

Full Length Research Article
Serum Levels of 25-OH Vitamin D3 and Vitamin D Receptor among Iraqi Children with Autism Spectrum Disorder
Riyam Abbas Kadhim1*, Rayah Salman Baban1, Areej Abdul Abass Al- Omrani2, Khaldoon Hussain Alhafidh3
Adv. life sci., vol. 11, no. 1, pp. 233-236, February 2024
*- Corresponding Author: Riyam Abbas Kadhim (areiyam@yahoo.com)
Authors' Affiliations
2. Professor of Pediatrics/ CABP /Al- Nahrain University / College of Medicine/Pediatric department – Iraq
3. A Consultant Pediatrician/ M.B.Ch.B, DCH, MSc in Epileptology and MRCPCH , London – United Kingdom
[Date Received: 20/07/2023; Date Revised: 23/12/2023; Date Published: 25/02/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Autism spectrum disorders are a neurodevelopmental disorder characterized by some degree of difficulty with social interaction and communication. It is regarded as a developmental disorder because the symptoms typically occur in the first three years of life.
Method: A total of forty-four (ASD children) and forty-four (controls) were enrolled in this study with the age range of 2 – 11 years old. 25-OH Vitamin D3 and Human Vitamin D receptor measured from serum samples by Enzyme Linked Immunosorbent Assay (ELISA).
Result: 25-OH vitamin D3 and Vitamin D Receptor were significantly lower in ASD patients’ group than in control group. There is no significant correlation between 25 OH Vitamin D3 and VDR .The ROC analysis revealed that 25OHVD3 exhibited the highest diagnostic accuracy with sensitivity (100%) and specificity (100%). In comparison, the Vitamin D Receptor exhibited a lower diagnostic accuracy with an AUC of 0.888 , sensitivity ( 95.45%) and specificity only (63.64%).
Conclusion :The concentration of 25OHvitamin D3 was significantly lower in ASD group which means that it can be used as a marker in the early stages of autism spectrum disorder. In contrast , the vitamin D receptor may not be as effective a marker in differentiating ASD cases from controls.
Keywords: Autism Spectrum Disorder; 25-OH Vitamin D3; Vitamin D Receptor
Introduction![]()
Autism spectrum disorders (ASD) are a brain developmental turmoil with a predestined 2 % prevalence[1]. Genetic, neurological, immunological, idiopathic, and postnatal factors may be important contributors to the etiology of ASD [2]. The first three years of this disorder’s onset are distinguished by a decline in interactions and contact in childhood [3]. Its neurobiology is thought to be influenced by neurochemical and genetic factors [4].Numerous studies have demonstrated the involvement of vitamin D in numerous neuronal processes as well as brain development. Also, Vitamin D insufficiency during pregnancy or infancy has been associated as a developmental risk factor for ASD [5].Vitamin D exhibits its efficacy through its binding to VDR in a variety of tissues including the brain and peripheral neurons. The vitamin D receptor is a member of the nuclear receptor family of transcription factors bound to vitamin D , which then forms VDR a heterodimer [6]. Alternatively, low serum levels of vitamin D Receptor and 25-OH Vitamin D3 have been shown in ASD children [7,8,9,10]. However, the linkage between psychiatric disorders and low vitamin D3 and VDR among ASD has been recognized [6,10].
Methods![]()
A case-control study was conducted on a group of 88 children. 44 had autism spectrum disorder and 44 were controls. The study was carried out from May 2022 to March 2023, with participants ranging in age from 2 to 11 years. Healthy controls and patients were chosen from the private clinic and AL- Kadhimiya Educational Hospital . Each patient's medical history, clinical and biochemical characteristics and the socio-demographic including their age and location were recorded. ASD was diagnosed in all of the patients according to childhood autism rating scale criteria (CARS ).
The human 25-Hydroxy Vitamin D3 kit (BT LAB , China, Cat. No E1981Hu)and Human Vitamin D receptor ELISA kit (BT LAB , China, Cat. No E1553Hu) were used to measure25OHVD3 and VDR levels by sandwich ELISA technique .
Ethical approval : ethical approval was obtained with the approval of the Research Ethical Committee from the Ministry of Higher Education and Scientific Research / Al-Nahrain University / College of Medicine / Baghdad, in conjunction with the Ministry of Health / Al-Kadhimiya Educational Hospital in Iraq (According to the decision for research ethics approval with No: 2022144 in 27/12/2023)(IRP/79). Approval of the children's families were taken too.
