

Full Length Research Article
The Therapeutic Effect of Hydroxychloroquine on Patients with Recurrent Miscarriage and the Risk Assessment of its Ocular Retinal Toxicity
Ai Zhang1, Xianhe Zheng1, Xiaoli Zhu2, Jing Zheng1*
Adv. life sci., vol. 11, no. 1, pp. 162-172, February 2024
*- Corresponding Author: Jing Zheng (qqbovov@163.com)
Authors' Affiliations
2. Department of Gynecology, Wenzhou TCM Hospital of Zhejiang Chinese Medical University,Wenzhou, Zhejiang – China
[Date Received: 30/09/2023; Date Revised: 24/10/2023; Date Published: 25/02/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Recurrent miscarriage (RM) refers to the unfortunate loss of pregnancy at least three times before the 20th week of gestation. The present study examined hydroxychloroquine (HCQ)'s therapeutic effects in recurrent miscarriage owing to potential positive outcomes like increased rate of live births and negative outcomes like ocular and retinal toxicity.
Methods: The investigation involved the randomization of 400 mg of HCQ intervention in 91 pregnant women attending a monthly clinic at the Wenzhou TCM Hospital of Zhejiang Chinese Medical University.
Results: According to the results, HCQ results in positive pregnancy outcomes, with improving rates of live births with continued use of the medication. At the same time, the results produced significant safety issues, including HCQ deposition in the retina and ocular toxicity. An investigation of HCQ's effects on the retinal nerve fiber layer measurements, ganglion cell layer measurements, and the inner plexiform layer measurements revealed a dynamic trend.
Conclusion: We did not obtain conclusive outcomes regarding HCQ's effects on the changes in retinal measurements. However, the deposition of HCQ in the retina and the resulting vision loss, especially loss of color vision, stood out. These outcomes represent the safety and therapeutic effects of HCQ in pregnancy, posing concerns and creating the need for further studies. Interestingly, none of these outcomes were related to or dependent on the participants' age.
Keywords: HCQ; Recurrent miscarriage; Ocular retinal toxicity; Effects; Live births; Still birth
Introduction![]()
Recurrent miscarriage refers to the unfortunate loss of pregnancy at least three times before the 20th week of gestation. Even though World Health Organization reports that RM occurs in 2 to 5% of couples, investigations in low- and middle-income nations are yet to arrive at conclusive outcomes [1] and it puzzles scientists and patients as 75% of its causes remain unexplained [2,3]. Nonetheless, the current evidence indicates that RM occurs due to modifiable and unmodifiable risk factors. The recent interventions are capitalized on modifiable risk factors and their respective countermeasures, like patient follow-up for reducing fetal loss due to RM.
In the last decades, HCQ evoked much interest in the scientific community amid mixed therapeutic outcomes. Researchers associate HCQ with potential therapeutic effects on RM, albeit concerns and alarms regarding ocular toxicity in the ciliary body, cornea, and retina [4,5]. These delved into therapeutic effects among pregnant women, juxtaposing assessment of risks like ocular retinopathy. The intersection of HCQ's complex clinical inquiry regards the potential positive outcomes, the intricacies of ocular retinopathy, and the premature loss of pregnancy.
Many studies associate HCQ treatment with improved pregnancy outcomes like increased live births and reduced congenital malformation [6,7,8,9] and provide relief against autoimmune diseases like arthritis [10]. Quantifying the HCQ-related risk factors revealed a small risk of malformations in the first trimester. A risk-benefit analysis of HCQ use for autoimmune disorders like arthritis revealed that the benefits outweighed the risks. HCQ downregulates immune system functions, thereby lowering inflammation in autoimmune disorders. This effect may have resulted from the alteration of different inflammatory pathways [11,12].
Concerns regarding HCQ's ocular effects and retinal interference have risen in recent years. Some studies contest that HCQ interferes with the retinal nerve fiber layer, ganglion cell layer, and the inner plexiform layers' measurements and could result in vision loss. The long-term use of HCQ has been mentioned as the biggest threat to retinal toxicity, resulting in central vision loss or bull's-eye maculopathy [13]. Vision loss is directly associated with elevated deposition of HCQ in the blood vessels and binding to the melanin in the retinal pigment epithelium. Eventually, the binding damages the macular cones outside the fovea centralis, resulting in blindness.
The primary ocular symptoms of HCQ-induced retinopathy include reduced visual acuity, poor night vision, and partial loss of peripheral and central vision [14]. However, partial night vision and visual acuity loss occur at the later stages of using HCQ. These symptoms pre-empt the danger posed by HCQ and the relevance of investigating HCQ's ocular and retinal toxicity in pregnancy.
