

Full Length Research Article
Soluble endoglin as a diagnostic glycoprotein in preeclampsia
Shaima Sh. Al-Kilan, Ekhlas Abdallah Hassan*
Adv. life sci., vol. 11, no. 3, pp. 593-599, August 2024
*– Corresponding Author: Muhammad Mohsin Zaman (mohsinzaman3@gmail.com)
Authors' Affiliations
[Date Received: 18/06/2023; Date Revised: 31/07/2023; Date Published: 10/07/2024]
Editorial Expression of Concern:
18 May 2025: Following publication of this paper, the internal audit (consequent to concerns on quality raised by Web of Science) notified Advancements in Life Sciences about problems in use of English language. By this Editorial Expression of Concern, we alert the scientific community as we address the errors.
Editorial Note:
31 May 2025: You are viewing the latest version of this article having minor corrections related to the use of English language. Expression of concern is hereby revoked.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Angiogenic factor imbalance, such as that caused by soluble endoglin (sEng), is a feature of preeclampsia. However, the connection between sEng and clinical and laboratory indicators, and the severity of preeclampsia is not entirely understood.
Methods: Ninety subjects were incorporated in this study, 30 were healthy pregnant with mean age (35.6) years. (32) mild Preeclampsia case with mean age (32.65) years preeclampsia, and (30) sever PE with mean age (32.65) and all women were more than 24 weeks of pregnancy. mean blood pressure and proteinuria levels were used as indicators of the severity of the disease. ELISA was used to measure the levels of sEng in the serum. Serum lipid profile was measured by enzymatic methods. The qualitative dip-stick technique (CYBOWTM DFI Co Ltd, Republic of Korea) was used to assess the amount of urine protein.
Results : A substantial difference in serum sEng concentration between the PE group and the healthy subjects (p 0.001) could be seen. Serum sEng concentrations differed significantly between patients with moderate and severe PE. Additionally, there were strong positive relationships between the serum sEng concentration and the SBP and proteinuria. serum sEng levels, biochemical indicators, and other factors, however, did not significantly correlate. The diagnostic accuracy (86.2) in distinguishing mild PE from the healthy patient group was good thanks to the excellent area under the curve (AUC = 0.827, p < 0.0001).
Conclusion: Levels of sEng in sera of PE patients were elevated. sEng was significantly elevated in PE patients.
Keywords: Soluble Endoglin; Preeclampsia; Proteinuria; Blood Pressure
Introduction![]()
Pre-eclampsia (PE) is a pregnancy-related multisystem disorder with no recognized cause. The root cause of PE is currently being investigated. It is believed to take place in two phases, though. The decidua's fetal trophoblastic invasion impairment and the placenta's localized hypoxia are included in the first stage [1,2]. The second stage includes the release of placental blood-associated molecules into the mother’s circulation as well as abnormal synthesis of pro-inflammatory, antiangiogenic, and angiogenic factors [3, 4]. Around week 20 of pregnancy, PE frequently shows clinical signs or later in the pregnancy, with the condition regressing after birth. Typical symptoms include proteinuria and elevated blood pressure [5]. Early-onset PE (which manifests before 34 weeks of gestation) and late-onset PE are the two main kinds of PE (which occurs beyond 34 weeks of gestation) [6,7]. Although the precise cause of this pregnancy-related disease is unknown, mounting evidence points to an imbalance between placental pro- and anti-angiogenic hormones that damages maternal vascular endothelium and causes preeclampsia, which then manifests clinically. Serum tests for pro- and anti-angiogenic factors, particularly placental growth factor, soluble vascular endothelial growth factor receptor-1, and soluble fms-like tyrosine kinase-1, have been used to diagnose this disorder, gauge its severity, and assess its therapeutic potential [8-14]. CD105, sometimes referred to as Eng (endoglin), is a transmembrane homodimeric glycoprotein that is extensively produced on the cellular membrane of endothelium. [15]. sEng (soluble Eng), on the other hand, which is produced when Eng is shed from endothelial cell surfaces and enters. The maternal circulation is responsible for the antiangiogenic effects seen in preeclampsia. It does this by adhering to circulating TGF-1 and preventing it from sending signals to endothelial cells (specifically, the endothelium’s usual proangiogenic and vasodilator functions) [16]. These results suggest that sEng may play a role in the preeclampsia's etiology and the disruption of the angiogenesis pathway may have a significant influence on the emergence of the condition's clinical and laboratory symptoms as well as its outcomes. The link between blood clinical and test results, as well as sEng levels clinical and test results, as well as sEng levels in preeclampsia patients is poorly understood, despite the wealth of studies examining the roles of sFlt-1 and PlGF in the condition. This study examined whether blood sEng levels in preeclampsia patients might predict severe sickness and poor maternal outcomes.
