

Full Length Research Article
Evaluation of BACTEC™ FX and BacT/Alert™ Automated Blood Culture Systems for Detection of Clinically Relevant Bacterial and Yeast Species
Muhammad Absar*, Ibraheem Alshahrani, Fahd Nashmy, Mosa Salami, Ali Hadadi, Aous AlMarzooq, Alhussain AlAsiri, Abdulaziz AlRashidi, Mohammed AlFaifi
Adv. life sci., vol. 11, no. 3, pp. 648-654, August 2024
*– Corresponding Author: Muhammad Absar (absarmu@ngha.med.sa)
Authors' Affiliations
[Date Received: 30/11/2023; Date Revised: 30/04/2024; Date Published: 10/07/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Bloodstream infections (BSI) are a significant health concern, necessitating effective diagnostic tools. This study evaluates the performance of the BD Bactec FX system in comparison to the established BacT/Alert system, examining mean time till detection (TTD) across various blood culture bottles.
Methods: The study involves 148 blood culture bottles, inoculated with representative bacterial ATCC strains (n= 15) and 04 yeast isolates. Parallel testing is conducted by seeding 10–30 colony-forming units (CFU) in duplicate in both BD Bactec FX and BacT/Alert systems. TTD is assessed across aerobic, anaerobic, and pediatric bottles for diverse microbial species.
Results: All 148 bottles tested in parallel show positive signals in both systems. BD Bactec FX demonstrates significantly shorter TTD for adult-seeded cultures in aerobic and anaerobic bottles compared to BacT/Alert Similarly, pediatric bottles with BD Bactec FX exhibit a shorter TTD compared to BacT/Alert. The statistical significance of TTD, 95% confidence intervals (CI), and p-values is evident for Bactec FX aerobic, anaerobic, and pediatric bottles across tested organisms. Notable examples of faster TTD include; Bacteroides ovatus (16.6h by Bactec FX vs. 70.5h by Bact/Alert 3D), Stenotrophomonas maltophilia (33.7h vs. 72.5h), and Streptococcus pyogenes (8.1h vs. 11.9h).
Conclusions: In conclusion, the study’s findings demonstrate that BD Bactec FX surpasses BacT/Alert in prompt microbial detection, showcasing potential for early identification of bacteremia and fungemia. Faster TTD implies the potential to initiate timely antimicrobial treatment, thereby reducing patient morbidity and mortality. However, exceptions in certain microbial species highlight the need for comprehensive clinical validation to establish the broad applicability of these findings.
Keywords: Blood Culture System; Recovery Rate; Time to detection; Blood stream infection; BTA3D; Bactec FX
Introduction![]()
A bloodstream infection (BSI) is characterized by the presence of pathogenic microorganisms, such as bacteria or fungi, detected through one or more positive blood cultures, coupled with systemic signs of infection like pyrexia, chills, and hypotension [1]. Globally, BSIs carry a substantial morbidity burden, with an estimated crude mortality rate ranging from 15% to 30% [2]. Particularly, patients in intensive care units (ICUs) face elevated risks of complications and mortality associated with bloodstream infections (BSIs) [3, 4]. BSIs are the leading cause of infection-related deaths in the continent of North America and Europe, with 2 million cases and 250,000 deaths annually [4].
Several factors, including the rise in invasive procedures, immunosuppressant use, and the administration of broad-spectrum antibiotics at high dosages, have contributed to an observed increase in BSI rates in recent years. The severe consequences of severe sepsis, which claims over 6 million lives annually, underscore the urgency of prompt and accurate identification of the underlying causes of infection [5, 6]. Timely and appropriate antibiotic treatment can significantly improve patient outcomes and reduce mortality rates. However, identifying the causative agent through blood culture (BC) is crucial, especially in cases where septic complications arise, necessitating the enhancement of diagnostic yield from positive BCs [7-9]. Hospitalized patients, especially those in healthcare settings, face a heightened risk of acquiring healthcare-associated infections, including BSI [10].
