

Full Length Research Article
Scrutiny of immunological components (CD20, CD30, and CD40) and HCMV and EBV infections in lymphoma Iraqi patients
Ahmed Talib Ghadhban1, Marwa Mohammed Ali Jassim1, Majid Mohammed Mahmood2*, Hayder Saad Hanfoosh Al Atabi1, Sameem Atia Rekan3
Adv. life sci., vol. 11, no. 1, pp. 61-65, February 2024
*- Corresponding Author: Majid M. Mahmood (majidmahmood93@yahoo.com)
Authors' Affiliations
2. Department of Biology, College of Science, Mustansiriyah University, Baghdad – Iraq
3. Pediatric and gynecology hospital Al Muthana Health Directorate – Iraq
[Date Received: 25/07/2022; Date Revised: 08/12/2023; Date Published: 25/02/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: This investigation concentrated on Hodgkin and non-Hodgkin lymphomas in the Iraqi province of Al-Muthanna. Environmental and immune characteristics have a role in this malignancy. In an attempt to assess Hodgkin and non-Hodgkin lymphomas in Iraqi patients, in addition to the detection of specific immunological and virological data, 30 patients and 10 controls were scrutinized.
Methods: Forty subjects with an age range of 20–82 years, 30 with lymphomas (Hodgkin and non-Hodgkin), and 10 with no lymphomas were analyzed. The tissue blocks were tested for EBER-EBV and PP65-CMV viruses using the in-situ hybridization (ISH) technique with the aid of kits of specific probes for viruses. Also, immunological markers such as CD markers were investigated using immunohistochemistry (IHC).
Results: In the Iraqi Al-Muthanna governorate Lymphoma cases rose notably among people beyond sixty. Hodgkin lymphoma cases were found more often than non-Hodgkin lymphoma cases, with a predominance of females in both types. The results of HCMV and EBV detection illustrated a higher prevalence of these viruses, especially in patients with non-Hodgkin lymphoma, accompanied by related immunological changes in lymphoma patients than in the lymphoma-free group.
Conclusions: In Al-Muthanna province, Hodgkin and non-Hodgkin lymphomas were slightly increased in females, along with more prevalent HCMV and EBV infections.
Keywords: HL-NHL lymphoma; Human cytomegalovirus; Epstein-Barr virus
Introduction![]()
Hodgkin lymphoma is classified as either classical Hodgkin lymphoma or nodular lymphocyte-predominant Hodgkin lymphoma [1]. It was responsible for 0.2% to 0.4% of all cancer cases and fatalities worldwide in 2020 [2]. Although uncommon, it is the most prevalent cancer among teenagers aged 15 to 19 [3, 4]. Hodgkin cancer affects people differently depending on their gender, age, sex, and where they live. Hodgkin lymphoma is more likely to happen to men [5], teenagers and young adults [6], people with a history of Epstein-Barr virus infection, HIV/AIDS, inflammatory diseases, exposure to pollution, smoking cigarettes, and people with it in their family tree. Recently antibody treatment has improved Hodgkin lymphoma survival. Vaccines, checkpoint inhibitors, and cytotoxic T cells are potential therapy [7-9]. Non-Hodgkin lymphoma is a kind of cancer that arises in the lymphatic artery and duct network. The lymphatic system is part of the immune system. Lymph is a clear fluid that circulates through the lymphatic system and includes white blood cells known as lymphocytes, which fight infections. Non-Hodgkin lymphoma tends to congregate in lymph nodes (glands) after abnormal cell growth [10]. Injured lymphocytes become less effective in fighting infection, leaving you more susceptible to illness. A non-painful lymph node enlargement often identifies non-Hodgkin lymphoma; these lymph nodes are often located in the neck, armpit, or groin. Multiple forms of NHL can be classified as either slow- or fast-growing [11].
B lymphocytes (B cells) create antibodies to help fight infections, while natural killer (NK) cells destroy cells infected with viruses or cancer cells. Lymphocytes (L cells) and other T lymphocytes (NK cells) can serve as the primary site of lymphoma formation. However, approximately 85–90% of NHL cases originate in B cells. These lymphoma cells accumulate and form masses (tumors) [12]. Untreated NHL results in a compromised immune system because malignant cells crowd out healthy white blood cells [13].