Methods![]()
PE patients and Healthy pregnant groups
The Baquba Teaching Hospital's Obstetrics and Gynecology Department conducted this cross-sectional, case-control study from Sep. 2022 to Dec 2023. The Diyala Sciences College's Ethical Committee granted its permission for this study's ethical conduct. The research included 22 third-trimester pregnant women with severe PE and 38 with moderate PE at admission (MPE group) (SPE group). 30 healthy and expecting.
- Proteinuria was < 2+ on urine dipstick on at least two random specimens collected more than 4 hours apart after the 24th week of pregnancy, and MPE was SBP 140 mmHg or DBP 90 mmHg validated by 6 or more hours apart.
- SPE was identified by having SBP of at least 160 mmHg, DBP of at least 110 mmHg, proteinuria > 2+ on a urine dipstick, as well as headache, visual disturbances, upper abdominal pain, and oliguria. The SPE group's whole female population experienced both proteinuria and hypertension.
- Healthy pregnant : Normotensive pregnant women with gestational ages of more than 24 weeks, no chronic medical conditions, and no signs of labor. They had healthy blood pressure and were not hypertensive during pregnancy. Patients having a history of diabetes, kidney illness, hypertension, other cardiovascular issues, or infectious infections with symptoms were not allowed to participate.
Criteria for inclusion
Absence of labor contractions, an early membrane rupture, or clinical chorioamnionitis were the criteria for the PE group. None of the patients included had any of the following conditions, which were ruled out through regular consultations, clinical examinations, and laboratory tests: underlying diabetes, renal illnesses, chronic hypertension, or symptomatic infectious diseases. Before being enrolled in the trial, for a minimum of seven days, the pregnant women did not get corticosteroids.
Sample collection
Blood samples were taken from the patients' antecubital veins while they were lying supine after a minimum of eight hours of fasting and one hour of rest. The serum was then collected and stored at -20 C until use; whereas the urine that was still in the sterile container was examined with a Dipstick.
Urine sample : First morning urine sample was taken in a clean container free from any detergent. A mid-stream sample was taken, and it was put in a sterile container. The sample was then moved to an all-purpose container, and the pee still present in the sterile container was analyzed using a Dipstick. The qualitative dip-stick technique was used to assess the protein content of urine.
Anthropometric Measurements
Age, weight, and height were established using anthropometric measurements. Calculating one's body mass index involves using the standard formula of weight divided by height squared (BMI).
Measurements of blood pressure
Using a stethoscope, sphygmomanometer, which consists of a blood pressure cuff and a mercury column pressure gauge, and auscultation, which involves listening to sounds, blood pressure was first measured indirectly in 1902 by Russian physician N.S. Korotkoff. Systolic and diastolic blood pressure were both measured in millimeters of mercury, and for each individual, the average of the previous two readings was taken.
Urine analysis
A mid-stream sample was taken, and it was put in a sterile container. The sample was then transferred to a general-purpose container, and the pee still present in the sterile container was analyzed using a Dipstick. The qualitative dip-stick technique was used to assess the amount of urine protein (CYBOWTM DFI Co Ltd, Republic of Korea). It was determined in accordance with the manufacturer's description. The test's underlying principle is the protein "error of indicators." The presence of protein causes indicator dyes to release H+ ions, which cause them to turn green from yellow to blue green whenever a buffer keeps the pH stable. A visual inspection is an assay. A new strip was briefly dipped into urine that had been gathered early in the morning and stored in clean, dry plastic containers. In less than two seconds, the Up to the test region, the strip was inserted. To eliminate extra urine, the strip's edge was drawn around the brim of the vessel, making sure the test area did not contact it. Since too much pee on the strip might produce chemical interactions between neighboring pads that would lead to inaccurate findings, to get rid of any remaining pee, the strip was turned over and tapped against a piece of absorbent paper. In well-lit situations, both the test result that was displayed on the strip that was held horizontally and the color scheme that was included on the bottle label were contrasted.