Despite the elaborate pathophysiology, there is insufficient evidence linking HCQ and loss of vision in pregnancy. The above-stated association between HCQ and vision loss or related complications is believed to cause visual complications among pregnant women with RM. The present study delved into an investigation of HCQ's therapeutic effects in pregnancy among women with RM. To find out whether the reported evidence is true, we deliberated a study on HCQ's effects on the retinal nerve fiber layer, ganglion cell layer, and the inner plexiform layers' measurements to represent the ocular and retinal effects of the drug. Also, the study investigated HCQ's effects on live births and focused on conclusive remarks regarding HCQ's safety in pregnancy.
Methods![]()
Description of the Study Area
The study was performed at Wenzhou TCM Hospital of Zhejiang Chinese Medical University. The study area was secure and protected to prevent any intrusion or interference. Only the researchers could access the study area. Additionally, the study design indicated the conditions for the researchers to access the study area, activities to be performed, and general conduct when in the study area.
Study Design, Sample Size, and Sampling Method
According to the guidelines, we conducted this study at Wenzhou TCM Hospital of Zhejiang Chinese Medical University. The study was carried out between 1st May 2021 and 30th September 2022 under the supervision of research and development. The randomized controlled approach was deployed in the study involving pregnant women who had not had a history of abortion. The sample size was randomly selected from the pregnant women attending the clinic at the facility. A guided approach was used in sample selection as the study focused on women who had recurrent miscarriages at least twice. In sample selection, the participants were required to present evidence of the miscarriage. The random selection focused on women with certified medical reports proving the recurrent miscarriages. Lastly, the study was timed at the time of the patient visit.
Eligibility Criteria
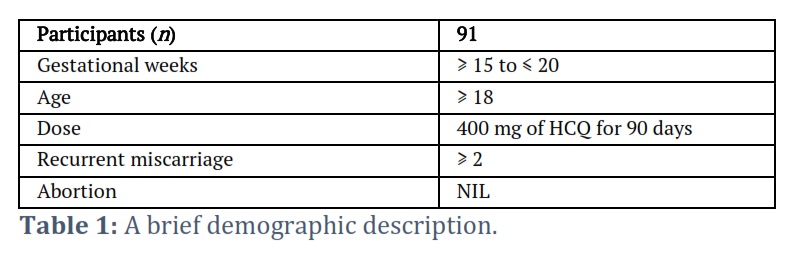
Our study incorporated a total of 91 pregnant women who were eligible for inclusion in the three-tier assessment of HCQ's therapeutic effects and potential risk factors. The inclusion criteria adopted to filter the patients considered the following: ❶ Only consenting pregnant women aged ≥ 18 years, above, ❷ Pregnant women with at ≥ 15 gestational weeks up to ≤ 20 gestational weeks, ❸ Only pregnant women with at least one miscarriage, and ❹ Pregnant women diagnosed with immune disorders requiring hydroxychloroquine (HCQ) treatment, without a diagnosis of ocular or retinal toxicity On the other hand, the study excluded: ❶ Women with a history of abortion, ❷ Pregnant women with > 20 gestational weeks, and ❸ Pregnant women who have not had recurrent miscarriages.
A Description of the Participant Population
The study was limited to pregnant women with a history of recurrent miscarriage. At the time of the investigation, the woman must be pregnant, preferably the ≥ 15 to ≤ 20 gestational weeks (Table 1). The table below captures the key demographic profile of eligible participants in this study.
Interventions and outcomes
HCQ was administered to the pregnant women in this study according to the indicated clinical guidelines. The intervention was scheduled to fit the patients' availability at the hospital for the clinical program. The 91 pregnant women received 400 mg of hydroxychloroquine daily for 90 days to improve pregnancy outcomes while observing the side effects. This intervention aimed to assess HCQ's effects on participants' rate of life births or successful pregnancies. Secondly, we assessed ocular and retinal toxicity by analyzing HCQ's effects on retinal thickness. Retinal changes at baseline, 3 months and 6 months were compared to inform HCQ's effects on the retinal measurements. Further, a correlational analysis was performed to relate age to retinal changes.
Thirdly, we sought therapeutic effects in pregnancy by measuring retinal thickness among participants. We contrasted the measurements at baseline, 3 months and 6 months to establish potential trends and patterns. In addition, we investigated the association between the resulting retinal thickness and age to determine whether age variance plays a significant role in the resulting ocular outcomes. Lastly, we investigated HCQ's ocular outcomes, focusing on renal toxicity and accumulation in the retina.
