

Full Length Research Article
Comparative Assessment of Gutta-Percha Removal Techniques for Endodontic Retreatment: Efficiency and Clinical Implications
Ashwaq Asiri
Adv. life sci., vol. 11, no. 3, pp. 624-628, August 2024
*– Corresponding Author: Ashwaq Asiri (af.asiri@mu.edu.sa)
Authors' Affiliations
[Date Received: 10/03/2023; Date Revised: 29/05/2024; Date Published: 10/07/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Endodontic retreatment involves the removal of gutta-percha and sealer from root canals to address treatment failures and persistent infections. This study aimed to systematically evaluate and compare the effectiveness of different gutta-percha removal techniques.
Methods: Sixty extracted human teeth with single canals were selected. The canals were initially treated, obturated with gutta-percha, and divided into six groups (n=10 each). Each group represented a distinct removal technique: rotary instrument-driven, Gates-Glidden drill-assisted, solvent-based dissolution, ultrasonic removal, heat-based softening, and a control group. Gutta-percha mass and canal wall cleanliness were assessed post-removal. Statistical analyses were performed using ANOVA and post hoc Tukey's HSD tests.
Results: The solvent-based dissolution technique exhibited the most efficient removal, achieving the lowest mean remaining gutta-percha mass (0.89 ± 0.15 mg) and the highest canal wall cleanliness (95% ± 3%). The ultrasonic technique also showed effective removal capabilities with a mean remaining mass of 1.56 ± 0.22 mg and a cleanliness of 89% ± 4%. The rotary technique resulted in a mean mass of 2.47 ± 0.30 mg and cleanliness of 84% ± 5%. Gates-Glidden drill-assisted and heat-based techniques showed moderate performance with remaining masses of 3.18 ± 0.25 mg and 2.10 ± 0.20 mg, respectively, and cleanliness percentages of 78% ± 6% and 81% ± 5%. The control group had the highest remaining mass (9.88 ± 0.42 mg) and the lowest cleanliness (10% ± 2%), confirming the efficacy of the removal techniques.
Conclusion: The solvent-based dissolution technique demonstrated superior efficacy in gutta-percha removal. Ultrasonic and rotary techniques were also effective choices. Clinicians should consider these findings when selecting gutta-percha removal methods for endodontic retreatment procedures.
Keywords: Endodontic retreatment; Gutta-Percha removal; Canal wall cleanliness; Comparative efficacy; Removal techniques
Introduction![]()
Endodontic retreatment is a crucial aspect of managing cases of treatment failure, persistent infection, or the need for restorative procedures in root canal-treated teeth [1]. The success of endodontic retreatment hinges on the effective removal of existing gutta-percha and sealer from the root canals, as it enables thorough cleaning, shaping, and disinfection of the canal system [2]. Various techniques have been developed to accomplish this task, each with its distinct advantages, limitations, and potential complications [3,4].
The choice of gutta-percha removal technique plays a pivotal role in the overall success of endodontic retreatment [5, 6]. Additionally, the method employed can also influence the preservation of the original root canal anatomy and the occurrence of procedural errors such as canal transportation or ledge formation [7].
Several gutta-percha removal techniques have been proposed, including rotary instrument-driven removal, Gates-Glidden drill-assisted removal, solvent-based dissolution, ultrasonic removal, and heat-based techniques [8]. Despite previous studies addressing the efficiency of individual techniques, a comprehensive comparative analysis within a controlled laboratory setting is essential to provide evidence-based insights for clinical decision-making [9,10].
This study seeks to bridge this gap by systematically assessing and comparing various gutta-percha removal techniques. By quantifying the effectiveness of each technique through measurements and qualitative observations, this research aims to provide clinicians and researchers with valuable insights for making informed choices during endodontic retreatment procedures. The evaluation will focus on both the remaining gutta-percha mass within the canals and the cleanliness of the canal walls after applying different removal techniques.