Blood sample collection and preservation
Disposable syringes and vein punctures were used to collect 2 ml of blood. The serum was obtained by collecting the blood in a tube and leaving the sample at room temperature. Then, the sample centrifuged at 3000 rpm after allowing the blood to clot for 15 min. All measurement of serum 25 OH Vitamin D3 and VDR levels were done by the Sandwich ELISA technique.
Exclusion criteria
Children aged > 11 years, liver diseases, renal diseases, attention deficit/ Hyperactivity disorder ADHD, Mental retardation and Case of diabetes were not allowed to participate in the study.
Statistical analysis
A two-tailed Mann- Whitney U test was used to assess the distribution of 25OHVD3 and VDR across ASD and Control groups. The Receiver Operating Characteristic (ROC) analysis was conducted to evaluate the performance of selected markers in distinguishing individuals with Autism Spectrum Disorder (ASD) from controls. P-values < 0.05 were regarded as significant.
Results![]()
The level of serum 25-OH Vitamin D3 in healthy control and ASD groups
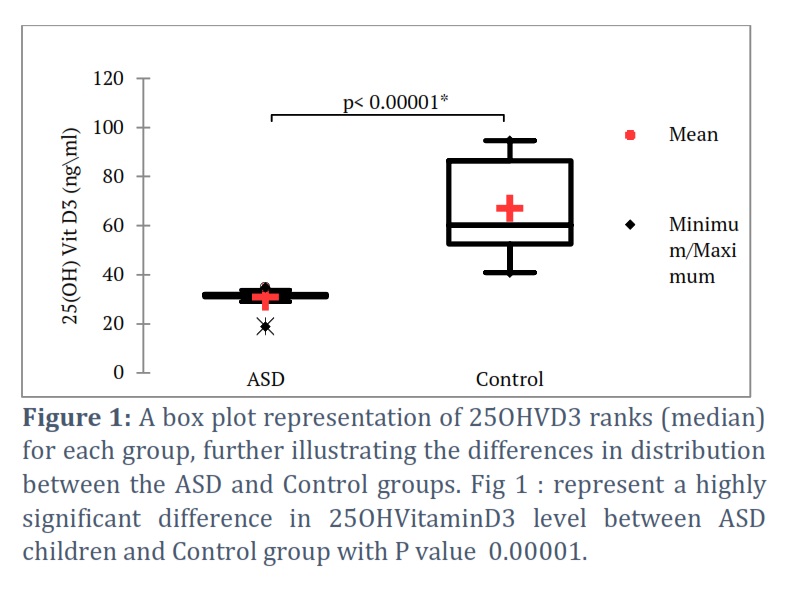
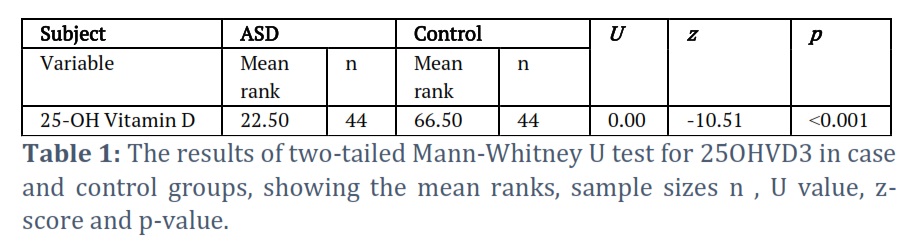
In Table (1) and Figure (1) the ASD group exhibited a mean rank of 22.50, while the Control group presented a mean rank of 66.50. The median 25OH Vitamin D3 level in the ASD group (Mdn = 31.55) was significantly lower compared to the Control group's median level (Mdn = 60.16).