Primary extranodal lymphoma is NHL that develops or spreads to other lymphoid-containing body regions, such as the spleen, digestive system, and bone marrow. The NHL is divided into over sixty subgroups [14]. The jaw, brain, intestines, kidneys, ovaries, and maybe other organs could be impacted by this illness. The CNS is a potential spread site for Burkitt lymphoma. An essential finding for diagnosing Burkitt lymphoma is the translocation (a rearrangement) of a gene called MYC [15]. The aggressive B-cell lymphoma known as diffuse large B-cell lymphoma (DLBCL) is sometimes indistinguishable from Burkitt lymphoma in adults. It arises because of an increase in defective B lymphocytes [16]. Burkitt lymphoma may be divided into three distinct subtypes. These classifications are based on the disease’s origin and prevalence worldwide. The most frequent kind of Burkitt lymphoma in the UK is sporadic Burkitt lymphoma. It is associated with the Epstein-Barr virus (EBV) [17]. Burkitt lymphoma is more common in African children, while HIV-related Burkitt lymphoma can develop in organ transplant recipients [18, 19]. A study implies a relationship between malaria and EBV; this form is uncommon in the UK; Burkitt lymphoma develops rapidly, and therapy begins immediately after diagnosis [20].
Methods![]()
A total of 40 people with age range between 20–82 years participated in this study (30 samples of lymphoma patients, 18 with Hodgkin and 12 non-Hodgkin lymphoma patients according to clinical diagnosis). In addition, 10 samples of control subjects among those who were negative for lymphoma. Immunohistochemistry kits (Abcam/UK) for detecting immunological markers (CD20, CD30, CD40) for diagnostic purposes and following the manufacturer's instructions. In situ hybridization kits (Abcam/UK) with probes specific for HCMV and EBV, were used. These tests were performed following the manufacturer's instructions.
Ethical Approval
Consent was obtained to collect samples from all patients. Additionally, this study obtained approval from the scientific committee at the site of the study (Iraqi Ministry of Health/Al Muthana Health Directorate/Al-Hussein Teaching Hospital) on November 24, 2022.
Statistical Analysis
The Chi-Square test determines the relationship between variables and percentages. Statistical significance, on the other hand, was evaluated at p < 0.05 and p < 0.01. Our data was collected and analyzed using SPSS 26.0, the Statistical Package for the Social Sciences.
