

Full Length Research Article
Association between vitamin D levels and insulin resistance in patients with type 2 diabetes mellitus
Muntaha Abdulmajeed Arif *1, Manal Kamal Rasheed2, Ammar Adil Ismaeel3
Adv. life sci., vol. 11, no. 2, pp. 419-424, May 2024
*- Corresponding Author: Muntaha Abdulmajeed Arif (montaha.abdulmajeed1109f@comed.uobaghdad.edu.iq)
Authors' Affiliations
2. Clinical biochemistry, College of Medicine, Baghdad University – Iraq
3. Department of Cardiology, FIBMS Interventional Cardiology, Ministry of Health, Medical City Department – Iraqi Center for Heart Disease – Iraq
[Date Received: 18/08/2023; Date Revised: 17/03/2024; Date Available Online: 18/04/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Insulin resistance (IR) is a major contributor to type 2 diabetes mellitus (T2DM) and is associated with various metabolic disorders. Vitamin D deficiency (VDD) has been linked to an increased risk of T2DM, but the relationship between vitamin D status and IR in T2DM patients remains unclear. This study explores this association in a male population with T2DM in Baghdad, Iraq.
Methods: A case-control study was conducted on 190 male participants: 40 healthy controls and 150 patients categorized into different groups; 40 diabetic patients, 55 with coronary artery disease (CAD) and T2DM (CAD+DM), and 55 with only CAD. Physicians diagnosed them, and they were evaluated by physical and full medical history. All the sample set parameters were measured in the fasting state for each group. The biochemical tests included body mass index (BMI), vitamin D levels, insulin levels, fasting tests glucose (FBG), and HbA1c were measured. Insulin resistance was calculated using the HOMA-IR model.
Results: Vitamin D levels were significantly lower in all diabetic groups (DM, CAD+DM) compared to the control group (p<0.001). All diabetic patients had insulin resistance. BMI was significantly higher in the CAD and CAD+DM groups compared to controls (p<0.00001, p<0.004). FBG, HbA1c, insulin levels, and HOMA-IR were all significantly higher in diabetic patients compared to controls (p<0.001 for all). Furthermore, increased HbA1c, fasting insulin, and homeostatic model assessment for insulin resistance (HOMA-IR) were associated with CAD progression in T2DM patients (p < 0.001).
Conclusion: This study suggests that vitamin D deficiency may contribute to insulin resistance in male T2DM patients in Baghdad, Iraq. Maintaining optimal vitamin D levels may be beneficial in diabetes management in this population. Incorporating vitamin D screening into routine check-ups for T2DM patients could aid in early detection and prevention of insulin resistance-associated complications.
Keywords: Diabetes mellitus; Insulin resistance; Vitamin D; Coronary artery disease
Introduction![]()
Insulin resistance (IR) represents a pathological state marked by decreased sensitivity to insulin and increased resistance to its effects. IR is associated with various metabolic ailments, including obesity, type 2 diabetes mellitus (T2DM), and cardiovascular disease [1]. Genetic and environmental factors, such as obesity, may be important contributors to the etiology of IR [2]. One of the main factors in the pathophysiology of T2DM is IR, where compensatory insulin secretion fails, resulting in high blood glucose levels [3]. Exploring the underlying mechanisms of IR could significantly impact efforts to prevent the occurrence of T2DM.
Vitamin D (VD) is a fat-soluble vitamin, can be obtained through two main sources: synthesis in the skin upon exposure to sunlight and dietary intake from sources rich in VD like fatty fish [4]. It has been implicated in the regulation of various mechanisms such as cell proliferation, immunological response, glucose metabolism, and inflammatory processes [5].
Multiple investigations have highlighted the implication of VD in various metabolic diseases, including T2DM. Additionally, growing evidence has suggested a correlation between VD levels and the likelihood of diabetes mellitus (DM). VDD is hypothesized to be a potential contributor to the development of IR and T2DM, potentially affecting insulin secretion and sensitivity. Through vitamin D receptors (VDR) located in pancreatic beta cells, VD affects the release of insulin [6,7].