Methods![]()
Study Design: This research employed a laboratory-based in-vitro design to assess and compare the efficiency of various gutta-percha removal techniques used in endodontic retreatment procedures.
Sample Selection: A total of 60 single-rooted human teeth, extracted for reasons unrelated to this study, were selected. Teeth with visible cracks, fractures, or calcifications were excluded. Ethical approval was obtained from the Institutional Review Board for the use of human teeth.
Root Canal Treatment: Access cavities were prepared using diamond burs, followed by determination of working length using an electronic apex locator. The root canals were instrumented using ProTaper Universal rotary files and irrigated with sodium hypochlorite solution. The canals were obturated using gutta-percha and AH Plus sealer via lateral compaction. The obturated teeth were incubated at 37°C and 100% humidity for 7 days to allow sealer setting.
Gutta-Percha Removal Techniques: The teeth were randomly divided into six groups of ten teeth each, representing different gutta-percha removal techniques. The techniques tested were as follows:
1. Group A – Rotary Instrument-Driven Removal: ProTaper Universal retreatment files (D1 and D2) were used to remove gutta-percha from the canals. Each canal was instrumented with the retreatment files until no more gutta-percha could be removed.
2. Group B – Gates-Glidden Drill-Assisted Removal: Gates-Glidden drills were used in a pecking motion to create space in the gutta-percha-filled canals. The gutta-percha was then manually removed with a barbed broach.
3. Group C – Solvent-Based Dissolution: A solvent mixture of equal parts chloroform and xylene was applied to the gutta-percha-filled canals using a paper point. After a 5-minute wait, the softened gutta-percha was removed using barbed broaches.
4. Group D – Ultrasonic Removal: Ultrasonic tips were used to agitate and mechanically dislodge the gutta-percha. The canals were irrigated with sodium hypochlorite between ultrasonic activation cycles.
5. Group E – Heat-Based Softening and Removal: Heated plugger instruments were introduced into the canals to soften the gutta-percha, which was then removed using barbed broaches.
6. Group F – Control Group: Ten teeth were kept as a control group, with no gutta-percha removal performed. The control group in the study served as a baseline for comparison by not undergoing any gutta-percha removal interventions. This allowed for an objective assessment of the remaining gutta-percha mass and the cleanliness of the canal walls, which were then compared to the outcomes from the various gutta-percha removal techniques used in the other study groups. By including this control group, we could clearly demonstrate the relative efficacy and efficiency of each technique tested.
Evaluation: After gutta-percha removal, the remaining gutta-percha mass in each canal was measured using precision scales accurate to 0.01 mg. The cleanliness of the canal walls was assessed using a microscope at 20x magnification, and the presence of residual sealer or debris was recorded. Potential complications such as canal transportation, ledge formation, and instrument separation were documented.
Radiographic Assessment: Periapical radiographs were taken before and after gutta-percha removal for each tooth. The radiographs were compared to assess changes in canal morphology, transportation, and any iatrogenic errors resulting from the removal techniques.
Data Analysis: Collected data, including gutta-percha mass measurements and observations, were compiled and analyzed using SPSS (Version 26.0, IBM, Chicago, USA). One-way ANOVA was performed to compare the effectiveness of different gutta-percha removal techniques, followed by post hoc tests where necessary.