Statistical Analyses
The descriptive statistics were used to summarize the central tendency, the distribution of retinal thickness, or spread among the participants. The distribution included the minimum and maximum measurements and the data points 25th, 50th, and 75th percentile [15,16,17]. Further, we used the one-way ANOVA test with repeated measures to contrast retinal thickness at baseline (before taking the medicine), three months after, and 6 months after. This analysis was based on the null hypothesis that there were no significant differences in the retinal thickness measurements at baseline, 3 months and 6 months. The alternate hypothesis was a significant difference in retinal thickness in at least two assessments or at baseline, 3 months and 6 months.
To decipher the correlation between changes in retinal measurements and age, the Pearson correlational analysis was used to gauge the direction and strength of the linear relationship between the participant's age and changes in retinal thickness measurements. The analysis pursued a linear relationship between the two variables to support clinical or therapeutic effects [18,19]. The Pearson correlational coefficient was calculated and denoted as "r," ranging from -1 to 1, where;
- A non-existent or negligible linear relationship exists between age and retinal thickness measurements when r is close to 0.
- There is a strong negative linear relationship between age and changes in retinal thickness when r is close to -1.
- A strong positive linear relationship exists between age and changes in retinal thickness measurements when r is close to 1.
The p-value of the Pearson correlation coefficient informed whether the relationship occurred by chance or was statistically significant, where statistical significance was denoted by p-value ≤ 0.05.
Results![]()
Live Births, Miscarriages, and Possible Changes in Pregnancies
The baseline, 3 months and 6 months examinations focused on pregnancy outcomes like live births, miscarriages, and possible changes during pregnancy. To decipher HCQ's therapeutic effects, trends and patterns of the incidence of miscarriages, live births, and changes in pregnancy among the 91 participants were assessed at baseline (before medication), three months after medication, and six months after medication.
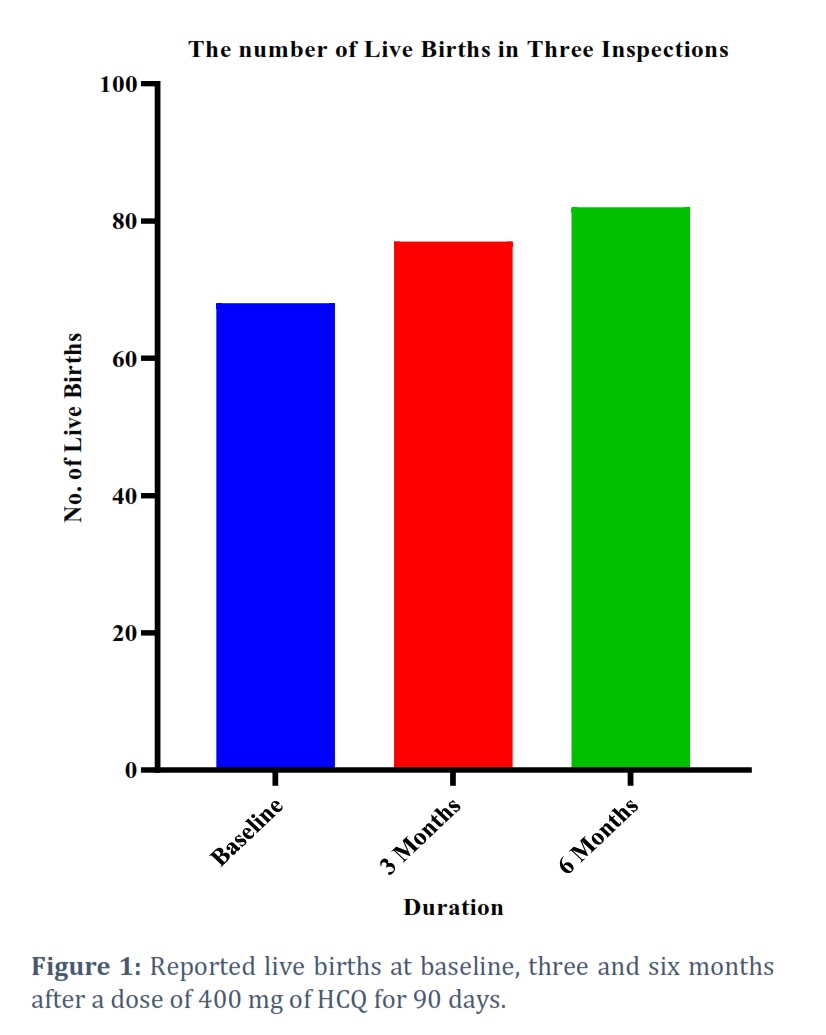
In Figure 1, notable trends in live births were observed across different time points. At the baseline, 68 live births were recorded, and this number increased to 77 at three months, further rising to 85 at the 6-month mark. This upward trajectory in live births suggests a potential positive association between HCQ administration and improved pregnancy outcomes in individuals with Recurrent Miscarriage. The observed increase in live births suggests a positive trend in terms of efficacy. The data indicates a potential benefit of HCQ in improving pregnancy outcomes for patients with Recurrent Miscarriage. However, it is important to note that individual responses can vary, and more extensive clinical studies are needed to establish the efficacy of HCQ in this specific context.