According to a meta-analysis, in diabetic patients, an inverse association was observed between VD levels and BMI, glucose homeostasis impairment, and HOMA-IR. Observational studies, involving animal models and human subjects, have reported an association between VDD and both IR, and T2DM, suggesting a beneficial impact of VD in obesity, IR, and T2DM [8]. There are several ways in which VD can affect insulin sensitivity, some of which are still not fully understood. According to several pieces of research, VD enhances the transcription and quantity of insulin receptors in tissues that respond to insulin by interacting with VDR. Additionally, VD can affect the extracellular calcium concentration and flow through the insulin-responsive cell, which in turn activates the glucose transporters and improves the cell’s responsiveness to insulin [9]. Furthermore, VD may inhibit the impact of inflammatory cytokines on insulin signaling by suppressing the release of inflammatory cytokines and modulating the immune system [10]. However, the protective function of VD in preventing IR remains ambiguous. So, the objective of this work is to explore the underlying mechanisms and potential of VDD in IR.
Methods![]()
Subjects and design
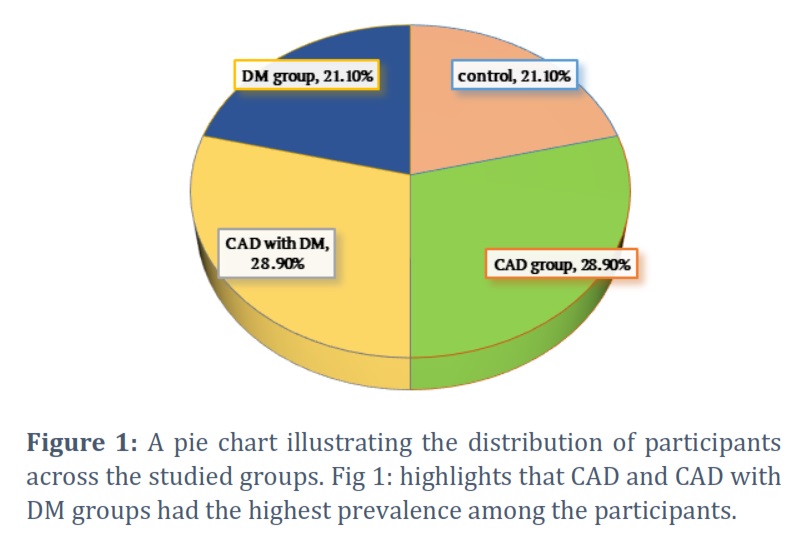
This case-control study included 190 Male; 40 (21.1%) as health control, and 150 patients classified into three groups; 40 (21.1%) diabetic patients, 55 (28.9 %) patients with CAD, and 55 (28.9 %) patients had DM and CAD. Participants were collected from those admitted to The Specialized Center for Endocrinology and Diabetes, Iraqi during the period from Feb 2022 to Nov 2022.
Sample collection
Blood samples were obtained via vein puncture following a 12-hour fasting period, with 4 ml collected from each subject. Of this, 2 ml was placed in an EDTA tube for subsequent HbA1c analysis. The remaining 2 ml was collected in a tube and left at room temperature. Following a clotting period of 10 minutes, the sample was centrifuged at 2000 rpm. The separated serum stored at −20 °C for VD level, insulin, and FBG analysis. HbA1c was estimated by an HPLC method using Bio-Rad method [11]. The serum 25-Hydroxy Vitamin D3 was measured following the manufacturer protocol of ELISA kit (My BioSource, USA, Cat. No MBS580159) [12]. The serum 25-Hydroxy Vitamin D3 concentration > 30 ng/mL, between 20–30 ng/mL, and < 20 were considered as sufficient, insufficient, and deficient respectively [13]. Insulin concentrations in serum were measured using (ELISA) kit from ALPCO (Salem, NH, USA), serum glucose levels were measured using kit (Shinyang, Busan, Korea) and HOMA-IR was calculated with a standard formula from fasting glucose and insulin levels [14].