The severe complications of BSIs, including septic shock or sepsis, underscore the need for high-throughput technology to facilitate the timely diagnosis of these infections. Any delay or oversight in detecting BSI can result in ineffective treatment, escalating into sepsis and a grim prognosis [11, 12].
Despite the advancements in diagnostic techniques, automated blood culture (BC) devices such as BactecTM FX (Bactec; Becton Dickinson, Sparks, MD, USA) and Bact/Alert®3D (BTA3D; bioMérieux, Marcy 'Étoile, France) remain the gold standard for BSI detection. This study focuses on the comparison between BactecTM FX and BTA3D, evaluating their performance in terms of proper growth, the ability to signal a positive BC bottle, and the time to detection (TTD) for clinically relevant bacterial and yeast species.
The choice between these systems significantly impacts the recovery of organisms, and both systems employ resin-containing media to enhance recovery. While the BTA3D instrument and its various generations have been in use since 1998, the Bact/Alert®VirtuoTM system (Virtuo) was introduced in 2014, offering several advantages over its predecessors, including enhanced temperature stability, automated loading and unloading of BC bottles, and an improved proprietary algorithm for decreased TTD (http://www.biomerieux-diagnostics.com/bact-alertr-virtuor-0).
Verification and validation are crucial aspects of assessing the performance of automated blood culture systems. Verification ensures that the test or instrument under study aligns with the manufacturer's claims, while validation involves ongoing monitoring of the instrument's performance through quality control, proficiency testing, calibration, etc. Verification of any automated blood culture system is considered one of the most challenging tasks for a clinical microbiology laboratory. The two well-known blood culture verification studies are seeded blood culture studies and parallel blood culture studies. The latter requires additional blood collection from each patient and is not feasible to conduct in many institutions. Conducting verification studies for automated blood culture systems, such as seeded blood culture studies and parallel blood culture studies, poses challenges. Parallel studies, which require additional blood collection from each patient, may not be feasible in many institutions due to logistical constraints and the low incidence of positive blood cultures. Seeded blood culture studies, while easier to conduct, and are not without challenges, including a limited number of isolated pathogens, which may skew the evaluation toward specific organisms. In light of these considerations, the present study aims to assess the Bactec FX instrument, a newly introduced system, in parallel with the BTA3D instrument, an established system, focusing on proper growth, the ability to signal a positive BC bottle, and the time to detection of clinically relevant bacterial and yeast species, utilizing seeded blood culture studies with standard ATCC strains [13, 14].
Methods![]()
Study design & setting
This study was conducted in the department of microbiology, at King Abdulaziz Hospital, National Guard, Saudi Arabia. This is a simulated, prospective, comparative study of test (BD Bactec FX) and reference (BTA3D) automated blood culture instruments by using seeded samples.
Types of blood culture bottles
The following frequently utilized commercial blood culture bottles were used in this study: BacT/Alert FA and BacT/Alert FN (bioMérieux, Durham, NC, USA), Plus aerobic/F and lytic/10 anaerobic/F (BD Diagnostics, Sparks, MD, USA), and each type of bottle utilized in the analyses from the same batch. Human blood was obtained from the hospital's blood bank laboratory and kept at 4°C for this experiment.
Organisms and Inoculum preparation
The following representative ATCC strains were utilized for verification studies (n=19); i) Anaerobes (n=4); Bacteroides fragilis (ATCC-25285), Bacteroides ovatus (ATCC-BAA-1296), Clostridium perfringens (ATCC-13124) and Clostridium septicum (ATCC-12464), ii) Gram negative bacteria; included facultative anaerobes and fastidious strains (n=5) Escherichia coli (ATCC-25922), Haemophilus influenza (ATCC-49247), Neisseria meningitides (ATCC-13077), Pseudomonas aeruginosa (ATCC-27853), Stenotrophomonas maltophilia (ATCC-17666), iii) Gram positive bacteria (n=6) included Enterococcus faecalis ATCC-29212), Staphylococcus aureus (ATCC-29213), Staphylococcus epidermidis (ATCC-12228), Streptococcus agalactiae (ATCC-12386), Streptococcus pneumoniae (ATCC-49619), Streptococcus pyogenes (ATCC-19615) and iv) Yeasts (n=4) included Candida albicans (ATCC-90028), Candida glabrata (ATCC-15126), Candida krusei (ATCC-6258), Candida parapsilosis (ATCC-22019).