Study of groups in clinical laboratories
The concentrations of sEng were measured using an ELISA plate reader (ca Inc., San Diego, CA, USA). An automated enzymatic technique was used to evaluate the serum lipid profile testing.
Statistical analysis
Using SPSS, the statistical analysis was completed (version 25). For numerical variables having normally distributed data, the data were converted into the average and the variation from the mean, respectively, and for categorical variables, into frequency/percentage. While a t-test performed independently, and an ANOVA test were employed to see whether there was a significant difference between the typically numerical variables. P 0.05 was used as the significant level The Pearson correlation and t-test were used to calculate the correlation's significance for the relationship between the two quantitative variables. Using the receiver operating characteristic (ROC) curve approach, it was possible to evaluate the utility of sEng as a diagnostic marker or disease-screening tool. Additionally, it was possible to determine the value range of the cut-off of the serum sEng concentration that has the maximum specificity and sensitivity for diagnostics.
Results![]()
PE patient groups and healthy persons' anthropometric and biochemical features
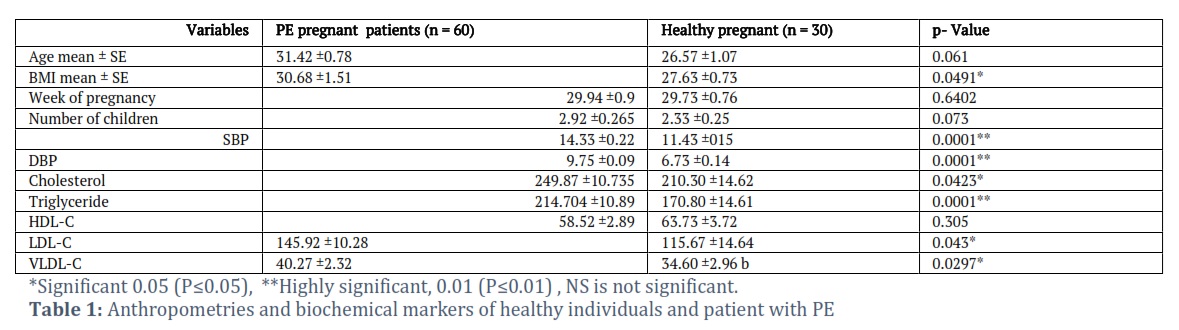
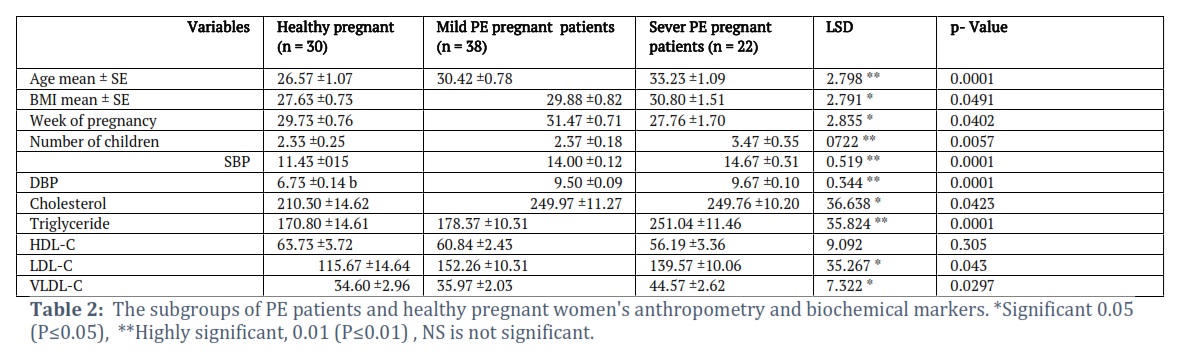
The mean ages of the normal participant group (43.6 4.7) and the PE patients (43.5 10.7) are shown in Table 1 with p 0.05, respectively. Between the healthy subject group's (29.2 3.7 kg/m2) and PE patients' (28.7 3.76 kg/m2) mean BMIs, there was no significant difference (p > 0.05). The findings from the subgroups, which included 30 patients with newly diagnosed PE and 30 individuals with continued diabetes, are given in table 2.