Inclusion criteria
Men aged from 41to 75 with confirmed diagnosis of T2DM based on medical records or clinical assessment. will be enrolled in this in this research.
Exclusion criteria
Men with other types of diabetes, chronic kidney disease, liver disease, hyperparathyroidism, or those utilizing VD supplements or medications that impact VD level.
Ethical approval
Authors have been signing on an ethical consideration’s approval, and the project was approved by the local ethical committee Iraqi Ministry of Health, – Medical City / National Center for Educational Laboratories. Medical City / Iraqi Center for Heart Disease according to the code number (ISU.134 – Date 23.1.2022).
Statistical analysis
The SPSS software, version 26, was utilized for statistical analysis (SPSS Inc., Chicago, IL, USA). The expression for continuous variables was mean ± standard deviation (SD). Frequencies and percentages are used to represent categorical variables. Continuous data were compared using the ANOVA test [15].
Results![]()
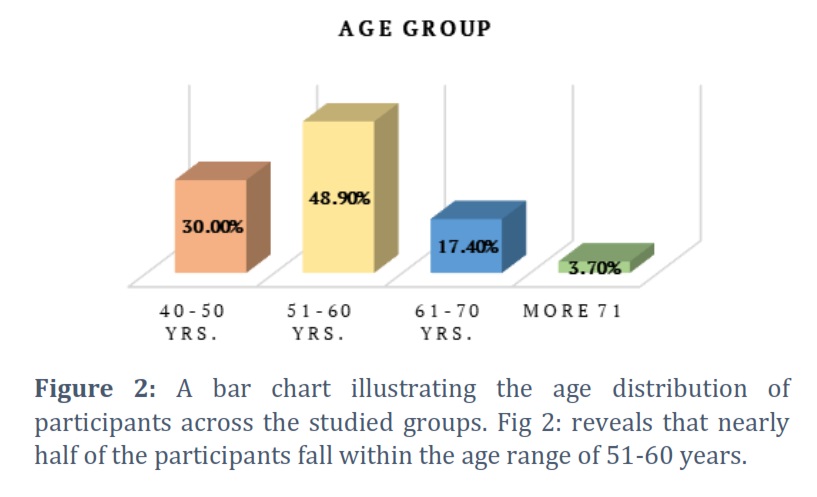
As shown in Figure 1, the study included 190 participants divided into 4 groups; 40 health control, 40 diabetic patients, 55 patients with CAD, and 55 patients had DM and CAD. As shown in Figure 2, the Mean age of included patients was 56.06 ± 7.22, with a range of (41-75) yrs. regarding the age groups, 48.9% of included patients were aged 51-60 yrs., 30.0% were aged 41-50 yrs., 17.4% were 61-70 yrs. and 3.7% were ≥ 71 yrs. the mean age in each group was 55.00±5.90, 55.15±8.49, 58.49±7.19 and 48.85±5.83 in DM, CAD, CAD with DM and control group respectively.
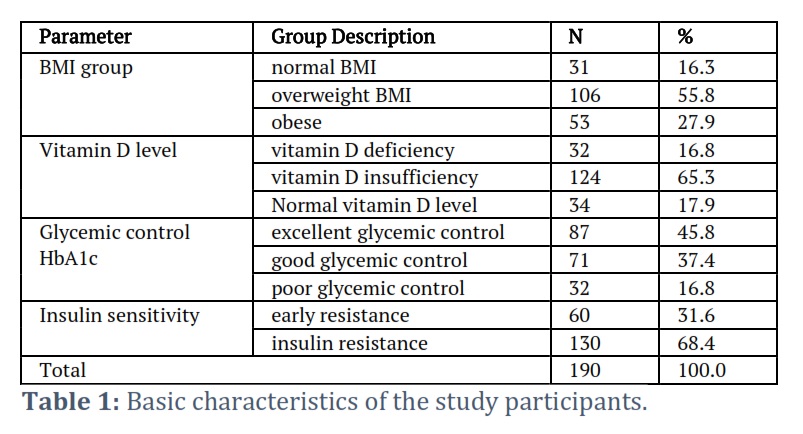
Table 1 shows the basic characteristics of the study participants including the BMI, VD status, glycemic control, and insulin sensitivity in all participants. According to BMI of participants, 16.3% had normal BMI, 55.8% were overweight and 27.9% were obese. According to VD levels, 16.8% had VDD, 65.3% had VD insufficiency and 17.9% had normal VD level. According to HbA1c, 37.4% had good glycemic control and 16.8% had poor control and 45.8% had excellent control. All the study participants had insulin resistance of which 31.6% had early resistance.