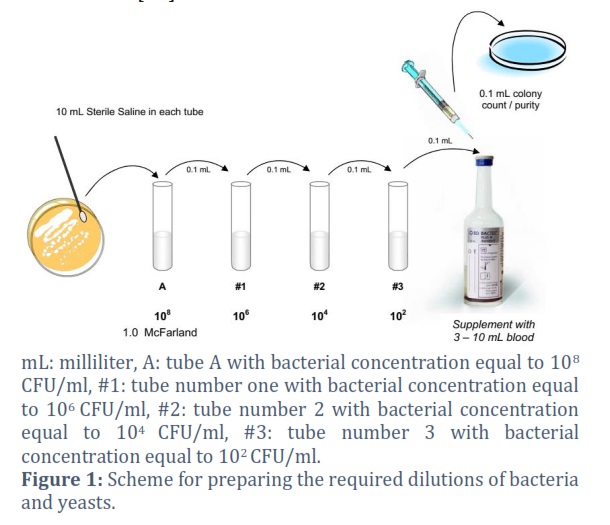
All strains were stored at minus 80°C and were sub-cultured twice to ensure complete revival and stability of the strains. These strains were suspended in 0.9% saline to yield a 1.0 McFarland bacterial suspension. The bacterial and yeast suspensions were diluted according to the scheme shown in figure 1 to yield the final suspension of 102 CFU/ml.
Inoculation of blood culture bottles and incubation
To mimic clinical conditions and for optimal growth of fastidious bacteria, 8-10ml and 2ml of human blood were inoculated in adult and pediatric bottles, respectively. The inoculum of organisms in each bottle was approximated as per the clinical course of bloodstream infection (10 to 30 CFU/per bottle). A total of 19 ATCC bacteria strains, tested in duplicates, were utilized to compare the three types of blood culture bottles of both instruments (anaerobic, aerobic, and pediatric) by simultaneous inoculation with the following ATCC bacteria or yeasts.
Anaerobic blood culture bottles were inoculated with the following seven ATCC strains (obligate anaerobes: n=4, 2 gram positive and 2-gram negative rods), facultative anaerobes: n=3). The ATCC # of these strains mentioned earlier above; Bacteroides fragilis, Bacteroides ovatus, Clostridium perfringens, Clostridium septicum, Staphylococcus aureus, Escherichia coli and Streptococcus pneumoniae. While aerobic and paediatric each blood culture bottles were inoculated with the following ATCC strains (ATCC # mentioned earlier, gram negative (n=5), gram positive (n=6) and yeasts (n=4); Escherichia coli, Haemophilus influenza, Neisseria meningitidis, Pseudomonas aeruginosa, Stenotrophomonas maltophilia, Enterococcus faecalis, Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus agalactiae, Streptococcus pneumoniae, Streptococcus pyogenes, Candida albicans, Candida glabrata, Candida krusei, Candida parapsilosis.
Briefly, each ATCC strain, 1.0 McFarland Standard (equivalent to ~3 x 108 CFU/ml) turbidity suspension was prepared and adjusted with Vitek II turbidity meter. Ten ml of 0.9% normal saline was added to each of the three sterile plastic tubes/strain. From 1.0 McFarland tube (Tube A), 0.1ml suspension was transferred to the first tube (tube # 1) (diluted to 106 CFU/ml), after proper mixing, 0.1ml of suspension was then transferred to tube # 2 and mixed well (diluted to 104 CFU/ml), it was followed by transfer of 0.1ml of suspension to tube # 3 (diluted to 102 CFU/ml). Finally, 0.1 ml was injected in respective blood culture bottles and also 0.1ml was inoculated on sheep blood agar by using a spread plate technique for verification of CFU count and purity check of the whole process of inoculum preparation. Haemophilus influenzae was inoculated onto a chocolate agar plate, gram positive onto blood agar, anaerobes on blood agar (incubated anaerobically) gram negatives onto MacConkey agar, and yeasts on Sabroud’s agar. Un-inoculated sterility control vials, vials with added human blood and no organism of both the test (BACTEC™ FX) and reference (BTA3D™) blood culture vials were included.
