linked immune-sorbent assay (ELISA). The ELISA of CXCL-12 and ASA depends on the competitive interaction between CXCL-12, ASA and the enzyme conjugate for a limited amount of immobilized monoclonal anti-CXCL-12 and anti-ASA antibodies respectively. After incubation of specimen and enzyme conjugate in the micro-titer plate wells, unbound conjugate was removed by washing out. At the point when substrate solution was included as step2, a blue color develops changing to yellow after stopping the reaction [19]. The strength of the color was correlated to the concentration of CXCL-12 and ASA in the sample. The absorbance of calibrators and sample were detected by utilizing ELISA micro-titer plate readers (BIOBASE Reader).
Results![]()
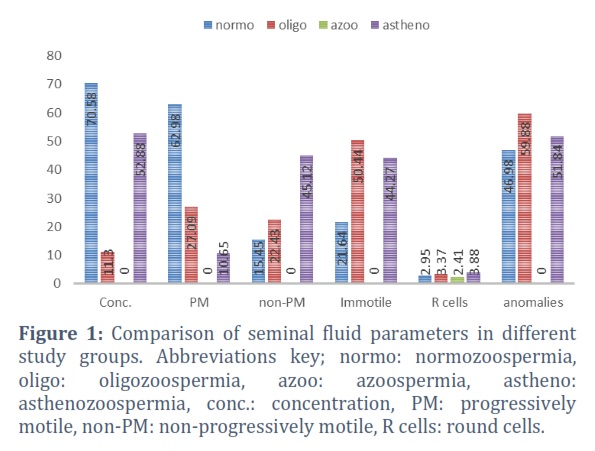
The analysis of seminal fluid parameters, including sperm concentration, motility grades, round cells, and anomaly of the spermatozoa revealed that the mean and standard deviation (SD) of spermatozoa concentration (million/ml) in normozoospermic men was (70.58 ± 20.96), which was significantly (p<0.05) higher than those of the azoospermic, oligozoospermic men, and asthenozoospermic men as shown in figure (1) and table (1).
Progressive sperm motility for men with normozoospermia was (62.98 ± 8.96), for men with oligozoospermia was (27.09 ± 14.99), for men with asthenozoospermia was (10.65±6.04), and zero for patients with azoospermia. These differences between the control and study groups are highly significant (p< 0.01), as shown in figure (1) and table (1). Non-progressive motile sperms% were (15.45±4.75) for normozoospermic men, (22.43±9.03) for oligozoospermic men, (45.12±12.99) for asthenozoospermic men, and (0.0±0.0) for azoospermia. According to figure (1) and table (1). the statistical analysis of the data of the patients revealed a highly significant difference between the groups, and asthenozoospermia patients having the highest mean.
For normozoospermic men the immotile sperms were (21.64 ± 6.82), for oligozoospermic were (50.44 ± 18.55), for asthenozoospermic were (44.27 ± 15.75), and obviously zero for azoospermia, according to the results the highest mean and SD was observed in oligozoospermia patients, as shown in figure (1) and table (1).
Round cells (cell/HPF) were (2.95 ± 1.41) for normozoospermic men, (2.41 ± 1.75) for azoospermic men, (3.37 ± 2.7) for oligozoospermic men, and (3.88 ± 1.24) for asthenozoospermic men, and there was no statically significant difference among them in this parameter. This is depicted in figure (1) and table (1).
Spermatozoa anomalies which was the last function parameter regarding this study was zero for azoospermia since no spermatozoa was counted and the mean of normozoospermia was (46.98 ± 8.01), for oligozoospermic men were (59.88 ± 9.63) and for asthenozoospermia were (51.84 ± 6.13), the results showed that there were highly significant (p<0.01) differences among them as shown in figure (1) and table (1).