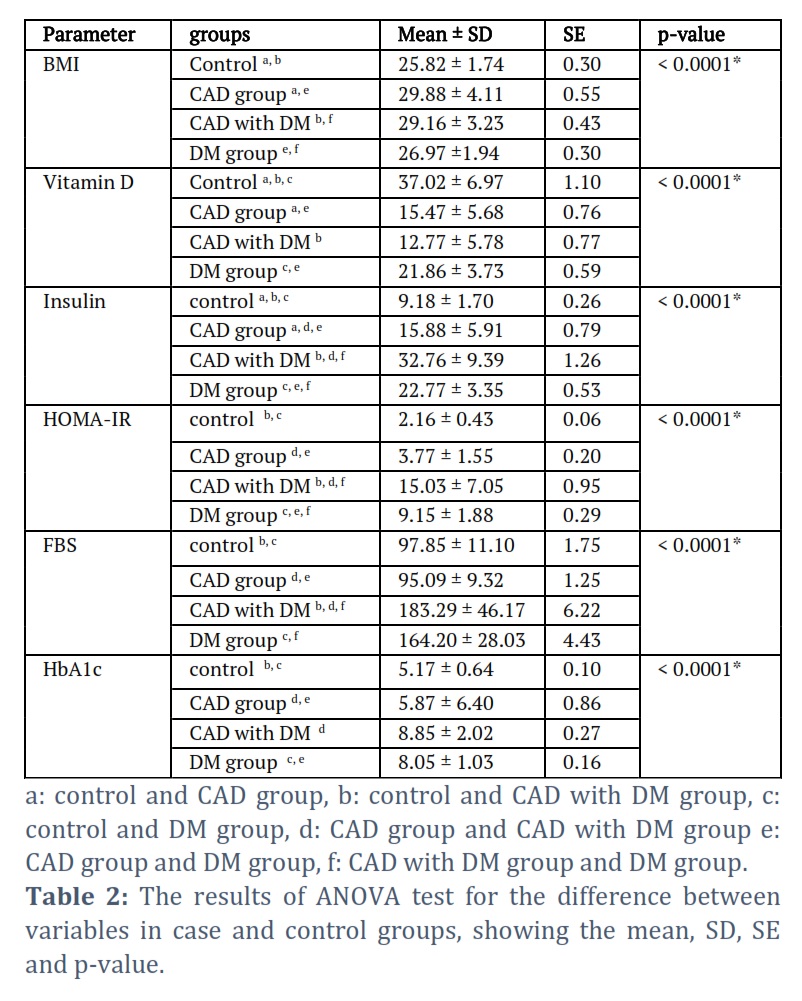
Table 2 shows the difference between the studied variables including Mean of BMI, VD levels, insulin level, HOMA-IR, FBS and HbA1c between the 4 groups. Our results showed a statistically significant difference in BMI, VD level, insulin level, HOMA-IR, FBS, and HbA1c between the studied groups p<0.0001.
Regarding BMI, Control individual had significantly lower BMI than in CAD and CAD with DM, p-value 0.00001, 0.004. CAD patients had a significantly higher BMI than DM patients, < 0.001. CAD with DM patients had a significantly higher BMI in comparison to DM patients, p-value of 0.004.