Results![]()
Distribution of data according to the gender of study groups
In Hodgkin lymphoma, there were 11 females and 7 males, in non-Hodgkin lymphoma, there were 8 females and 4 males., while the control group composed of 5 males and 5 female.
Distribution of data according to age of study groups
The age distribution of the study groups was classified as 20–40, 40–60, 60–80, ˃80. However, the predominance of lymphoma in both types was in the 60–80 age group, whereas the lowest distribution of lymphoma was in ˃80 age group.
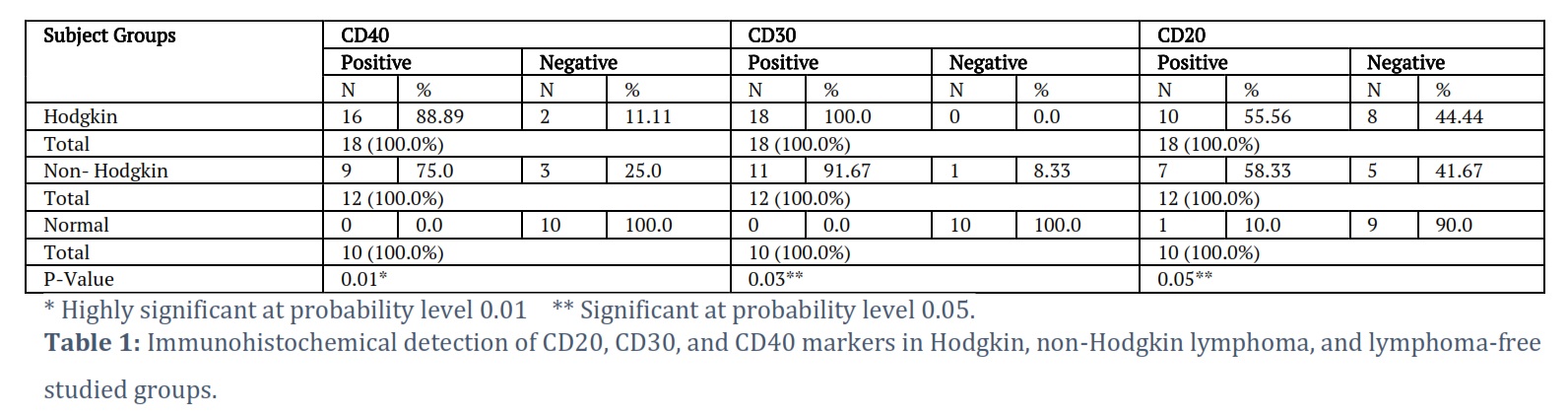
Immunological detection of CD markers in Hodgkin, No-Hodgkin Lymphoma, and Lymphoma free studied groups
The results of immunological markers are illustrated in Table 1. The number of positive results and percentages of CD40 were [16 (88.89%), 9 (75.0%), 0 (0.0%)] in Hodgkin, non-Hodgkin, and lymphoma free groups, respectively. The number of positive results and percentages of CD30 in Hodgkin, non-Hodgkin, and lymphoma free groups, were [18 (100.0%), 11 (91.67%), 0 (0.0%)] respectively. While the number of positive results and percentages of CD20 were as follows: 10 (56%) in Hodgkin, 7 (58.33) in non-Hodgkin, and 1 (10%) in lymphoma free groups. However, the studied groups have highly significant differences at p-level 0.01 in CD40. In addition, there are significant differences at the p-level (0.03 and 0.05) in regard to CD30 and CD20, respectively. This may reflect the importance of immune cells carrying those markers in such tumors, according to the situation, each by itself.
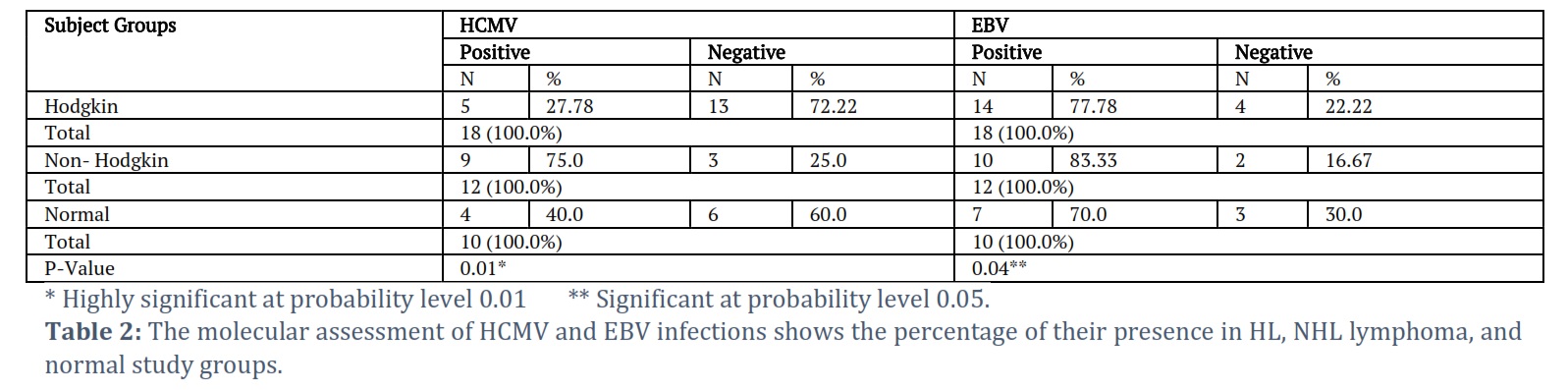
The molecular assessment of viral infection in Hodgkin, Non-Hodgkin lymphoma, and lymphoma free studied groups
Table 2 shows the molecular detection of viral infection in the study groups. The percentage of HCMV-positive sections was the highest (75.0%) in non-Hodgkin lymphoma, while the percentage in Hodgkin lymphoma was the lowest (27.78%), as positive sections were found in 40.0% of lymphoma-free individuals.
Similarly, the highest percentage of EBER-EBV positive detections (83.33%) were also recorded in non-Hodgkin lymphoma, while a slightly lower percentage of positive detections were recorded in the Hodgkin lymphoma group (77.78%), followed by 70.0 percent in lymphoma-free subjects. There are highly significant differences at the p-level of (0.01) regarding HCMV infection. Likewise, there are significant differences at a p-value of (0.04) for EBV infection among the studied groups.