The level of serum Vitamin D Receptor in healthy control and ASD groups
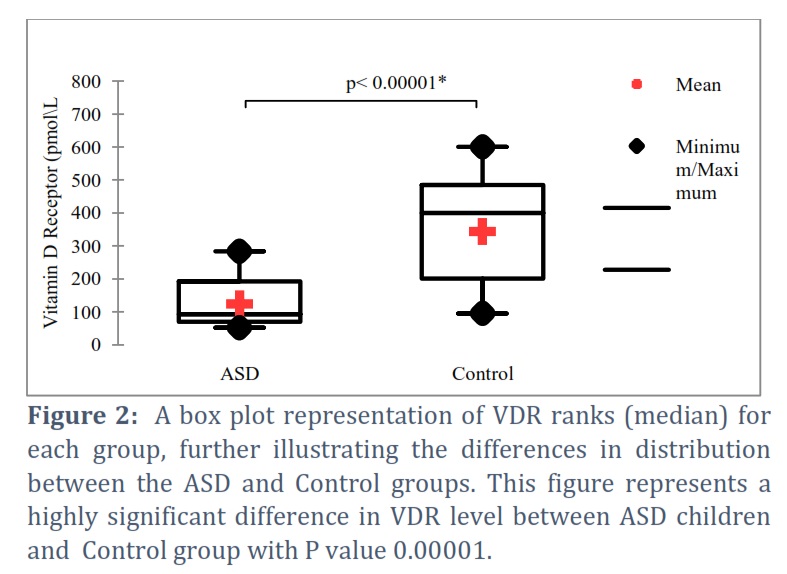
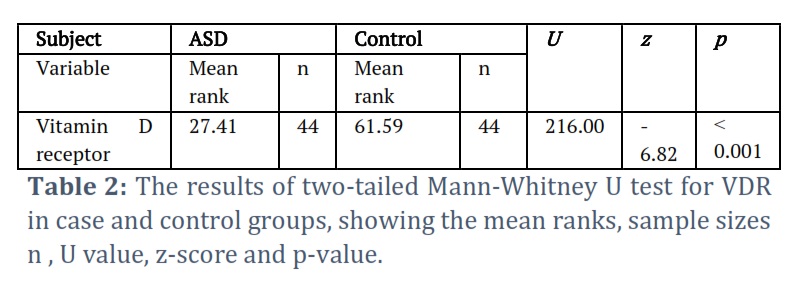
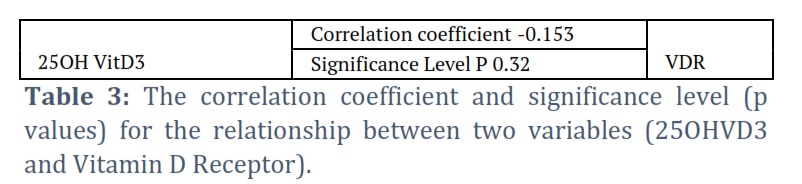
In Table 2 and Figure 2 the ASD group had a mean rank = 27.41 while, the Control group had a mean rank = 61.59. Furthermore, the median Vitamin D receptor level in the ASD group (Mdn = 92.75)was statistically lower compared to the Control group's median VDR level (Mdn = 400.35). There was no significant correlation between 25-OH VD3 and VDR.
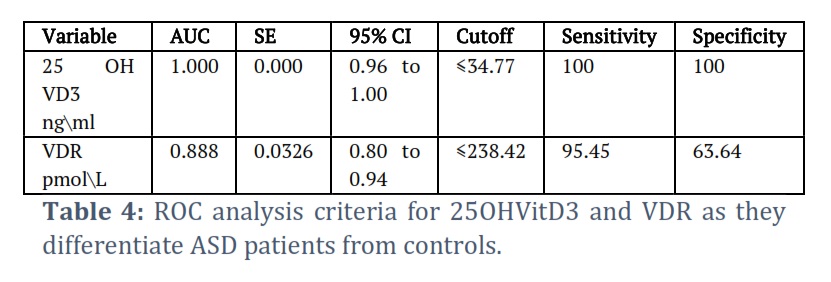
ROC analysis criteria for 25-OH Vit. D3 and VDR
The ROC analysis reveals that 25 OH VD3 exhibits the highest diagnostic accuracy, with a perfect AUC of 1.000, sensitivity (100%) and specificity (100%). VDR exhibits a lower diagnostic accuracy with an AUC of (0.888), sensitivity of 95.45% and specificity 63.64%. VDR may not be as effective in differentiating ASD cases from controls.
Figures & Tables
Due to its growing prevalence over time, ASD is regarded as a major clinical problem as a neurodevelopmental condition. Finding the main cause of ASD may hold promise for its prevention and/or treatment. Vitamin D deficiency has recently been considered an environmental aspect in the etiology of autism, in addition to genetic ones. In this study , all Iraqi autistic participants had 25OH vitamin D3 deficiency . Additionally, the serum 25OHVD3 level (which is a measurable indicator of vitamin D) was statistically lower in ASD children than in healthy controls with sensitivity (100%) and specificity (100%). In similar manner, the recent research revealed that children with ASD had a lower 25OH vitamin D3 levels than their peers [11]. In ASD children, the level of VDR was significantly lower compared to control group with sensitivity of 95.45% and specificity 63.64% . This result confirms previous studies that showed VDR to be decrease in ASD [10]. Furthermore, this result supports previous research that showed a decrease level of 25OH vitamin D3 and VDR in ASD [7,8,9,11,12].