Statistical analysis
The assessment of the recovery rate (the total number i.e., n (%) of bottles from which microbes were recovered) and time until detection (TTDs; average value in hours) capabilities of reference and test blood culture instruments was conducted utilizing Fisher's exact test and the chi-square test.
In order to evaluate the capabilities of the two machines, the variances in mean TTDs for each microorganism between the BACTEC FX and BTA3D were computed. Comparing the means with an online calculator yielded the difference in means. This method figures out how different the observed means in two distinct samples are from one another. It reports the 95% Confidence Interval (CI) and the significance value (p-value) of the difference. The p-value represents the likelihood that the observed variation between the samples would occur if the null theory were true. The null hypothesis is the hypothesis that the difference is 0. Standard Deviation was calculated online as per Furey, Edward "Standard Deviation Calculator" at https://www.calculatorsoup.com/calculators/statistics/standard-deviation-calculator.php from Calculator Soup, https://www.calculatorsoup.com– Online Calculators[15]. The no growth (negative blood culture) cut-off was set at 120 hours. Statistical analysis was conducted using MedCalc v.19.2.6 (MedCalc Software, Ostend, Belgium), with a P < 0.05 indicating significant differences [16].
Results![]()
Bactec FX and BTA3D BC systems for seeded human blood cultures
Overall performance
BC bottles were incubated concurrently in both blood culture systems. In total, we evaluated 148 seeded blood culture bottles (28 anaerobic, 60 bottles each of aerobic & paediatric blood culture bottles). These 60 single aerobic and paediatric bottles (n=120) were inoculated with six, five, and four gram-positive, gram-negative, and yeast species, respectively. Among the five-gram negatives, 2 isolates were fastidious, namely, H. influenzae and N. meningitidis 2 were non-fermenters while one was a facultative anaerobe. All six gram-positive bacteria were facultative anaerobes. Twenty-eight anaerobic bottles were inoculated with strict anaerobic bacterial species (2 each, gram-positive & gram-negative spore-forming rods). Within the five days of the incubation period, all BC-seeded bottles (n = 148, 100%) were detected positive, while 12 control bottles (un-inoculated) signaled negative.
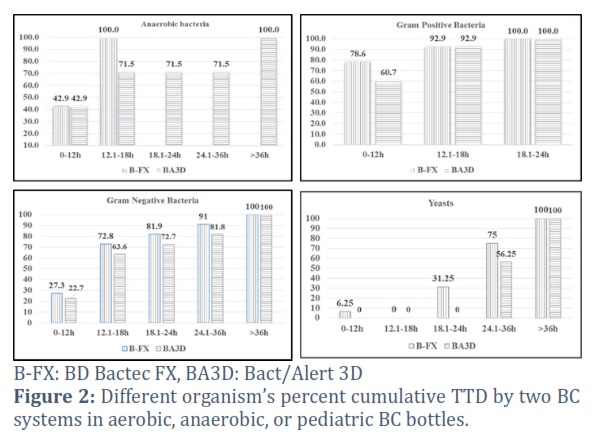
The cumulative percent TTD of different organism groups in different bottle types over time intervals in the two BC is displayed in Figure 2. The TTD of anaerobic bacteria was 100 and 75.1% at 12 hours of incubation in the Bactec FX and BTA3D systems, respectively. For gram-positive organisms, the positivity rate in Bactec FX was superior to BTA3D at 12-hour time intervals; however, for the rest of the time intervals, both instruments had a uniform distribution of percent positivity rates. Among Gram-negative bacteria, 72.8 and 63.6% of organisms reached positivity within 18 h when incubated in the Bactec FX and BTA3D systems, respectively. Among the yeasts, 75 and 56.3% of isolates reached positivity within 36hrs in Bactec FX and BTA3D systems, respectively (Figure 2).