Figures & Tables
In-situ hybridization for EBER is commonly employed to assess cancer's EBV status in various types including lymphoid cancers. The capacity of the common herpes virus EBV to hide out in dormant form among B-lymphocytes gives it a distinct advantage over the host immune system. Cellular immunity deficiencies, such as those induced by concurrent infections, old age, and immunosuppressive conditions, greatly increase the likelihood of EBV reactivation and B-cell transformation. In the current scrutiny, we validated that EBV genes were present in neoplastic cells of lymphoma patients, as it was reported by Li et al. (1995) and Mundo et al. (2020) [21, 22]. As a result, and in contrast to the study by Shahriari-Ahmadi et al., which found no evidence of EBV infection in NHL patients, we warned that EBV may have a role in lymphomagenesis.
In respect to CMV infection (CMVI) and in retrospective research done by Sato et al. (2022), it was shown that 5.5% of the included patients with malignant lymphoma who had undergone chemotherapy or radiation experienced infection with CMV [23]. Furthermore, they showed that CMVI may lead to poor survival [24]. In another investigation accomplished by Mehravaran et al., they found that 20% of non-Hodgkin's lymphoma patients expressed UL 138, suggesting that latent CMV infection may contribute to disease development [25].
Human cytomegalovirus produces the protein pp65, which has been implicated in several significant events in tumor progression [26, 27]. Most virion proteins and non-infectious viral particles are Pp65 during active infection. 76% of 29 central nervous system diffuse large B-cell lymphoma biopsies had HCMV pp65 [28]. Consequently, patients with aggressive non-Hodgkin lymphoma, Hodgkin lymphoma, and follicular non-Hodgkin lymphoma all had significant frequencies of HCMV pp65 antigenemia (57%, 49%, and 44%, respectively) [29]. Despite this and despite what has been mentioned about the EBV, which reported to be associated with non-Hodgkin’s lymphoma [30], the outcome is not complete for the viruses with the presence of antiviral immune activities that do not allow them to do uncontrollably.
In the Iraqi province of Al-Muthanna Hodgkin lymphoma grew, notably among women. There is a higher prevalence of viral infections (HCMV and EBV) in the tissues of non-Hodgkin lymphoma patients, in spite of the greater frequencies of exhibiting positive immunological CD marker signs. Due to the relatively high expression rate for pp65 in lymphoma patients, particularly non-Hodgkin lymphoma, latent CMV infection may have a role in the development of the illness. In this regard, the data from this study are an essential reference parameter for evaluating and monitoring the progress of national initiatives for surveillance programs and clinical management enhancements designed to reduce the incidence of lymphoma in Iraq.
Conflict of Interest
The authors declare that there is no conflict of interest.
Acknowledgement
This research project was supported by the College of Science / Mustansiriyah University; authors thank the Deanship of college of science for their technical support.
Conceptualization: Ahmed Talib Ghadhban, Marwa Mohammed Ali Jassim, Majid Mohammed Mahmood, Hayder Saad Hanfoosh Al atabi, Sameem Atia Rekan
Data Curation: Ahmed Talib Ghadhban, Marwa Mohammed Ali Jassim, Majid Mohammed Mahmood, Hayder Saad hanfoosh Al atabi, Sameem Atia Rekan
Formal Analysis: Marwa Mohammed Ali Jassim, Majid Mohammed Mahmood, Ahmed Talib Ghadhban, Sameem Atia Rekan, Hayder Saad hanfoosh Al atabi
Funding Acquisition: Majid Mohammed Mahmood, Ahmed Talib Ghadhban, Marwa Mohammed Ali Jassim, Hayder Saad hanfoosh Al Atabi, Sameem Atia Rekan
Investigation: Hayder Saad Hanfoosh Al Atabi, Sameem Atia Rekan, Majid Mohammed Mahmood, Ahmed Talib Ghadhban, Marwa Mohammed Ali Jassim
Methodology: Majid Mohammed Mahmood, Ahmed Talib Ghadhban, Marwa Mohammed Ali Jassim, Hayder Saad Hanfoosh Al Atabi, Sameem Atia Rekan