A healthy pregnant woman's serum sEng in PE groups
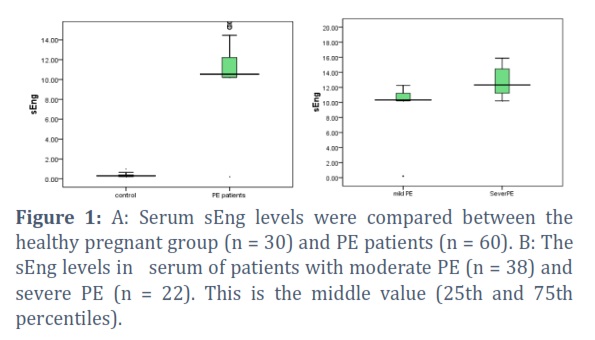
The level of serum sEng was significantly higher in pregnant patients with PE(58.31) ng/ml compared to the healthy pregnant group (82.53±13.16 ng/ml) (p < 0.05), and it was also significantly higher in severe PE patients (51.26 ± 7.05) ng/ml compared to the moderate PE patients group (67.08±6.59] ng/ml). These findings are depicted in Figure 1 (A, B).
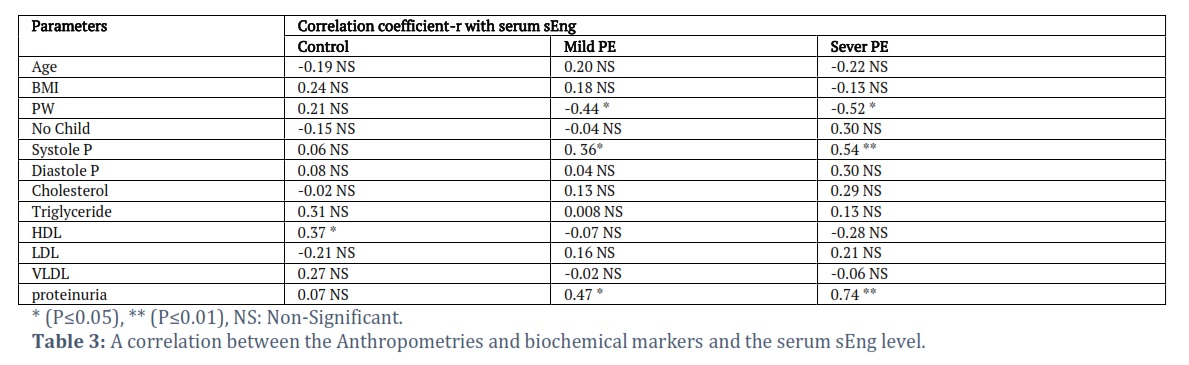
A correlation between the severity of the illness and the serum sEng level
As shown in Table 3, there was a significant positive association between the serum sEng concentration and proteinuria in the moderate PE group (R = 0.47, p< 0.05) as well as SBP (R = 0.36, p< 0.05). Additionally, In the group with severe PE, Serum sEng concentration correlated substantially with proteinuria (R = 0.74, p <0.001) and SBP (R = 0.54, p 0.001). A significant inverse association between the serum sEng levels and the weeks of pregnancy at the time of sampling, however, also exists. Serum sEng did not significantly correlate with any biochemical variable, including the lipid profile (p > 0.05).
ROC curve analysis test
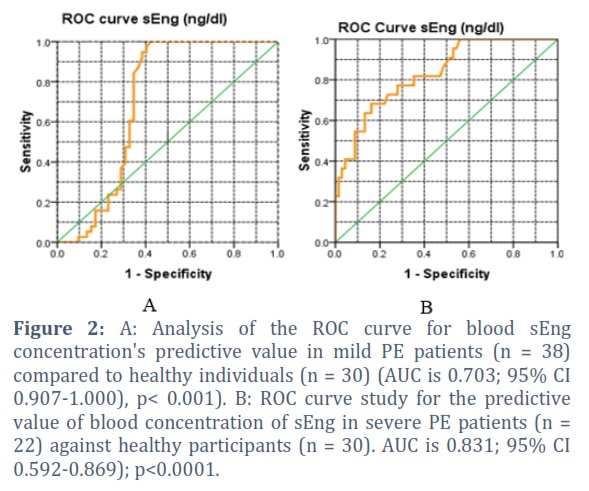
Utilizing ROC curve analysis (Table 4; Fig. 2(A)), it was determined how well the blood sEng concentration could discriminate mild PE patients from healthy pregnant women. Compared to the PE diagnostic test, the ROC curve showed significantly higher reliability (high sensitivity and high specificity). Accuracy in predicting proteinuria was maximized at an AUC of 0.70 (p = 0.001), as shown by the ROC curve for the diagnosis of mild PE patients (Table 4; Fig. 2(A)). Serum sEng concentration was evaluated using ROC curve analysis to see if it could distinguish severe PE patients from healthy pregnant women (Table 5; Fig. 2(B)). The ROC curve demonstrated higher diagnostic accuracy than the standard test for PE, which was significantly higher (high sensitivity and high specificity). a fair level of accuracy in predicting proteinuria was shown by the occurrence of a PE diagnosis, as indicated by the ROC curve AUC of 0.703 (p< 0.001).