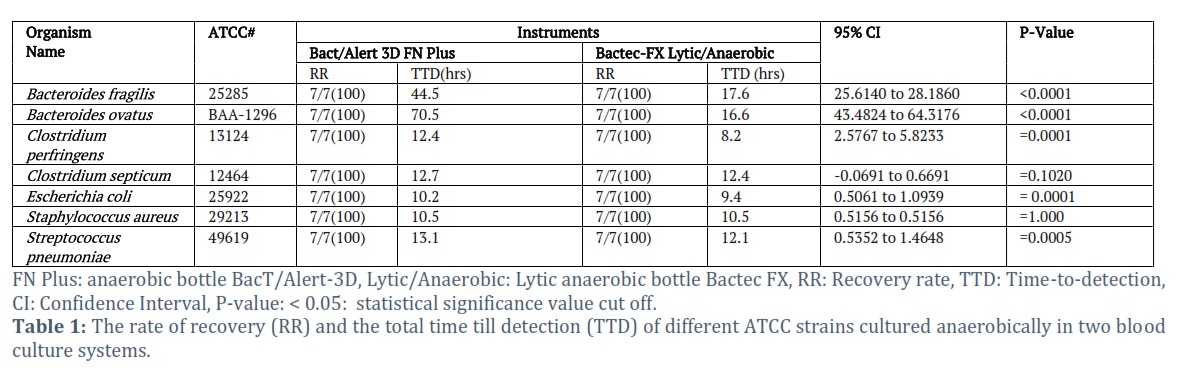
Adult anaerobic seeded BC bottles performance
The TTD of the microorganisms inoculated in anaerobic bottles of both BC systems is displayed in Table 1. The Bactec FX system, anaerobic bottles had an overall mean TTD of 12.4 hours, which was significantly shorter than anaerobic bottles incubated in the BTA3D system, which took 24.8 hours. A p-value of less than 0.05 indicated statistical significance for 71.4% of the ATCC strains that were tested.
Adult aerobic seeded BC bottles performance
Table 2 illustrates the RR, TTD and 95% CI and P value of tested ATCC isolates in Aerobic BC bottles in each BC system. Bactec FX Aerobic BC bottles mean TTD was superior (19.9hrs) to BTA3D system (24hrs). For 93.3% of the tested ATCC strains, a difference with statistical significance (p-value = <0.05) was observed.
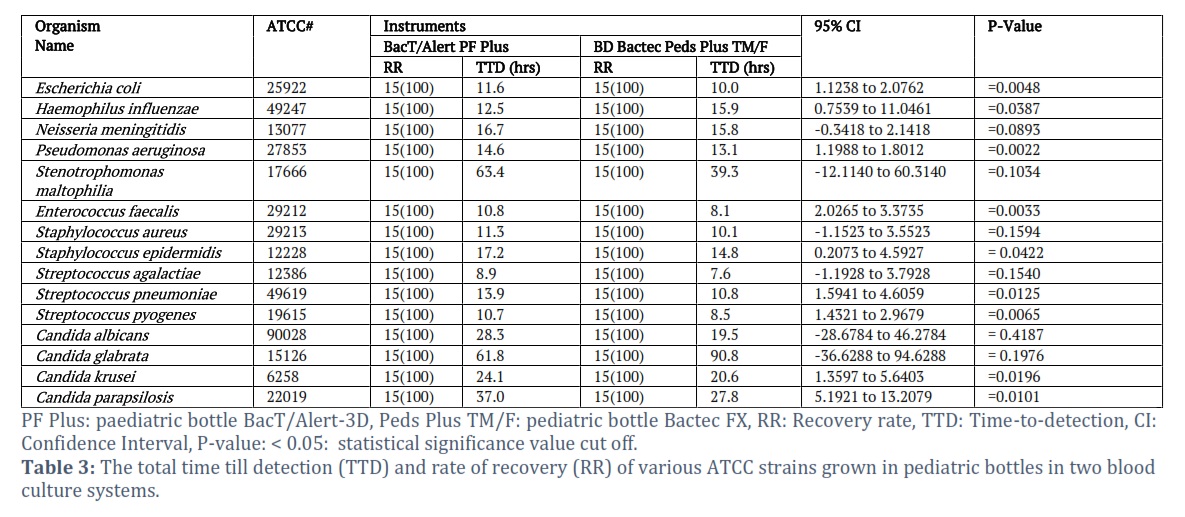
Paediatric seeded BC bottles performance
The mean TTD was substantially shorter for paediatric bottles incubated in the Bactec FX (20.8 h) system than in BTA3D (22.9 h) systems. The most significant disparities in the average TTD (≥29.5hrs) among BC systems were found for C. glabrata cultivated in paediatric bottles (Bactec FX: 90.8hrs vs. BTA3D: 61.8hrs).