Regarding VD levels, control individual had significantly higher VD levels than CAD and CAD with DM patients, p-value < 0.001 and < 0.001. CAD patients had significantly higher VD than those in the DM group, p-value < 0.001. CAD with DM patients had a significantly higher VD in comparison to those in the DM group, 0.003. The control individual had a significantly higher VD in comparison to the other groups, < 0.001, < 0.001 and < 0.001. CAD patients had significantly lower VD levels in comparison to the DM patients, < 0.001.
The control individual had significantly lower insulin levels in comparison to the other groups, < 0.001, < 0.001 and < 0.001. CAD patients had significantly lower insulin levels in comparison to CAD with the DM and DM patients, < 0.001 and < 0.001. CAD with DM patients had a significantly higher insulin in comparison to DM patients, p-value < 0.001.
Regarding HOMA-IR, the control individual had significantly lower HOMA-IR in comparison to CAD with the DM and DM patients, < 0.001 and < 0.001. CAD patients had significant lower HOMA-IR in comparison to CAD with the DM and DM patients, < 0.001 and < 0.001. CAD with DM patients had a significantly higher HOMA-IR in comparison to DM patients, p-value < 0.001. In terms of FBG, the control group had significantly lower FBG in comparison to CAD with the DM and DM group, < 0.001 and < 0.001. CAD patients had significantly lower FBG in comparison to CAD with the DM and DM patients, < 0.001 and 0.009. CAD with DM patients had a significantly higher FBG in comparison to the DM patients, p-value < 0.001. In terms of HbA1c, the control group had significantly lower HbA1c in comparison to CAD with DM and DM group, 0.003 and < 0.001. CAD patients had significantly lower HbA1c in comparison to CAD with the DM and DM patients, 0.009 and < 0.001. CAD with DM patients had a significantly higher HbA1c in comparison to CAD patients, p-value < 0.001.
Figures & Tables
Type 2 diabetes mellitus (T2DM) represents a growing global public health concern characterized by increasing prevalence rates and considerable health burdens. Insulin resistance (IR), a pivotal aspect of T2DM, is central to its development and progression, marked by reduced responsiveness of peripheral tissues to insulin's actions, resulting in impaired glucose metabolism. Despite advances in understanding the multifactorial etiology of IR, there is ongoing interest in identifying factors that can be modified to prevent or manage it effectively [16]. VD, a fat-soluble steroid hormone, has attracted attention for its potential traditional function in bone health and calcium regulation. Recent research suggests that VD may influence glucose metabolism and IR in ways yet to be fully elucidated [17]. Observational studies have reported at a relation between VDD and increased risk of IR, T2DM, and associated complications [18]. However, the precise mechanisms driving this relationship and its clinical implications remain unclear. There is a need for further investigation into how VD level relates to IR in individuals with T2DM. This study aims to explore the association between VDD and IR in T2DM patients. From our results, CAD and CAD with DM showed a significantly elevated BMI than healthy control (p < 0.00001, p < 0.004). These findings align with prior research that has established a positive correlation between increased BMI and an elevated risk of CVD incidence. Overweight and obese patients constitute a substantial proportion of CAD patients, with individuals having a higher BMI being more prone to developing coronary artery disease [19–21]. VD levels showed a significant decline in all groups DM and CAD a well as CAD with DM compared to healthy controls (p < 0.001). These findings are supported by numerous reports that have shown a higher risk of developing diabetes in individuals with VDD [22,23]. VD can play significant roles in improving glucose metabolism and IR in DM by enhancing secretion and sensitivity of insulin, as well as mitigating inflammation in T2DM [24]. VDD has been linked to poor glycemic control and IR in patients with T2DM, as well as complications of DM [25]. Additionally, VD administration has significantly lower the incidence of T2DM and enhance the rate at which prediabetes reverts to normoglycemia [26,27]. Furthermore, recent studies coincide with our findings, revealing that increased HbA1c, fasting insulin, and HOMA-IR are associated with CAD progression in patients with T2DM [28,29], suggesting that they may have value as predictors of the severity of CAD. The results of the study indicate that low levels of vitamin D are linked to heightened insulin resistance among diabetic individuals in Baghdad, Iraq. Poorly controlled diabetes is often correlated with insufficient levels of vitamin D. Maintaining optimal vitamin D levels may effectively reduce the incidence of insulin resistance. Therefore, incorporating vitamin D screening as a routine check-up for T2DM patients is advisable.