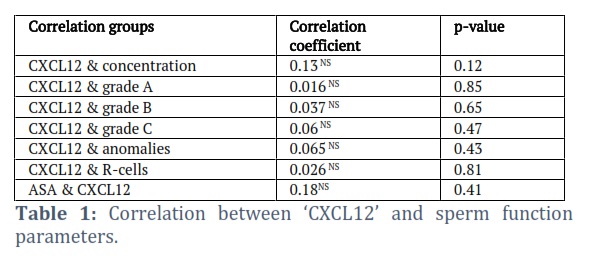
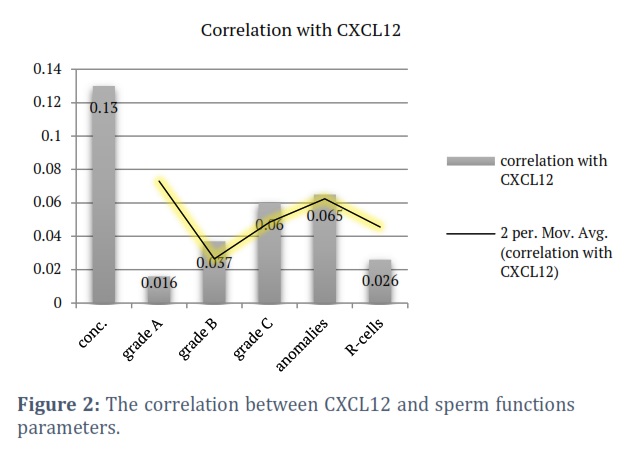
The total number of specimens used in this investigation was 144, and the 34 specimens with sperm agglutination ranged in grade from I to III. The overall percentage of agglutinated samples was 23.61%, with asthenozoospermia accounting for the vast majority of these cases and azoospermia definitely being exempt. Similarly, it could not be seen in oligozoospermia, which may be related to the low likelihood of sperm attachment due to the availability of free space in the seminal fluid. Conversely, 60% of positive ASA individuals had agglutinated samples, which would suggest that ASA was present in the sample. There were no discernible variations in the mean and SD of CXCL12 between normozoospermic males (168.24 ± 45.58), azoospermia men (149.23±22.0), oligozoospermic men (161.37±26.4), and asthenozoospermic men (165.92±40.17). Although there was no statistically significant difference, it is clear that the control group had the highest level, and the azoospermia patients had the lowest level. as demonstrated in picture (2) and table (1). The mean and SD of ASA in this prospective study were (48.64±13.21) in normozoospermic men, (59.69±12.89) in azoospermic men, (45.14±14.22) in oligozoospermic men, and (49.7±15.29) in asthenozoospermic men. As shown in table (2), the findings revealed a statistically significant difference between the study groups (p<0.05). Twenty three males with ASA levels more than 60 U/ml in serum participated in this investigation; they were divided among the four study groups in the following proportions: five had normozoospermia, or 10.63%, eleven had asthenozoospermia, or 20.75%, three had oligozoospermia, or 9.37%, and four had azoospermia, or 33.33%. The overall percentage of men who tested positive for ASA was 15.97%, with the lowest positive result being 60.03 U/ml and the highest being 92.56 U/ml. The correlation investigation between CXCL12 and spermatozoa function parameters showed that CXCL12 and other spermatozoa function parameters did not significantly correlate, which suggests that the association does exist but is very weak. The results, as shown in table (1) and figure (2), indicated that the largest positive association could be detected with spermatozoa concentration and the lowest with immotile sperms and abnormalities, respectively.
Figures & Tables

Since CXCL12 is an essential chemokine for the migration and colonization of primordial germ cells throughout the embryonic stage, it is vital for human fertility. And based on the study's findings, it is evident that normozoospermic men have the highest levels of CXCL12, while azoospermic men have the lowest levels. Low levels of CXCL12 may be the result of a genetic defect, which could lead to abnormal gonad and germ cell differentiation during the embryonic stage.
By raising sperm intracellular calcium, the CXCL12-CXCR4 signaling can cause sperm hyperactivation, most likely by controlling the activity of Catsper channels[18]. These occurrences appear to be related to spermatozoa chemotaxis, and CXCL12-CXCR4 signaling may be a crucial step in the fertilization of the ovum. The results of this study concurred with those from Wang et al., Hatef et al., Hakimi et al., and Politch et al., who for the first time found very high amounts of CXCL12 in the semen of fertile men. It follows that CXCL12 may play a significant part in the development and maintenance of male fertility [21-24].
As mentioned above, in this study, normozoospermic men had the highest level of functionally normal sperm parameters, while the functions decreased in other groups and disappeared in azoospermic men. These findings concurred with Calagna et al., [25] and were in agreement with WHO2021 standards [18]. The results of the sperm anomalies study supported Otasevic et al., in that oligozoospermic men had the highest level of anomalies and normozoospermic men had the lowest level [26]. According to Shibahara, who supports the study’s findings, ASA can influence male fertility through a variety of processes. Others had to do with sperm agglutination. The conclusions of this study concur with those of the WHO Laboratory Manual for the Examination and Processing of Human Semen, published in 2021[27, 18].