Figures & Tables

Blood culture is the most common bacteremia/ fungemia test. To maximize the effectiveness of antibiotic therapy, positive blood cultures identify the etiologic agent for antimicrobial susceptibility testing. Early blood testing for the infection's etiology and starting antibiotic therapy early can improve disease outcomes [17]. Every hour of antibiotic delay has been
associated with an 18% increase in the risk of mortality at 28 days [18].
In this study, we inoculated aerobic, anaerobic and paediatric blood culture bottles with recommended ATCC strains by seeded blood culture methodology, simultaneously to evaluate the performance of two blood culture systems, Bactec FX and BTA3D automated BC systems for their capability of detecting microbial growth. All 148/148 inoculated bottles were detected as
positive in both microbial detection systems (MDS). We observed outstanding performance of Bactec FX with an overall faster TTD in comparison with BTA3D (Table, 1, 2 and 3). Overall, Bactec FX aerobic, anaerobic, and paediatric blood culture bottles and tested organism types had statistically significant TTD compared to BTA3D, i.e., 93.3%, 71.4%, and 53.3%, respectively. Most of the 19 microbial species tested were detected faster with BD Bactec FX. The notable exceptions include the findings that In BTA3D, C. glabrata aerobic and paediatric BC bottles mean TTD was faster (43.1hrs and 61.8hrs, respectively) than Bactec FX (57.8hrs and 90.8hrs, respectively). C. glabrata mean TTD was statistically significant for BTA3D aerobic BC bottle type (p = 0.0083), while it was not statistically significant for paediatric BC bottle type (p = 0.1976). The mean TTD for fastidious H. influenzae in the BTA3D paediatric bottle was 3.4 hours quicker and statistically significant (p=0.0387) than in the Bactec/FX paediatric bottle type. Despite the fact that S. epidermidis was detected earlier in aerobic BC (2.4hrs earlier TTD than Bactec FX), the difference was not statistically significant. The most significant difference in the mean TTD (≥53.9hrs) by BC systems regarded B. ovatus when cultured in anaerobic bottles; p<0.001. Anaerobic bottles incubated in Bactec FX showed a statistically significant finding (p-value= <0.05) for 71.4% of tested ATCC strains compared to its competitor BTA3D. Mueller-Premru and colleagues reported similar findings [19]. Another study from Jeddah, Saudi Arabia, reported the shortest median TTD for anaerobes in Bactec FX (18hrs) compared to BacT/ALERT FN (23.5hrs) [20, 21]. BSI due to anaerobic bacteria is associated with high mortality despite having a lower clinical occurrence than aerobic bacteria. Therefore, for optimal patient’s management, timely, rapid detection and identification of the causative agent, as well as the delivery of appropriate antimicrobials, are of utmost importance [22, 23]. The S. maltophilia mean TTD when cultured in aerobic bottles was statistically significant, with a remarkable difference of 33.5hrs early detection i.e. (39hrs by Bactec FX vs. 72.5hrs by BTA3D; p-value= <0.05).