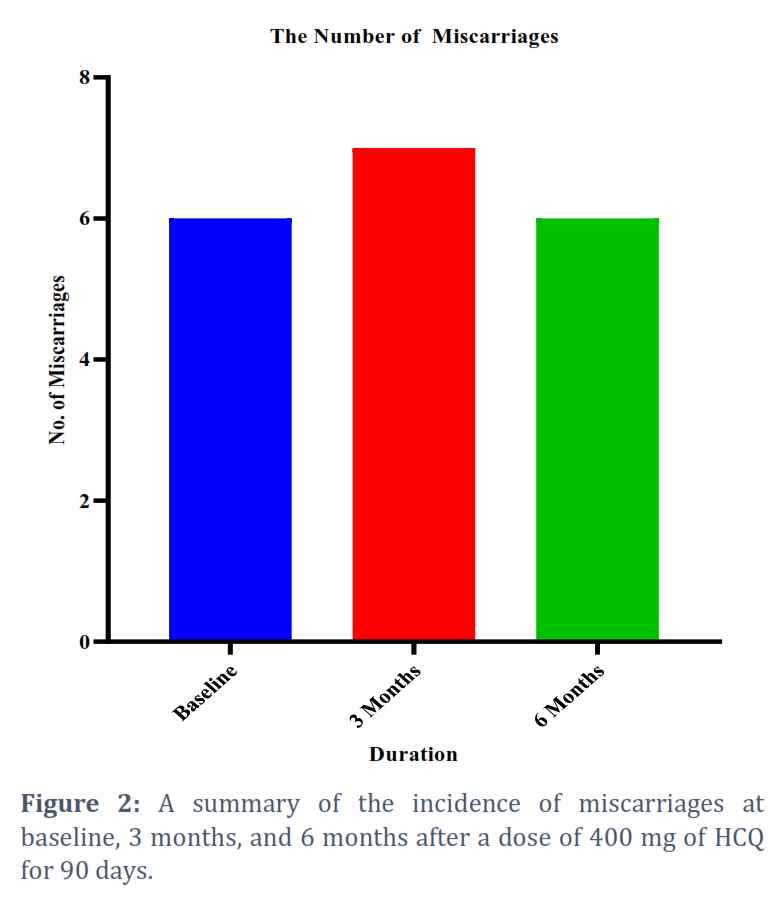
The assessment of miscarriages revealed HCQ's effects on RM. At the baseline, six miscarriages were recorded, and this number slightly increased to 7 at 3 months before decreasing to 6 at the 6-month mark. The observed fluctuations in miscarriage rates necessitate an evaluation of potential factors contributing to these occurrences. The fluctuations in miscarriage rates may prompt a closer examination of potential risks associated with HCQ, including any impact on early pregnancy viability. Careful monitoring for adverse effects and a thorough understanding of the medication's safety profile are essential (figure 2).
In Figure 3, the incidence of diarrhea among participants at 3 months was recorded at 27%. Diarrhea is a common gastrointestinal side effect associated with HCQ use. Monitoring dehydration and adjusting treatment if necessary is crucial in managing this side effect. The incidence of diarrhea decreased to 15.5% in 6 months. This reduction suggests a potential adaptation or resolution of this gastrointestinal side effect throughout treatment. Monitoring gastrointestinal symptoms and adjusting management strategies as needed remain important.
Approximately 17.6% of participants reported experiencing nausea at 3 months. Nausea is another gastrointestinal side effect commonly associated with HCQ. Addressing this symptom may involve adjusting the timing of medication administration or providing antiemetic support. The incidence of nausea also decreased to 14.3% at 6 months. A decline in nausea suggests a potential improvement in gastrointestinal tolerance to HCQ. Similar to diarrhea, ongoing monitoring, and supportive measures may be necessary.
28.4% of participants reported arthritis as an adverse effect at 3 months. Arthritis-like symptoms, including joint pain, are known side effects of HCQ. Monitoring the severity of joint symptoms and considering appropriate interventions are essential in managing this aspect. Arthritis-related symptoms increased to 44% in 6 months. This notable rise may indicate a cumulative effect or progression of arthritis-like side effects associated with HCQ. Management strategies, including potential adjustments to the treatment plan, should be considered in addressing these symptoms.