Silva et al., found that the prevalence of ASA-related infertility among instances of male infertility is rather low (2.6-6.6%). The results of this study conflict with those of a previous study that found that 15.97% of infertile males participated in it [28]. According to Cui et al., and AS, V. et al., two studies that concurred with this one, the presence of ASA dramatically decreased sperm concentration and motility [29, 6]. A high percentage of ASA was found in azoospermia in this study, indicating the presence of sperm in the testes that are prevented from ejaculating. The research matched Lee et al., [30].
The findings of this study may lead us to the conclusion that immunological infertility may be indicated by the presence of sperm agglutination in seminal fluid, and that ASA levels in the patient's serum or seminal plasma should be checked. The presence of ASA in azoospermia may lead us to assume that the condition is an obstructive azoospermia, which can be treated with medicine or in vitro fertilization. There was a significant difference between the groups in ASA, which was at its greatest level in Azoospermia and Asthenozoospermia. In this investigation, there was no discernible relationship between sperm function metrics and ASA and CXCL12.
Acknowledgements
First and foremost, we would like to express our sincere gratitude to Almighty Allah for providing us with the will and strength to complete this study. We are really appreciative of anyone who has assisted or provided guidance. We would especially like to thank Mr. Baker Awad and Mr. Khalil Ibrahim for their assistance in the lab. We are grateful to the study's volunteers for their assistance.
Author Contributions
The authors confirm contribution to the paper as follows: study conception and design: Fahad Dhamin Oleiwi, Mousa J. Mohammed, Chatin I. Ali; data collection: Fahad Dhamin Oleiwi; analysis and interpretation of results: Fahad Dhamin Oleiwi, Mousa J. Mohammed, Chatin I. Ali; draft manuscript preparation: Fahad Dhamin Oleiwi, Mousa J. Mohammed, Chatin I. Ali. All authors reviewed the results and approved the final version of the manuscript.
The author declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- Harrison JE, Weber S, Jakob R, Chute CG. ICD-11: an international classification of diseases for the twenty-first century. BMC medical informatics and decision making, (2021); 21, 1-10.
- Agarwal A, Baskaran S, Parekh N, Cho CL, Henkel R, et al. Male infertility. The Lancet, (2021); 397(10271): 319-333.
- Luther SA, Bidgol A, Hargreaves DC, Schmidt A, Xu Y, et al. Differing activities of homeostatic chemokines CCL19, CCL21, and CXCL12 in lymphocyte and dendritic cell recruitment and lymphoid neogenesis. The Journal of Immunology, (2002); 169(1): 424-433.
- Mao TL, Fan KF, Liu C L. Targeting the CXCR4/CXCL12 axis in treating epithelial ovarian cancer. Gene therapy, (2017); 24(10): 621-629.
- Huynh C, Dingemanse J, Zu Schwabedissen HEM, Sidharta PN. Relevance of the CXCR4/CXCR7-CXCL12 axis and its effect in pathophysiological conditions. Pharmacological Research, (2020); 161: 105092.
- AS V, Dhama K, Chakraborty S, Abdul Samad, H, K Latheef S, et al. Role of antisperm antibodies in infertility, pregnancy, and potential for contraceptive and antifertility vaccine designs: Research progress and pioneering vision. Vaccines, (2019); 7(3): 116.
- Lu SM, Li X, Wang S L, Yang X L, Xu YZ, et al. Success rates of in vitro fertilization versus intracytoplasmic sperm injection in men with serum anti-sperm antibodies: a consecutive cohort study. Asian Journal of Andrology, (2019); 21(5): 473.
- Parida, R. Human MOSPD2: A bacterial Lmb mimicked auto-antigen is involved in immune infertility. Journal of translational autoimmunity, (2019); 1, 100002.
- Westerman, R. Biomarkers for demographic research: Sperm counts and other male infertility biomarkers. Biodemography and Social Biology, (2020); 65(1): 73-87.
- Piroozmand A, Nasab SDM, Erami M, Hashemi SMA, Khodabakhsh E, et al. Distribution of human papillomavirus and antisperm antibody in semen and its association with semen parameters among infertile men. Journal of Reproduction & Infertility, (2020); 21(3): 183.
- Matzinger P. The danger model: a renewed sense of self. science, (2002); 296(5566): 301-305.