The mean TTD of Bactec FX paediatric bottles was superior for 86.7% of tested ATCC strains. The only two exceptions were H. influenzae and C. glabrata. Similarly, aerobic blood culture bottles incubated in Bactec FX had a faster TTD for 86.7% (p=<0.05) of tested ATCC strains. The only exception when BTA3D showed a statistically significant mean TTD (p=0.0083) was for C. glabrata (14.7hrs early detection) compared to the competitor Bactec FX (table 2 and 3). Significantly shorter recovery time was observed in a research study, comparing aerobic bottles of Bactec FX and Bact/Alert 3D (17.2 and 24.7 h, respectively) (P < 0.001) [24].
Among yeast, overall, Bactec FX mean TTD was faster than BTA3D, a few notable examples include C. parapsilosis, both aerobic and paediatric bottles (p= 0.0074 and 0.0101, respectively) and C. krusei, both paediatric and aerobic bottles, which had an early mean TTD (p= 0.0196 and 0.001, respectively), as shown in tables 2 and 3.
In conclusion, our research study demonstrates that the Bactec FX outperformed the BTA3D system in terms of early identification of tested microorganisms. The faster time to positivity may significantly decrease patient morbidity and mortality by facilitating earlier administration of the appropriate antimicrobial medication. To confirm this, a larger clinical specimen-based investigation is required.
Acknowledgement
The authors thank the microbiology laboratory staff at King Abdulaziz Hospital National Guard, AlAhsa, Saudi Arabia, for their help in seeding blood cultures.
Author Contributions
Muhammad Absar and Ibraheem AlShahrani designed the study and supervised the experiment. Fahd AlNashmy Mosa Salami, Ali Hadadi, Aous AlMarzooq, Alhussain AlAsiri, Abdulaziz AlRashidi, Mohammed AlFaifi performed the experiments. Muhammad Absar, Fahd AlNashmy, Ali Hadadi, Aous AlMarzooq, Mohammed AlFaifi performed data analysis. Muhammad Absar & Ibraheem AlShahrani wrote the manuscript. All the authors read and sanctioned the final version of the manuscript.
The author declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- Rhee C, Dantes R, Epstein L, Murphy DJ, Seymour CW, et al. Incidence and Trends of Sepsis in US Hospitals Using Clinical vs Claims Data, 2009-2014. The Journal of the American Medical Association, (2017); 318(13): 1241-1249.
- Hattori H, Maeda M, Nagatomo Y, Takuma T, Niki Y, et al. Epidemiology and risk factors for mortality in bloodstream infections: A single-center retrospective study in Japan. American Journal of Infection Control, (2018); 46(12): e75-e79.
- Kumar G, Kumar N, Taneja A, Kaleekal T, Tarima S, et al. Nationwide trends of severe sepsis in the 21st century (2000-2007). Chest, (2011); 140(5): 1223-1231.
- Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clinical Microbiology and Infection, (2013); 19(6): 501-509.
- Palmer HR, Palavecino EL, Johnson JW, Ohl CA, Williamson JC. Clinical and microbiological implications of time-to-positivity of blood cultures in patients with Gram-negative bacilli bacteremia. European Journal of Clinical Microbiology & Infectious Diseases, (2013); 32(7): 955-959.
- Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Critical Care Medicine Journal, (2014); 42(8): 1749-1755.
- Adhikari NK, Fowler RA, Bhagwanjee S, Rubenfeld GD. Critical care and the global burden of critical illness in adults. The Lancet, (2010); 376(9749): 1339-1346.
- Lamy B, Dargere S, Arendrup MC, Parienti JJ, Tattevin P. How to Optimize the Use of Blood Cultures for the Diagnosis of Bloodstream Infections? A State-of-the Art. Frontiers in Microbiology, (2016); 7: 697.