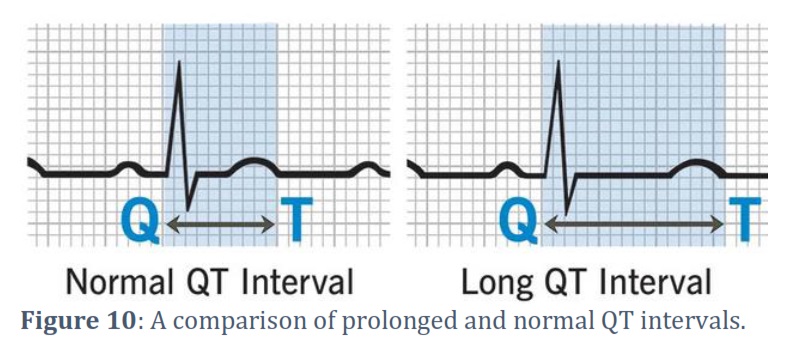
Prolonged QT intervals were reported in 27% of participants at 3 months. Prolonged QT is a cardiac side effect associated with HCQ use, and it requires careful monitoring as it can lead to serious cardiac arrhythmias. Regular electrocardiogram (ECG) monitoring is typically recommended in patients receiving HCQ. The incidence of prolonged QT intervals remained at 26.2% in 6 months. Cardiac monitoring remains crucial due to the persistence of this side effect, and adjustments to the treatment plan may be necessary to mitigate the risk of serious cardiac complications.
Ocular Toxicity and Retinal Measurement Outcomes
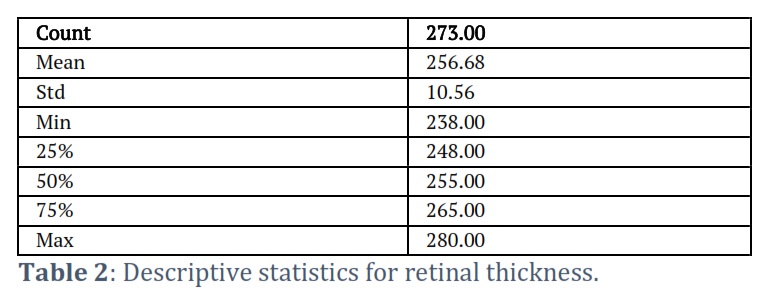
By description, the mean retinal thickness of the 91 participants was 256.68, and the standard deviation was 10.56. The standard deviation represented the viability of retinal thickness among the participants, suggesting a minimal margin of variation. The minimum retinal thickness was 238.00 μm, whereas the maximum was 280.00 μm. The percentile data revealed that the 25% percentile's retinal thickness was ≤ 248.00 μm and the 75%percentile's retinal thickness was ≤ 265.00 μm (table 2). These measurements are within the threshold retinal thickness measurements of 248.7 μm in males and 249.2 μm in females.
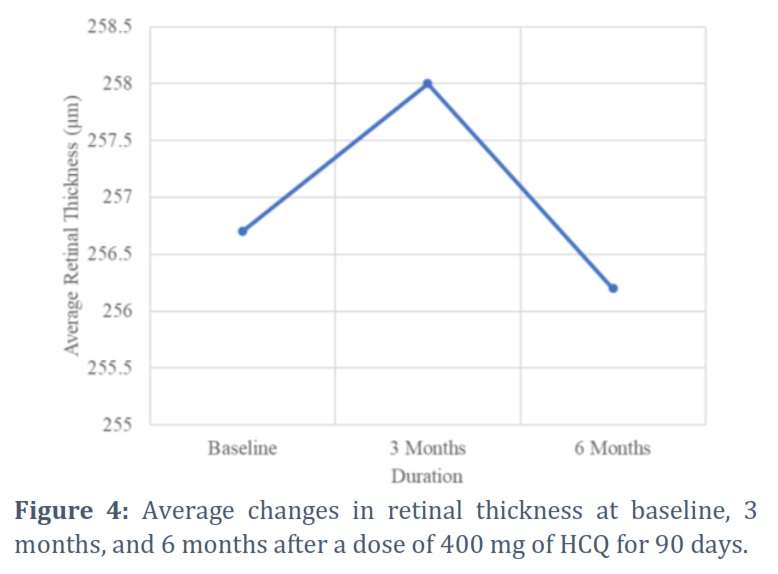
The results presented in Figure 4 show the average retinal thickness measured in micrometers (µmm) at different time points. The average retinal thickness at baseline was 256.7 µmm. This measurement serves as the initial reference point before the administration of HCQ. It indicates the baseline condition of the retina in patients with Recurrent Miscarriage. After 3 months of HCQ treatment, the average retinal thickness increased to 258 µmm. This slight increase could suggest a potential impact of HCQ on retinal thickness. Regular monitoring is essential, as this medication is known for its association with retinal toxicity. At the 6-month mark, the average retinal thickness decreased to 256.2 µmm. This decrease may indicate a stabilization or even a reversal of the earlier observed increase in retinal thickness. It is crucial to note that this change might be interpreted as a positive outcome, as it suggests a possible mitigation of adverse effects on retinal health.