- Archana SS, Selvaraju S, Binsila BK, Arangasamy A, Krawetz SA. Immune regulatory molecules as modifiers of semen and fertility: A review. Molecular Reproduction and Development, (2019); 86(11): 1485-1504.
- Azizi G, Namaki S, Mirshafiey A, Hamid KM. HLA antigens and anti-sperm antibody production in Iranian vasectomized men. Journal of biomedical research, (2015); 29(1): 87.
- Xu F, Ye L, Hu Y, Cai C, Wang Z, et al. A novel protein biochip screening serum anti-sperm antibody expression and natural pregnancy rate in a follow-up study in Chinese infertility. Bioscience Reports, (2020); 40(2): BSR20191769.
- Lotti F, Baldi E, Corona G, Lombardo F, Maseroli E, et al. Epididymal more than testicular abnormalities are associated with the occurrence of antisperm antibodies as evaluated by the MAR test. Human Reproduction, (2018); 33(8): 1417-1429.
- Barbonetti A, Castellini C, D’Andrea S, Cordeschi G, Santucci R, et al. Prevalence of anti-sperm antibodies and relationship of degree of sperm auto-immunization to semen parameters and post-coital test outcome: a retrospective analysis of over 10 000 men. Human Reproduction, (2019); 34(5): 834-841.
- Al-Daghistani HI. Staphylococcusaureus protein A as a means of assessing sperm penetrability in cervical mucus in vitro. Clinical and Experimental Reproductive Medicine, (2020); 47(3): 186.
- Björndahl L, Brown JK. The sixth edition of the WHO Laboratory Manual for the Examination and Processing of Human Semen: ensuring quality and standardization in basic examination of human ejaculates. Fertility and sterility, (2022); 117(2), 246-251.
- Alhajj M, Zubair M, Farhana A. Enzyme linked immunosorbent assay [Internet]. U.S. National Library of Medicine; 2023 [cited 2023 Apl 24]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555922/
- Sugiyama H, Chandler DE. Sperm guidance to the egg finds calcium at the helm. Protoplasma, (2014); 251: 461-475.
- Wang C, Huang J, Ding L, Huang R, Dai L, et al. Effects of CXCL12/CXCR4/CXCR7 axis on human sperm motility and chemotaxis. bioRxiv, (2019); 831065.
- Hatef B, Taromchi A, Nejatbakhsh R, Farrokhi A, Shokri S. Supplementation of freezing media with stromal cell-derived factor-1α preserves human sperm from cryodamage. Cryobiology, (2017); 79: 37-42.
- Hakimi H, Zainodini N, Khorramdelazad H, Arababadi MK, Hassanshahi G. Seminal levels of pro-inflammatory (CXCL1, CXCL9, CXCL10) and homeostatic (CXCL12) chemokines in men with asymptomatic Chlamydia trachomatis infection. Jundishapur journal of microbiology, (2014); 7(12): e11152
- Politch JA, Tucker L, Bowman FP, Anderson DJ. Concentrations and significance of cytokines and other immunologic factors in semen of healthy fertile men. Human Reproduction, (2007); 22(11): 2928-2935.
- Calagna G, Catinella V, Polito S, Schiattarella A, De Franciscis P, et al. Vitamin D and Male Reproduction: Updated Evidence Based on Literature Review. Nutrients, (2022); 14(16): 3278.
- Otasevic V, Kalezic A, Macanovic B, Jankovic A, Stancic A, et al. Evaluation of the antioxidative enzymes in the seminal plasma of infertile men: Contribution to classic semen quality analysis. Systems biology in reproductive medicine, (2019); 65(5): 343-349.
- Shibahara H, Chen Y, Honda H, Wakimoto Y, Fukui A, et al. Sex difference in anti‐sperm antibodies. Reproductive Medicine and Biology, (2022); 21(1): e12477.
- Silva AF, Ramalho-Santos J, Amaral S. The impact of antisperm antibodies on human male reproductive function: An update. Reproduction, (2021), 162(4): R55-R71.
- Cui D, Han G, Shang Y, Liu C, Xia L, et al. Antisperm antibodies in infertile men and their effect on semen parameters: a systematic review and meta-analysis. Clinica Chimica Acta, (2015); 444: 29-36.
- Lee R, Goldstein M, Ullery BW, Ehrlich J, Soares M, et al. Value of serum antisperm antibodies in diagnosing obstructive azoospermia. The Journal of urology, (2009); 181(1): 264-269.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0![]()