Figures & Tables


This study evaluated sEng levels in women with mild and severe PE and healthy pregnant women. Angiogenic imbalance is thought to play a role in the pathophysiology of PE [17]. Eng, a pro-angiogenic drug, inhibits hypoxia endothelial cell death and regulates vascular tone via nitric oxide [18,19]. An anti-angiogenic protein called soluble Eng prevents TGF-b1 from attaching to its receptors and suppresses downstream signaling, which includes eNOS activation and vasodilation [20].
Preeclampsia patients have greater serum sEng levels than typical pregnant women. We also found that sEng levels rose with preeclampsia severity, suggesting that they accurately signify the deterioration of the systemic vascular endothelium. Worse preeclampsia symptoms were associated with higher blood sEng levels, including proteinuria exceeding 2g/day. Our findings support the idea that this particular antiangiogenic factor is altered in women with preeclampsia and that these biochemical abnormalities become more prominent as the condition progresses, especially when preterm. [21,22].
Additionally, we found that the serum sEng levels and the number of weeks pregnant had a substantial negative correlation. A significant inverse relationship between the blood sEng levels and gestational age at sampling has been shown by prior studies1[23,24].
Troisi et al. (2008) linked sEng to pregnancy-related elevated blood pressure [23]. In one PE animal model, sEng-encoding adenovirus induced hypertension, proteinuria, and endothelial dysfunction, which were exacerbated by sEng and sFlt1 coadministration and brought about the help syndrome and prenatal growth restriction [26]. Our experimental results are supported by the positive correlation between systolic blood pressure and PE sEng levels.
Since glomeruli separate the blood and urine compartments, angiogenesis is crucial to renal homeostasis. Genetic studies in mice show that VEGF and PlGF are crucial to renal development and vascular health [27]. sFlt-1 and sEng, anti-angiogenic factors, are linked to glomerular injury and proteinuria. Venkatesha et al. [26] discovered nephrotic-range proteinuria in sEng-treated rats and severe proteinuria in sFlt-1-treated rats. Masuyama et al. [28] found higher proteinuria in high-sEng patients.
Serum sEng has a high AUC of 0.95 and more than 90% sensitivity and specificity for PE diagnosis in normal pregnant women. Based on our findings, sEng is a serum marker with excellent accuracy in identifying PE. Its higher sensitivity and specificity in severe and early-onset PE patients makes it more accurate. De Vivo et al. [29] found that sEng may predict PE early with over 80% sensitivity and specificity in blood samples from 24–28 weeks of gestation. Lim et al.[30] found sEng’s PE prediction AUC to be 0.83. Baumann et al. [31] found an AUC of 0.62 for sEng in predicting late-onset PE in first trimester serum. Our ROC curve study shows that sEng is better at diagnosing PE in normal pregnant women than severe and early-onset cases.
Our study's strengths include a well-defined, standardized medical regimen for preeclampsia patients and the fact that all samples were taken early in PE, avoiding selection bias. Our study only included PE patients as the case group, and we lost individuals from early pregnancy before PE onset. Thus, longitudinal studies should evaluate sEng, a potential marker, in a larger sample size and follow patients from early pregnancy.
Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Ekhlas Abdallah Hassan: conceptualization, analysis, visualization, curation of data, study, writing, original draft.
Shaima Sh. Al-Kilan: Resources, Visualization, editing writing
The final paper was read and authorized by all writers.