ANOVA analysis was performed to compare retinal thickness following HCQ treatment for statistical significance. The ANOVA results found an F-statistic of 0.165 and a p-value of 0.848, suggesting a lack of statistical significance (table 3). The lack of statistical significance suggests negligible differences in the retinal thickness measurements at baseline, 3 months, and 6 months. Therefore, we rejected the null hypothesis. Further, we performed a correlational analysis of age and retinal thickness measurements and did not find statistically significant outcomes (p-value = 0.99) (table 3). These statistical outcomes asserted no relationship between retinal thickness and age.
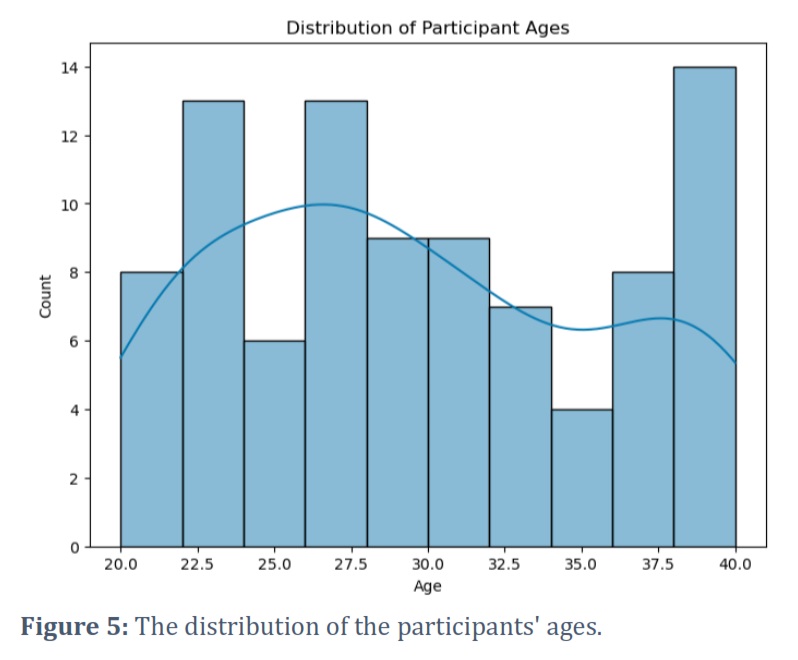
We analyzed age distribution by borrowing the proclaimed non-existent relationship between retinal thickness and the participants' age. Figure 5 represents the age distribution in the participant group. The data reveals a somewhat uneven age distribution across the participant group, suggesting that HCQ's effects in pregnancy are not age-dependent. The clinical effect of this observation is an age-independent indication of the drug for women with RM.
Retinal Toxicity and Visual Problems
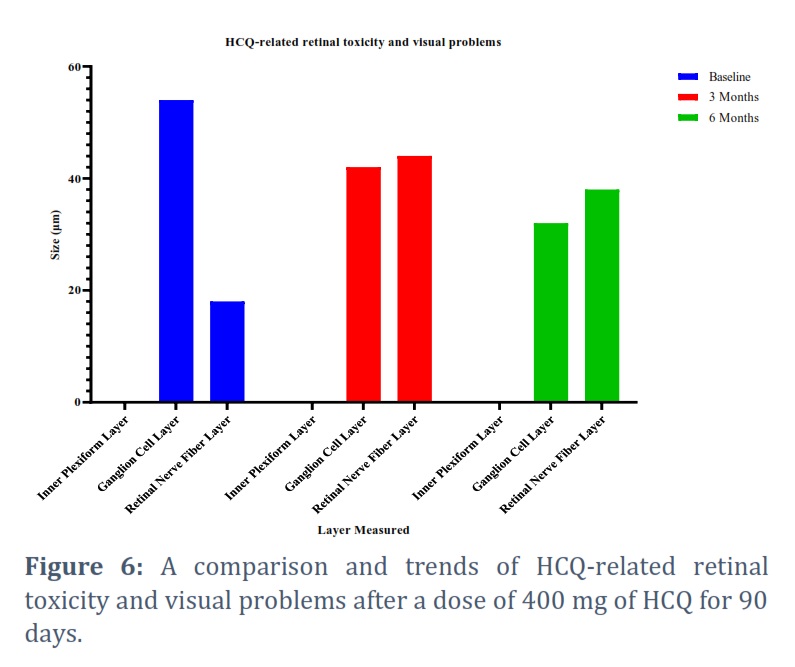
HCQ's retinal toxicity and visual problems invoked significant interest in the investigation. To decipher HCQ's retinal toxicity and visual complications in pregnancy, we independently assessed retinal nerve fiber layer measurements, ganglion cell layer measurements, and the inner plexiform layer measurements. We observed the trends to arrive at conclusive remarks regarding the therapeutic effects of 400 mg of HCQ treatment for 90 days.