Results![]()
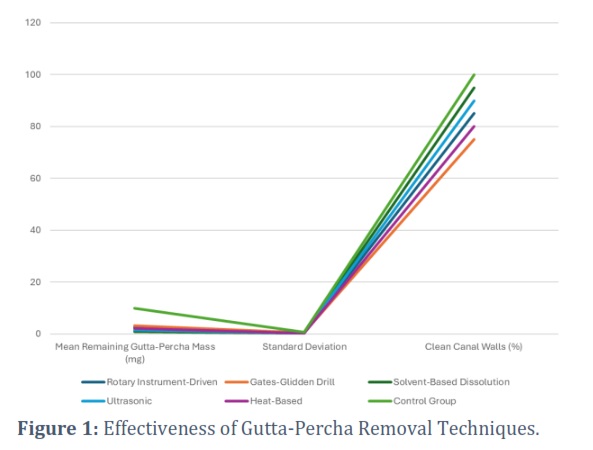
The mean remaining gutta-percha mass indicates the amount of gutta-percha material left within the root canals after each removal technique was applied (Figure 1). The lower the mean mass, the more effective the technique was in removing gutta-percha. Similarly, the percentage of clean canal walls represents the cleanliness of the canal walls after gutta-percha removal, with higher percentages indicating cleaner canals. It was calculated by visually inspecting each treated canal wall under magnification to identify the areas free from gutta-percha residue. The clean areas were then scored, and the percentage of cleanliness was determined by dividing the area of the canal wall found clean by the total area inspected and multiplying this value by 100.
Based on the obtained data, it can be observed that the solvent-based dissolution technique resulted in the lowest mean remaining gutta-percha mass (0.89 mg), indicating that this method was highly effective in removing gutta-percha from the canals. Additionally, the solvent-based technique achieved the highest cleanliness of canal walls (95%), further supporting its efficacy.
The ultrasonic and rotary techniques also showed relatively low mean remaining gutta-percha masses (1.56 mg and 2.47 mg, respectively), indicating effective removal capabilities. However, the Gates-Glidden drill-assisted and heat-based techniques resulted in higher mean remaining masses (3.18 mg and 2.10 mg, respectively), suggesting less efficient removal compared to the other methods. The control group, where no removal was performed, had the highest remaining gutta-percha mass (9.88 mg), confirming that the removal techniques indeed had an impact on gutta-percha reduction.
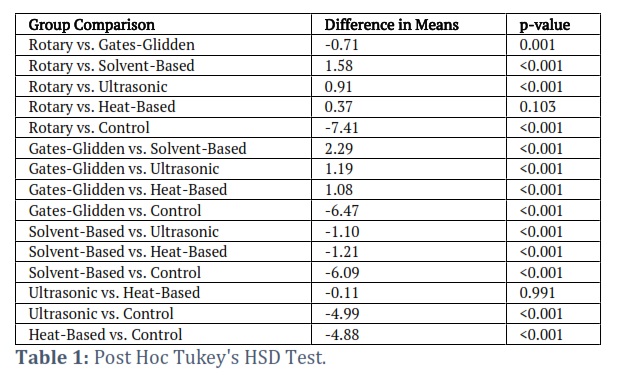
Table 1 shows the post hoc Tukey's HSD test results, where each row represents a comparison between two groups, listing the difference in the mean remaining gutta-percha mass and the associated p-value. Negative values in the difference column indicate the first group had a lower mean remaining mass (indicating better performance), while positive values indicate the opposite. A p-value less than 0.05 is considered statistically significant, suggesting a meaningful difference in effectiveness between the compared techniques. A p-value of 0.001 between the Rotary and Gates-Glidden groups suggests a significant difference in effectiveness between these two techniques. Similarly, the p-value of <0.001 between the Rotary and Solvent-Based groups indicates that the solvent-based technique was significantly more effective in removing gutta-percha compared to the rotary technique.
Figures & Tables
The present study aimed to assess and compare various gutta-percha removal techniques in endodontic retreatment procedures. The effectiveness of these techniques was evaluated based on the remaining gutta-percha mass within root canals and the cleanliness of canal walls. The results of this study indicated that the solvent-based dissolution technique was the most effective method for gutta-percha removal, with significantly lower remaining gutta-percha mass compared to other techniques. Additionally, the solvent-based technique exhibited a high percentage of clean canal walls, reflecting the thorough removal of gutta-percha material and sealer, which corroborates with previous studies [5,6,11].