- Armstrong-Briley D, Hozhabri NS, Armstrong K, Puthottile J, Benavides R, et al. Comparison of length of stay and outcomes of patients with positive versus negative blood culture results. Baylor University Medical Center Proceedings, (2015); 28(1): 10-13.
- Boev C, Kiss E. Hospital-Acquired Infections: Current Trends and Prevention. Critical Care Nursing Clinics of North America, (2017); 29(1): 51-65.
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Medicine, (2017); 43(3): 304-377.
- Zhang J, Yang F, Sun Z, Fang Y, Zhu H, et al. Rapid and precise identification of bloodstream infections using a pre-treatment protocol combined with high-throughput multiplex genetic detection system. BMC Infectious Diseases, (2022); 22(1): 823.
- Wilson ML, Mitchell M, Morris AJ, Murray PR, Reimer LG, et al. CLSI. Principles and Procedures for Blood Cultures; Approved Guideline. Approved Guideline. In., vol. 27, No. 17, M47-A edn. Wayne, PA: Clinical and Laboratory Standards Institute, (2007).
- O'Hara CM. Manual and automated instrumentation for identification of Enterobacteriaceae and other aerobic gram-negative bacilli. Clinical Microbiology Reviews, (2005), 18(1): 147-162.
- "Standard Deviation Calculator" at https://www.calculatorsoup.com/calculators/statistics/standard-deviation-calculator.php from CalculatorSoup, https://www.calculatorsoup.com – Online Calculators, accessed October 5, 2023).
- MedCalc Software Ltd. Comparison of means calculator. https://www.medcalc.org/calc/comparison_of_means.php (Version 22.013; accessed October 5, 2023).
- Khatib R, Saeed S, Sharma M, Riederer K, Fakih MG, et al. Impact of initial antibiotic choice and delayed appropriate treatment on the outcome of Staphylococcus aureus bacteremia. European Journal of Clinical Microbiology & Infectious Diseases, (2006); 25(3): 181-185.
- Rosa RG, Goldani LZ. Cohort study of the impact of time to antibiotic administration on mortality in patients with febrile neutropenia. Antimicrobial Agents and Chemotherapy, (2014); 58(7): 3799-3803.
- Mueller-Premru M, Jeverica S, Papst L, Nagy E. Performance of two blood culture systems to detect anaerobic bacteria. Is there any difference? Anaerobe, (2017), 45: 59-64.
- Almuhayawi M, Altun O, Abdulmajeed AD, Ullberg M, Ozenci V. The Performance of the Four Anaerobic Blood Culture Bottles BacT/ALERT-FN, -FN Plus, BACTEC-Plus and -Lytic in Detection of Anaerobic Bacteria and Identification by Direct MALDI-TOF MS. PLoS One, (2015); 10(11): e0142398.
- Rocchetti A, Di Matteo L, Bottino P, Foret B, Gamalero E, et al. Prospective study of the clinical performance of three BACTEC media in a modern emergency department: Plus Aerobic/F, Plus Anaerobic/F, and Anaerobic Lytic/F. Journal of Microbiological Methods, (2016); 130: 129-132.
- Kim J, Lee Y, Park Y, Kim M, Choi JY, et al. Anaerobic Bacteremia: Impact of Inappropriate Therapy on Mortality. Journal of Infection and Chemotherapy, (2016); 48(2): 91-98.
- Vena A, Munoz P, Alcala L, Fernandez-Cruz A, Sanchez C, et al. Are incidence and epidemiology of anaerobic bacteremia really changing? European Journal of Clinical Microbiology & Infectious Diseases, (2015); 34(8): 1621-1629.
- Roh KH, Kim JY, Kim HN, Lee HJ, Sohn JW, et al. Evaluation of BACTEC Plus aerobic and anaerobic blood culture bottles and BacT/Alert FAN aerobic and anaerobic blood culture bottles for the detection of bacteremia in ICU patients. Diagnostic Microbiology and Infectious Disease, (2012); 73(3): 239-242.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0