Children with ASD become less exposed to sunlight because of the low levels of physical activity and sedentary behaviors . Furthermore , the restricted dietary behavior may lead to vitamin D deficiency [13]. In several ways, a lower level of vitamin D observed in the pathogenesis from ASD has been shown to be both an organ-specific and pathological disorder like de-novo gene mutations, compromised detoxification system, inflammation, abnormal neurotrophic factor and neurotransmitters levels [14,15].Vitamin D shows its impacts by binding to VDR[5]. Low VDR levels are thought to be able to affect ASD regardless of vitamin D levels. Therefore, studies assessing the relationship between the VDR and ASD are required.
Author Contributions
R.S. B. and A. A. and K. H. A. contributed to the interpretation and review of the research, checking the results and verifying the validity of what was stated in the research. R. A. K. contributed to designing and implementing the research, analyzing the results and writing this manuscript. The authors discussed the results and contributed to the final manuscript.
We have read and understood ALS policy on declaration of interests and declare that we have no competing interests.
![]() References
References
- Hodges H, Fealko C, Soares N. Autism spectrum disorder: definition, epidemiology, causes, and clinical evaluation. Translational pediatrics, (2020); (Suppl 1): S55-S65
- Kinney DK, Barch DH, Chayka B, Napoleon S, Munir KM. Environmental risk factors for autism: do they help cause de novo genetic mutations that contribute to the disorder. Med Hypotheses, (2010); 74(1):102-106.
- El-Ansary A, Al-Ayadhi L. Neuroinflammation in autism spectrum disorders. Journal of Neuroinflammation, (2012); 9(1): 1–9.
- RapinI, Tuchman RF. Autism: definition, neurobiology, screening and diagnosis. Pediatric Clinics of North America, (2008); 55(5): 1129-1146.
- Altun H, Kurutaş EB, ŞahinN, Güngör O, Fındıklı E. The levels of vitamin D, vitamin D receptor, homocysteine and complex B vitamin in children with autism spectrum disorders. Clinical Psychopharmacology and Neuroscience, (2018);16(4): 383.
- Eyles DW, Smith S, Kinobe R, Hewison M, McGrath JJ. Distribution of the Vitamin D receptor and 1α-hydroxylase in human brain. Journal of Chemical Neuroanatomy, (2005); 29(1): 21–30.
- Humble MB, Gustafsson S, Bejerot S. Low serum levels of 25-hydroxyvitamin D (25-OHD) among psychiatric out-patients in Sweden: relations with season, age, ethnic origin and psychiatric diagnosis. Journal of Steroid Biochemistry and Molecular Biology, (2010); 121: 467- 470.
- Mostafa GA, Al-Ayadhi LY. Reduced serum concentrations of 25-hydroxy vitamin D in children with autism: relation to autoimmunity. Journal of Neuroinflammation, (2012); 9: 201.
- Gong ZL, Luo CM, Wang L, Shen L, Wei F, Tong RJ, et al. Acknowledgments Vitamins, Homocysteine and Autism Spectrum Disorders 389 Serum 25- hydroxyvitamin D levels in Chinese children with autism spectrum disorders. Neuro report, (2014); 25: 23-27.
- Areej Sh. ,Israa F. Serum Level of Vitamin D receptor and Genetic polymorphism in children suffering from Autism. Annals of Tropical Medicine & Public Health, (2021); 24: 546-551.
- Kočovská E, Fernell E, Billstedt E, Minnis H, Gillberg C. Vitamin D and autism: clinical review. Res Dev Disabil, (2012); 33(5):1541-50.
- Saad K, Abdel-Rahman AA, Elserogy YM, Al-Atram AA, Cannell JJ, Bjørklund G, et al. Vitamin D status in autism spectrum disorders and the efficacy of vitamin D supplementation in autistic children. Nutritional Neuroscience, (2016); 19: 346-351.
- Must A, Phillips SM, Curtin C, Anderson SE, Maslin M, Lividini K, et al. Comparison ofsedentary behaviors between children with autism spectrum disorders and typically developing children. Autism, (2014); 18: 376-384.
- Rossignol DA, Frye RE. Evidence linking oxidative stress, mitochondrial dysfunction, and inflammation in the brain of individuals with autism. Frontiers in physiology, (2014); 5: 150.
- Groves NJ, McGrath JJ, Burne TH. Vitamin D as a neurosteroid affecting the developing and adult brain. Annual Review of Nutrition, (2014); 34: 117-141.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