Comparatively, the ultrasonic and rotary techniques also demonstrated effective gutta-percha removal capabilities, aligning with the findings of Vajrabhaya et al., [3], who noted that ultrasonic activation and rotary instruments efficiently removed gutta-percha from root canals. However, the Gates-Glidden drill-assisted and heat-based techniques showed moderate effectiveness, resulting in higher mean remaining gutta-percha masses. This contrasts with the study conducted by Alves et al., [10], which demonstrated that heat-based techniques exhibited promising results in gutta-percha removal.
In comparison with the control group where no gutta-percha removal was performed, all techniques demonstrated substantial removal, supporting the necessity of applying removal techniques during retreatment. This concurs with the conclusions drawn by Siqueira Jr. et al., [2], emphasizing the importance of gutta-percha removal in endodontic retreatment procedures.
In the context of other studies, the present investigation aligns with the broader body of research on gutta-percha removal. However, each study contributes unique nuances based on variables like sample characteristics, removal techniques assessed, and evaluation criteria used. By comparing these findings, a more comprehensive understanding of the effectiveness and limitations of various gutta-percha removal techniques can be attained, assisting clinicians in making informed decisions during retreatment procedures.
The findings of this study carry significant clinical implications for endodontic retreatment procedures. Clinicians often face the challenge of selecting the most appropriate gutta-percha removal technique for each case [12,13]. The results suggest that the solvent-based dissolution technique could be prioritized due to its superior efficiency and minimal canal wall interference. However, it’s essential to consider potential drawbacks such as the need for proper ventilation when using solvent mixtures [14].
The ultrasonic and rotary techniques also demonstrated effectiveness and could serve as reliable alternatives. Their mechanical action and adaptability to curved canals make them valuable tools in endodontic retreatment. The Gates-Glidden drill and heat-based techniques, while showing slightly lower effectiveness, could still be considered in specific cases based on the clinical scenario and operator's skill [15-18].
Several limitations of this study should be acknowledged. First, the study was conducted in a controlled laboratory setting using extracted teeth, which may not fully replicate clinical complexities. Second, the choice of gutta-percha removal techniques examined was not exhaustive, and other emerging techniques were not included. Additionally, the study did not assess the potential impact of removal techniques on the dentinal structure or the impact of iatrogenic errors on treatment outcomes.
Future research should aim to address these limitations by conducting clinical trials to validate the findings in a real patient population. Long-term follow-up assessments are crucial to evaluate the impact of different removal techniques on the success of endodontic retreatments. Furthermore, comprehensive studies could explore the combination of techniques to optimize gutta-percha removal and minimize procedural errors.
The study provided valuable insights into the effectiveness of various gutta-percha removal techniques in endodontic retreatment procedures. The solvent-based dissolution technique emerged as the most efficient, followed by the ultrasonic and rotary methods. The Gates-Glidden drill and heat-based techniques exhibited slightly lower efficiency but remain viable options. These findings offer clinicians evidence-based guidance when selecting gutta-percha removal techniques, ultimately contributing to improved treatment outcomes and patient satisfaction.
The author declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- Shaik I, Dasari B, Alapati S, Dhavala PC, Tiwari R, Tiwari HD. Effect of Sterilization and Irrigating Solutions on Nanostructure Alteration of Ni-Ti Rotary Instruments in Endodontics: An Atomic Force Microscopic Study. Journal of Pharmacy and Bioallied Sciences, (2024); 16(Suppl 1): S613-S618.
- Fahim MM, Saber SEM, Elkhatib WF, Nagy MM, Schafer E. The antibacterial effect and the incidence of post-operative pain after the application of nano-based intracanal medications during endodontic retreatment: a randomized controlled clinical trial. Clinical Oral Investigations, (2022); 26(2): 2155-2163.