Project Administration: Marwa Mohammed Ali Jassim, Majid Mohammed Mahmood, Ahmed Talib Ghadhban, Sameem Atia Rekan, Hayder Saad hanfoosh Al Atabi
Resources: Ahmed Talib Ghadhban, Marwa Mohammed Ali Jassim, Majid Mohammed Mahmood, Hayder Saad Hanfoosh Al Atabi, Sameem Atia Rekan
Software: Marwa Mohammed Ali Jassim, Majid Mohammed Mahmood, Ahmed Talib Ghadhban, Sameem Atia Rekan, Hayder Saad hanfoosh Al Atabi
Supervision: Majid Mohammed Mahmood, Ahmed Talib Ghadhban, Marwa Mohammed Ali Jassim, Hayder Saad Hanfoosh Al Atabi, Sameem Atia Rekan
Validation: Majid Mohammed Mahmood, Ahmed Talib Ghadhban, Marwa Mohammed Ali Jassim, Hayder Saad Hanfoosh Al Atabi, Sameem Atia Rekan
Writing: Original Draft Preparation: Marwa Mohammed Ali Jassim, Majid Mohammed Mahmood, Ahmed Talib Ghadhban, Sameem Atia Rekan, Hayder Saad hanfoosh Al atabi
Review & Editing: Ahmed Talib Ghadhban, Marwa Mohammed Ali Jassim, Hayder Saad Hanfoosh Al atabi, Majid Mohammed Mahmood, Sameem Atia Reka
![]() References
References
- Huang J, Pang WS, Lok V, Zhang L, Lucero-Prisno III DE, XuW, and NCD Global Health Research Group, Association of Pacific Rim Universities (APRU). Incidence, mortality, risk factors, and trends for Hodgkin lymphoma: a global data analysis. Journal of Hematology & Oncology, (2022);15(1): 57.
- Smith CM, Friedman DL. Advances in Hodgkin Lymphoma: Including the Patient's Voice. Frontiers in Oncology, (2022); 855725.
- Stephens DM, Li H, Schöder H, Straus DJ, Moskowitz CH, LeBlanc M, and Friedberg JW. Five-year follow-up of SWOG S0816: limitations and values of a PET-adapted approach with stage III/IV Hodgkin lymphoma. Blood. The Journal of the American Society of Hematology, (2019); 134(15):1238-1246.
- Mauz-Körholz C, Landman-Parker J, Balwierz W, Ammann RA, Anderson RA, et al. Response-adapted omission of radiotherapy and comparison of consolidation chemotherapy in children and adolescents with intermediate-stage and advanced-stage classical Hodgkin lymphoma (EuroNet-PHL-C1): a titration study with an open-label, embedded, multinational, non-inferiority, randomised controlled trial. The lancet oncology, (2022); 23(1): 125-137.
- Quintana MDP, Smith‐Togobo C, Moormann A, and Hviid L. Endemic Burkitt lymphoma–an aggressive childhood cancer linked to Plasmodium falciparum exposure, but not to exposure to other malaria parasites. Apmis, (2020); 128(2): 129-135.
- Cole PD, McCarten KM, Pei Q, Spira M, Metzger ML et al. Brentuximab vedotin with gemcitabine for paediatric and young adult patients with relapsed or refractory Hodgkin's lymphoma (AHOD1221): a Children's Oncology Group, multicentre single-arm, phase 1–2 trial. The Lancet Oncology, (2018); 19(9): 1229-1238.
- Broccoli A, Argnani L, Botto B, Corradini P, Pinto A, and Re A. First salvage treatment with bendamustine and brentuximab vedotin in Hodgkin lymphoma: a phase 2 study of the Fondazione Italiana Linfomi. Blood Cancer Journal, (2019); 9(12): 100.
- Society A C. American Cancer Society. Cancer Facts & Figures 2020. Am Cancer Soc, (2020); 1-52.
- Flerlage JE, Metzger ML, Bhakta N. The management of Hodgkin lymphoma in adolescents and young adults: burden of disease or burden of choice? Blood. The Journal of the American Society of Hematology, (2018); 132(4): 376-384.
- Derebas J, Panuciak K, Margas M, Zawitkowska J, and Lejman M. The new treatment methods for non-hodgkin lymphoma in pediatric patients. Cancers, (2022); 14(6): 1569.
- Jassim MM, Naji SA, Mahmood MM. BRCA1, BCL2, and the RB Tumor Suppressor have abnormal expressions in lung cancer. Research Journal of Pharmacy and Technology, (2022); 15(9): 4083-4087.
- Jacobsen E. Follicular lymphoma:2023 update on diagnosis and management. American Journal of Hematology, (2022); 97(12):1638-1651.
- Chin L, Wong CY, Gill H. Targeting and Monitoring Acute Myeloid Leukaemia with Nucleophosmin-1 (NPM1) Mutation. International Journal of Molecular Sciences, (2023); 24(4): 3161.