In Figure 6, the decreasing thickness in the Ganglion Cell Layer over the treatment period suggests potential changes in the density or health of ganglion cells. Monitoring this layer is crucial, as alterations may impact visual function and could be associated with the known side effects of HCQ on the retina. Fluctuations in the Retinal Nerve Fiber Layer thickness, with an increase at 3 months and a decrease at 6 months, indicate dynamic changes in this layer. Monitoring the Retinal Nerve Fiber Layer is important, as even subtle alterations can affect visual function and may be linked to retinal toxicity associated with HCQ. Due to the minimal nature of these changes, the possibility of errors in examinations should also be considered.
The consistent measurement of the Inner Plexiform Layer at 0 µmm across all time points (Baseline, 3 Months, and 6 Months) suggests a unique aspect of retinal thickness that did not exhibit observable changes during the study period. It may suggest that this specific layer is less susceptible to measurable changes or that the measurement technique employed may have limitations in accurately capturing variations in this layer.
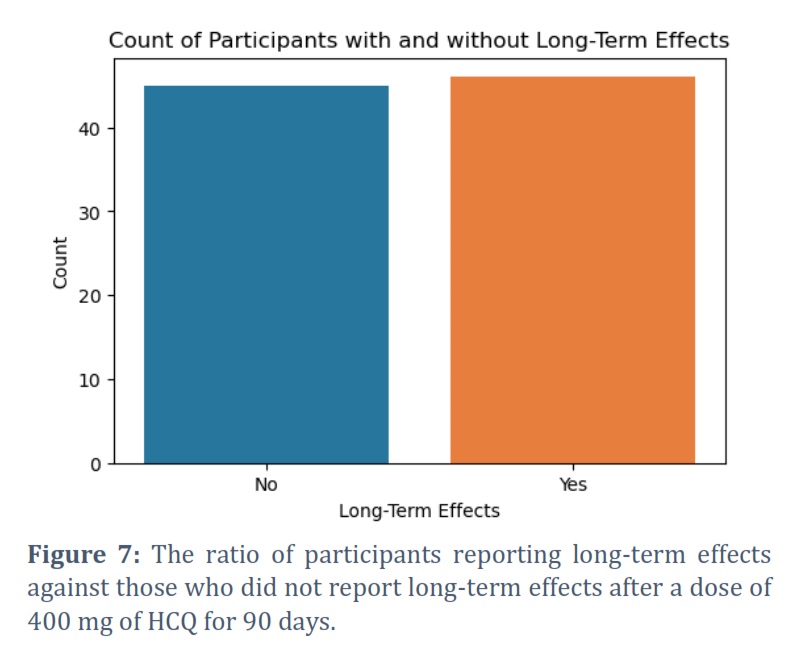
At 3 and 6 months after medication, we examined HCQ's long-term effects, including retinal nerve fibers, ganglionic cells, and the inner plexiform layers. In this assessment, we were keen to note any slight implications of the interventions in the patient's eyes. Interestingly, we found a relatively equal number of patients with potential long-term effects against those who did not report any outcomes. Significantly, the number of participants with overall long-term effects exceeded those who did not report long-term effects (figure 7). With about 50% of the participants reporting long-term effects, HCQ's safety and efficacy concerns emerged. The data posits that HCQ could inflict adverse effects on a large population of pregnant women with recurrent pregnancy if they are not closely monitored.