Limitation
The small sample size was limitation point in the current study; a larger number is needed to generalize the current finding on Iraqi population.
Conflict of Interest
The authors declare that there is no conflict of interest.
M. A. A. and M. K. R. contributed to the interpretation and review of the research, checking the results and verifying the validity of what was stated in the research. A. A. I. contributed to designing the research, analyzing the results and writing this manuscript. The authors discussed the results and contributed to the final manuscript.
![]() References
References
- Li M, Chi X, Wang Y, Setrerrahmane S, Xie W i wsp. Trends in insulin resistance: insights into mechanisms and therapeutic strategy. Signal Transduction and Targeted Therapy, (2022); 7(1): 216.
- Calderón-DuPont D, Torre-Villalvazo I, Díaz-Villaseñor A. Is insulin resistance tissue-dependent and substrate-specific? The role of white adipose tissue and skeletal muscle. Biochimie, (2023); 204: 48–68.
- Rachdaoui N. Insulin: the friend and the foe in the development of type 2 diabetes mellitus. International journal of molecular sciences, (2020); 21(5): 1770.
- Albai O, Braha A, Timar B, Golu I, Timar R. Vitamin D—A New Therapeutic Target in the Management of Type 2 Diabetes Patients. Journal of Clinical Medicine, (2024); 13(5): 1390.
- Charoenngam N, Holick MF. Immunologic effects of vitamin D on human health and disease. Nutrients, (2020); 12(7): 2097.
- Pittas AG, Jorde R, Kawahara T, Dawson-Hughes B. Vitamin D Supplementation for Prevention of Type 2 Diabetes Mellitus: To D or Not to D? The Journal of Clinical Endocrinology & Metabolism, (2020); 105(12): 3721–33.
- Rafiq S, Jeppesen PB. Insulin Resistance Is Inversely Associated with the Status of Vitamin D in Both Diabetic and Non-Diabetic Populations. Nutrients, (2021); 13(6): 1742.
- Gong T, Di H, Han X, Hu X, Liu C i wsp. Vitamin D is negatively associated with triglyceride in overweight/obese patients with type 2 diabetes. Endocrine, (2022); 76(2): 304–11.
- Szymczak-Pajor I, Drzewoski J, Śliwińska A. The molecular mechanisms by which vitamin D prevents insulin resistance and associated disorders. International journal of molecular sciences, (2020); 21(18): 6644.
- Nimitphong H, Guo W, Holick MF, Fried SK, Lee M. Vitamin D Inhibits Adipokine Production and Inflammatory Signaling Through the Vitamin D Receptor in Human Adipocytes. Obesity, (2021); 29(3): 562–8.
- Musa IR, Omar SM, Sharif ME, Ahmed ABA, Adam I. The calculated versus the measured glycosylated haemoglobin (HbA 1c ) levels in patients with type 2 diabetes mellitus. Journal of Clinical Laboratory Analysis, (2021); 35(8): 129–32.
- Ahmed SS, Ghareeb A-W El, El-Nahas T, Sobhy M, Hassan EA i wsp. The Effect of Vitamin D Deficiency on the Frozen-Thawed Embryo Transfer Outcome. The Egyptian Journal of Hospital Medicine, (2024); 94(1): 725–32.
- Afarid M, Ghattavi N, Karim Johari M. Serum Levels of Vitamin D in Diabetic Patients With and Without Retinopathy. Journal of Ophthalmic and Vision Research, (2020); 15(2): 172–177.
- Lee H, Ha TY, Jung CH, Nirmala FS, Park S i wsp. Mitochondrial dysfunction in skeletal muscle contributes to the development of acute insulin resistance in mice. Journal of Cachexia, Sarcopenia and Muscle, (2021); 12(6): 1925–39.