![]() References
References
- Hung TH, Skepper JN, Charnock-Jones DS, Burton GJ. Hypoxia-reoxygenation: a potent inducer of apoptotic changes in the human placenta and possible etiological factor in preeclampsia. Circulation research, (2002);90(12):1274-81.
- Soleymanlou N, Jurisica I, Nevo O, Ietta F, Zhang X, et al. Molecular evidence of placental hypoxia in preeclampsia. The Journal of Clinical Endocrinology & Metabolism, (2005);90(7):4299-308.
- Turpin CA, Sakyi SA, Owiredu WK, Ephraim RK, Anto EO. Association between adverse pregnancy outcome and imbalance in angiogenic regulators and oxidative stress biomarkers in gestational hypertension and preeclampsia. BMC pregnancy and childbirth, (2015);15:1-0.
- Kim SY, Ryu HM, Yang JH, Kim MY, Han JY, et al. Increased sFlt-1 to PlGF ratio in women who subsequently develop preeclampsia. Journal of Korean medical science, (2007);22(5):873-7.
- Osungbade KO, Ige OK. Public Health Perspectives of Preeclampsia in Developing Countries: Implication for Health System Strengthening, Journal of Pregnancy. (2011); 2011(481095):6.
- Wilkinson J, Cole G. Preeclampsia knowledge among women in Utah. Hypertension in Pregnancy, (2018);37(1):18–24.
- Raymond D, Peterson E. A critical review of early-onset and late-onset preeclampsia. Obstetrical & Gynecological Survey, (2011);66(8):497–506.
- Levine RJ, Maynard SE, Qian C, Lim KH, England LJ, Yu KF, Schisterman EF, Thadhani R, Sachs BP, Epstein FH, Sibai BM, Sukhatme VP, Karumanchi SA. Circulating angiogenic factors and the risk of preeclampsia. New England Journal of Medicine, (2004);350:672–683.
- Levine RJ, Lam C, Qian C, Yu KF, Maynard SE, Sachs BP, Sibai BM, Epstein FH, Romero R, Thadhani R, Karumanchi SA; CPEP Study Group. Soluble endoglin and other circulating antiangiogenic factors in preeclampsia. New England Journal of Medicine, (2006); 355:992–1005.
- Leaños-Miranda A, Campos-Galicia I, Isordia-Salas I, Rivera-Leaños R, Romero-Arauz JF, et al. Changes in circulating concentrations of soluble fms-like tyrosine kinase-1 and placental growth factor measured by automated electrochemiluminescence immunoassays methods are predictors of preeclampsia. Journal of Hypertension, (2012);30:2173–2181.
- Rana S, Powe CE, Salahuddin S,V erlohren S, Perschel FH, Levine RJ, Lim KH, Wenger JB, Thadhani R, Karumanchi SA. Angiogenic factors and the risk of adverse outcomes in women with suspected preeclampsia. Circulation, (2012);125:911–919.
- Leaños-Miranda A, Campos-Galicia I, Ramírez-Valenzuela K, Chinolla-Arellano ZL, Isordia-Salas I. Circulating angiogenic factors and urinary prolactin as predictors of adverse outcomes in women with preeclampsia. Hypertension, (2013);61:1118–1125
- Leaños-Miranda A, Méndez-Aguilar F, Ramírez-Valenzuela KL, et al. Circulating angiogenic factors are related to the severity of gestational hypertension and preeclampsia, and their adverse outcomes. Medicine (Baltimore), (2017);96:e6005e.
- Zeisler H, Llurba E, Chantraine F, Vatish M, Staff AC, Sennström M, Olovsson M, Brennecke SP, Stepan H, Allegranza D, Dilba P. Predictive value of the sFlt-1: PlGF ratio in women with suspected preeclampsia. New England Journal of Medicine, (2016);374(1):13-22.
- Pece Barbara N, Wrana JL, Letarte M. Endoglin is an accessory protein that interacts with the signaling receptor complex of multiple members of the TGF-β superfamily. Journal of Biological Chemistry, (1999);274:584-94.
- Luft FC. Soluble endoglin (sEng) joins the soluble fms-like tyrosine kinase (sFlt) receptor as a pre-eclampsia molecule. Nephrology Dialysis Transplantation, (2006);21(11):3052-4.