- Amhaz G, Bazarbachi A, and El-Cheikh J. Immunotherapy in indolent Non-Hodgkin's Lymphoma. Leukemia Research Reports, (2022); 17: 100325.
- Shafie M, Shahmohamadi E, Ghasemi H, Zarei Jalalabadi N, and Parsa S. Burkitt lymphoma presenting as cecum mass and spontaneous tumor lysis syndrome with hypercalcemia. Clinical Case Reports, (2023); 11(2): 6977.
- Flegel K. Burkitt’s Lymphoma: The Discovery and Diagnosis of a New Illness. Canadian Journal of General Internal Medicine, (2023);18(1): 1-8.
- Ricard F, Cheson B, Barrington S, Trotman J, Schmid A, Brueggenwerth G, and Korn R. Application of the Lugano Classification for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The PRoLoG Consensus Initiative (Part 1—Clinical). Journal of Nuclear Medicine, (2023);64(1): 102-108.
- Zhao X, Ma Y, Bian H, and Liu Z. CD20 expression is closely associated with Epstein–Barr virus infection and an inferior survival in nodular sclerosis classical Hodgkin lymphoma. Frontiers in Oncology, (2022); 4717.
- Vaccher E, Gloghini A, Volpi C C, & Carbone A. Lymphomas in People Living with HIV. Hemato, (2022); 3(3): 527-542.
- Jassim MM, Mahmood MM, & Musa SQ. Herpetic Oncogenic Virus Co-Infections Impinge Cell Cycle Regulatory Gene Expressions in Oral Cavity Malignancies. Systematic Reviews in Pharmacy, (2020);11(3):
- Mundo L, Del Porro L, Granai M, Siciliano M C, Mancini V, et al. Frequent traces of EBV infection in Hodgkin and non-Hodgkin lymphomas classified as EBV-negative by routine methods: expanding the landscape of EBV-related lymphomas. Modern Pathology, (2020); 33(12): 2407-2421.
- Li D, Oda K, Mikata A, and Yumoto N. Epstein‐Barr virus genomes in Hodgkin's disease and non-Hodgkin's lymphomas. Pathology international, (1995); 45(10): 735-741.
- Jassim MM, Mahmood MM, Ali SH, and Kamal MS. Interplay between EBERS and P27 tumor suppressor proteins in molecular transformation of nasopharyngeal and sinonasal carcinomas. Indian Journal of Public Health, (2019); 10(6): 19.
- Sato K, Igarashi S, Tsukada N, Inamura J, Yamamoto M, et al. Cytomegalovirus infection in patients with malignant lymphomas who have not received hematopoietic stem cell transplantation. BMC cancer, (2022); 22(1): 944.
- Mehravaran H, Makvandi M, Zade AS, Neisi N, Kiani H, et al. Association of human cytomegalovirus with Hodgkin’s disease and non-Hodgkin’s lymphomas. Asian Pacific Journal of Cancer Prevention, (2017); 18(3): 593.
- Ponticelli C. Herpes viruses and tumours in kidney transplant recipients. The role of immunosuppression. Nephrology Dialysis Transplantation, (2011); 26(6): 1769-1775.
- Cai ZZ, Xu JG, Zhou YH, Zheng JH, Lin KZ, et al. Human cytomegalovirus-encoded US28 may act as a tumor promoter in colorectal cancer.World Journal of Gastroenterology, (2016); 22(9):2789.
- Libard S, Popova SN, Amini RM, Kärjä V, Pietiläinen T, Hämäläinen KM, and Alafuzoff I. Human cytomegalovirus tegument protein pp65 is detected in all intra-and extra-axial brain tumours independent of the tumour type or grade. PloS one, (2014); 9(9): e108861.
- Mariotti J, Maura F, Spina F, Roncari L, Dodero A, et al. Impact of cytomegalovirus replication and cytomegalovirus serostatus on the outcome of patients with B cell lymphoma after allogeneic stem cell transplantation, Biology of Blood and Marrow Transplantation, (2014); 20(6): 885-890.
- Economides MP, Mahale P, Turturro F, Hosry J, Samaniego F, et al. Development of non-Hodgkin lymphoma as a second primary cancer in hepatitis C virus-infected patients with a different primary malignancy. Leukemia & Lymphoma, (2017); 58(2): 485-488.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