- Borg DN, Barnett AG, Caldwell AR, White NM, Stewart IB. The bias for statistical significance in sport and exercise medicine. Journal of Science and Medicine in Sport, (2023); 26(3): 164–8.
- Al-Janabi AHA, Abdulzahra MA, Jaafar SS, Hussein TS, Al-Mawlah YH. Chromium status and insulin resistance as the risk factors of ischemic heart disease in Type 2 Diabetes Mellitus patients. Journal of Biotech Research, (2023); 15: 24–30.
- Wu J, Atkins A, Downes M, Wei Z. Vitamin D in diabetes: uncovering the sunshine hormone’s role in glucose metabolism and beyond. Nutrients, (2023); 15(8): 1997.
- Sun L-J, Lu J-X, Li X-Y, Zheng T-S, Zhan X-R. Effects of vitamin D supplementation on glucose and lipid metabolism in patients with type 2 diabetes mellitus and risk factors for insulin resistance. World Journal of Diabetes, (2023); 14(10): 1514–23.
- Zhao Y, Qie R, Han M, Huang S, Wu X i wsp. Association of BMI with cardiovascular disease incidence and mortality in patients with type 2 diabetes mellitus: A systematic review and dose–response meta-analysis of cohort studies. Nutrition, Metabolism and Cardiovascular Diseases, (2021); 31(7): 1976–84.
- Buschmann K, Wrobel J, Chaban R, Rösch R, Ghazy A i wsp. Body Mass Index (BMI) and Its Influence on the Cardiovascular and Operative Risk Profile in Coronary Artery Bypass Grafting Patients: Impact of Inflammation and Leptin. Oxidative Medicine and Cellular Longevity, (2020); 2020: 1–9.
- Eid O, Eid R, Styliou T, Diakonikolaou S, Christou V i wsp. Prevalence and impact of high BMI in CAD patients. European Journal of Preventive Cardiology, (2022); 29(1): 56–79.
- Charoenngam N, Holick MF. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients, (2020); 12(7): 2097.
- Abugoukh TM, Sharaby A Al, Elshaikh AO, Joda M, Madni A i wsp. Does Vitamin D Have a Role in Diabetes? Cureus, (2022); 14(10): e30432.
- Wardani IS, Aliza Raudatin Sahly, Indana Eva Ajmala, Dewi Suryani. Vitamin D and Type 2 Diabetes Mellitus: Role in Insulin Resistance, Glycemic Control and Long Term Complications. Unram Medical Journal, (2022); 11(2): 942–52.
- Farahmand MA, Daneshzad E, Fung TT, Zahidi F, Muhammadi M i wsp. What is the impact of vitamin D supplementation on glycemic control in people with type-2 diabetes: a systematic review and meta-analysis of randomized controlled trails. BMC Endocrine Disorders, (2023); 23(1): 15.
- Zhang Y, Tan H, Tang J, Li J, Chong W i wsp. Effects of Vitamin D Supplementation on Prevention of Type 2 Diabetes in Patients With Prediabetes: A Systematic Review and Meta-analysis. Diabetes Care, (2020); 43(7): 1650–8.
- Barbarawi M, Zayed Y, Barbarawi O, Bala A, Alabdouh A i wsp. Effect of Vitamin D Supplementation on the Incidence of Diabetes Mellitus. The Journal of Clinical Endocrinology & Metabolism, (2020); 105(8): 2857–68.
- Tanaka T, Kishi S, Ninomiya K, Ishizawa T, Kikushima H i wsp. Clinical Predictors of Coronary Artery Plaque Progression by Quantitative Serial Assessment Using 320-Row Computed Tomography Coronary Angiography in Asymptomatic Patients with Type 2 Diabetes Mellitus. Journal of Cardiology, (2020); 76(4): 378–84.
- Yaseen RI, Beda MY, Ibrahim FA. Correlation between Severity of Coronary Artery Disease and Insulin Resistance in Diabetic Patients. The Egyptian Journal of Hospital Medicine, (2021); 84(1): 2084–9.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