- Robinson CJ, Johnson DD. Soluble endoglin as a second-trimester marker for preeclampsia. American journal of obstetrics and gynecology, (2007);197(2):174-e1.
- Li C, Issa R, Kumar P, Hampson IN, Lopez-Novoa JM, Bernabeu C, Kumar S. CD105 prevents apoptosis in hypoxic endothelial cells. Journal of cell science, (2003);116(13):2677-85.
- Jerkic M, Rivas‐Elena JV, Prieto M, Carrón R, Sanz‐Rodríguez F, Pérez‐Barriocanal F, Rodríguez‐Barbero A, Bernabéu C, López‐Novoa JM. Endoglin regulates nitric oxide‐dependent vasodilatation. The FASEB Journal, (2004);18(3):609-11.
- Venkatesha S, Toporsian M, Lam C, Hanai JI, Mammoto T, Kim YM, Bdolah Y, Lim KH, Yuan HT, Libermann TA, Stillman IE. Soluble endoglin contributes to the pathogenesis of preeclampsia. Nature medicine, (2006);12(6):642-9.
- Leaños-Miranda A, Campos-Galicia I, Ramírez-Valenzuela KL, Chinolla-Arellano ZL, Isordia-Salas I. Circulating angiogenic factors and urinary prolactin as predictors of adverse outcomes in women with preeclampsia. Hypertension, (2013);61(5):1118-25.
- Leaños-Miranda A, Méndez-Aguilar F, Ramírez-Valenzuela KL, Serrano-Rodríguez M, Berumen-Lechuga G, Molina-Pérez CJ, Isordia-Salas I, Campos-Galicia I. Circulating angiogenic factors are related to the severity of gestational hypertension and preeclampsia, and their adverse outcomes. Medicine, (2017);96(4).
- Perucci LO, Gomes KB, Freitas LG, Godoi LC, Alpoim PN, Pinheiro MB, Miranda AS, Teixeira AL, Dusse LM, Sousa LP. Soluble endoglin, transforming growth factor-Beta 1 and soluble tumor necrosis factor alpha receptors in different clinical manifestations of preeclampsia. PloS one, (2014);9(5):e97632.
- Rana S, Cerdeira AS, Wenger J, Salahuddin S, Lim KH, Ralston SJ, Thadhani RI, Karumanchi SA. Plasma concentrations of soluble endoglin versus standard evaluation in patients with suspected preeclampsia. PloS one, (2012);7(10):e48259.
- Troisi R, Braekke K, Harsem NK, Hyer M, Hoover RN, Staff AC. Blood pressure augmentation and maternal circulating concentrations of angiogenic factors at delivery in preeclamptic and uncomplicated pregnancies. American journal of obstetrics and gynecology, (2008);199(6):653-e1.
- Venkatesha S, Toporsian M, Lam C, Hanai JI, Mammoto T, Kim YM, Bdolah Y, Lim KH, Yuan HT, Libermann TA, Stillman IE. Soluble endoglin contributes to the pathogenesis of preeclampsia. Nature medicine, (2006);12(6):642-9..
- Tjwa M, Luttun A, Autiero M, Carmeliet P. VEGF and PlGF: two pleiotropic growth factors with distinct roles in development and homeostasis. Cell and tissue research, (2003);314:5-14.
- Masuyama H, Nakatsukasa H, Takamoto N, Hiramatsu Y. Correlation between soluble endoglin, vascular endothelial growth factor receptor-1, and adipocytokines in preeclampsia. The Journal of Clinical Endocrinology & Metabolism, (2007);92(7):2672-9.
- De Vivo A, Baviera G, Giordano D, Todarello G, Corrado F, D'anna R. Endoglin, PlGF and sFlt-1 as markers for predicting pre-eclampsia. Acta obstetricia et gynecologica Scandinavica, (2008);87(8):837-42.
- Lim JH, Kim SY, Park SY, Yang JH, Kim MY, Ryu HM. Effective prediction of preeclampsia by a combined ratio of angiogenesis-related factors. Obstetrics & Gynecology, (2008);111(6):1403-9.
- Baumann MU, Bersinger NA, Mohaupt MG, Raio L, Gerber S, Surbek DV. First-trimester serum levels of soluble endoglin and soluble fms-like tyrosine kinase-1 as first-trimester markers for late-onset preeclampsia. American journal of obstetrics and gynecology, (2008); 199(3):266-e1.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0