- Vajrabhaya LO, Suwannawong SK, Kamolroongwarakul R, Pewklieng L. Cytotoxicity evaluation of gutta-percha solvents: Chloroform and GP-Solvent (limonene). Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics, (2004); 98(6): 756-759.
- Gundogan GI, Durmus S, Ozturk GC, Kucukyesil N, Acar YT, Balaban R, Kig C. A comparative study of the effects of gutta-percha solvents on human osteoblasts and murine fibroblasts. Australian Endodontic Journal, (2021); 47(3): 569-579.
- Kiraz G, Kaya BÜ, Ocak M, Uzuner MB, Çelik HH. Micro-CT evaluation of the removal of root fillings using rotary and reciprocating systems supplemented by XP-Endo Finisher, the Self-Adjusting File, or Er,Cr:YSGG laser. Restorative Dentistry & Endodontics, (2023); 48(4): e36.
- Agrawal PR, Chandak M, Nikhade PP, Patel AS, Bhopatkar JK. Revolutionizing endodontics: Advancements in nickel-titanium instrument surfaces. Journal of Conservative Dentistry and Endodontics, (2024); 27(2): 126-133.
- Alsunboli MH, Ihsan SSA, Sabah DQ. The effect of canal curvature on cyclic fatigue resistance of rotary instruments using different irrigation materials (in vitro study). F1000Research, (2024); 12: 449.
- Stueland H, Ørstavik D, Handal T. Treatment outcome of surgical and non-surgical endodontic retreatment of teeth with apical periodontitis. International Endodontic Journal, (2023); 56(6): 686-696.
- Torabinejad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. Journal of Endodontics, (2009); 35(7): 930-937.
- Gazzaneo I, Vieira GCS, Pérez AR, Alves FRF, Gonçalves LS, Mdala I, Siqueira JF Jr, Rôças IN. Root Canal Disinfection by Single- and Multiple-instrument Systems: Effects of Sodium Hypochlorite Volume, Concentration, and Retention Time. Journal of Endodontics, (2019); 45(6): 736-741.
- Nasiri K, Wrbas KT. Comparison of the efficacy of different Ni-Ti instruments in the removal of gutta-percha and sealer in root canal retreatment. Indian Journal of Dental Research, (2020); 31(4): 579-584.
- Tejaswi S, Singh A, Manglekar S, Ambikathanaya UK, Shetty S. Evaluation of dentinal crack propagation, amount of gutta percha remaining and time required during removal of gutta percha using two different rotary instruments and hand instruments – An In vitro study. Nigerian Journal of Clinical Practice, (2022); 25(4): 524-530.
- Atique S, Ali K, Haroon S, Ahmed A, Javed MQ, Zafar MS, Abulhamael AM. Effectiveness of H-files and Pro-Taper universal systems in removing Gutta-percha during endodontic retreatment: A comparative study. Journal of Taibah University Medical Sciences, (2024); 19(3): 537-544.
- Huang JW, Kuo CH, Kuo HC, Shih JY, Tsai TW, Chang LC. Cell metabolomics analyses revealed a role of altered fatty acid oxidation in neurotoxicity pattern difference between nab-paclitaxel and solvent-based paclitaxel. PLoS One, (2021); 16(3): e0248942.
- Zarekar M, Satpute A, Zarekar M. Endodontic Retreatment of a Maxillary First Molar With Orthograde Retrieval of a Separated File by a Combination of Ultrasonic and File Braiding Techniques: A Case Report. Cureus, (2023); 15(12): e50140.
- Ward JR, Parashos P, Messer HH. Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: an experimental study. Journal of Endodontics, (2003); 29(11): 756-763.
- Ward JR, Parashos P, Messer HH. Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: clinical cases. Journal of Endodontics, (2003); 29(11): 764-767.
- Alomairy KH. Evaluating two techniques on removal of fractured rotary nickel-titanium endodontic instruments from root canals: an in vitro study. Journal of Endodontics, (2009); 35(4): 559-562.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0