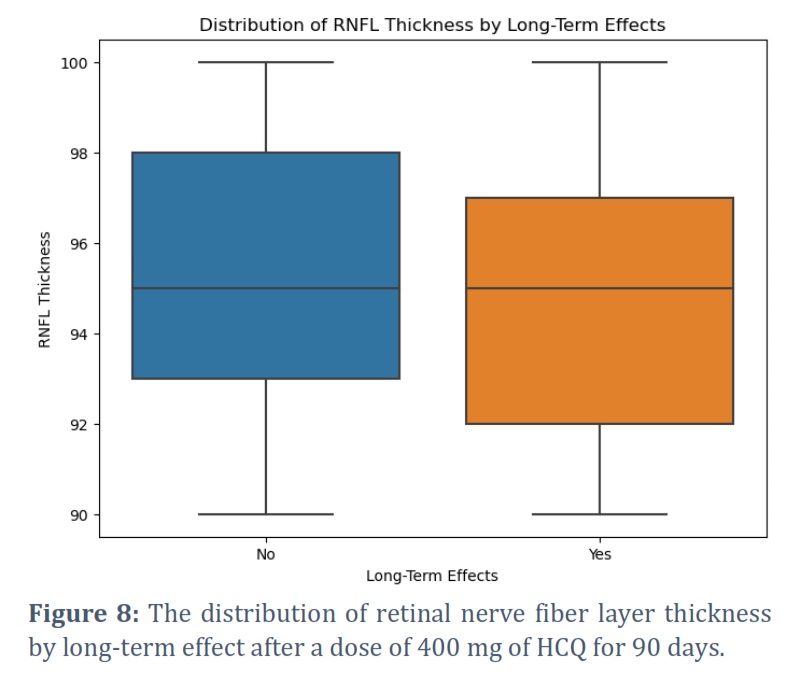
HCQ's long-term effects on ocular toxicity and retinal outcomes emerged as a dynamic aspect. We observed the differences in the central tendency and the spread of retinal nerve fiber layer measurements (RNFL) among participants who reported long-term effects and those who did not. The clinical data indicates that participants with RNFL thickness exceeding ≥ 95µm did not report long-term effects as their counterparts reported long-term effects (figure 8). We noted that RNFL thickness determined whether participants would experience long-term effects, with RNFL thickness exceeding ≥ 95µm more likely to induce long-term effects.
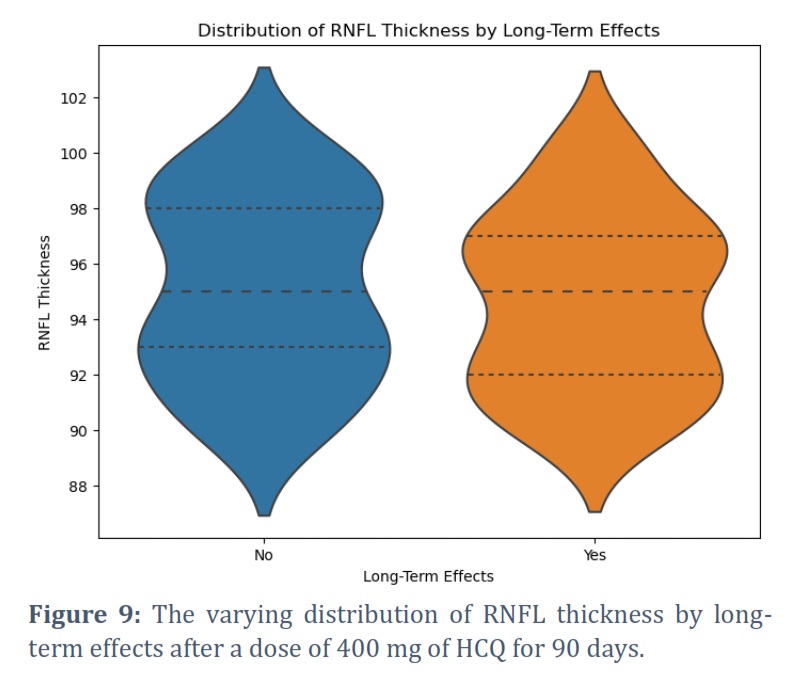
We examined the variations of the distributions of the RNFL thickness among participants who reported long-term effects and those who did not use violin plots. To decipher the varying distribution of RNFL's thickness, we observed the differences in the shapes of the violin plots representing participants reporting long-term effects. We contrasted them with those who did not report long-term effects. High variability of RNFL thickness in the group did not report long-term effects among participants found with RNFL thickness of 93µm and 98µm. The group reported the lowest variability with an RNFL thickness of 95µm. On the other hand, there was a high variability of participants with RNFL thicknesses of 92µm and 97µm, with minimum variability among participants found with a thickness of 95µm (figure 9).
Figures & Tables


RM remains a crucial health concern as it poses maternal and neonatal life-threatening risks. Many medications, including HCQ, have been indicated to manage RM without substantial outcomes. Even though HCQ has been flouted as an effective medication against rheumatic conditions among pregnant women, few research outcomes report its teratogenic implications [10,20]. HCQ’s rationale for the management of rheumatic conditions in pregnancy regards efficacy against inflammation associated with lupus or arthritis that causes premature fetal growth and birth complications [21]. In addition to this, studies supporting its use in pregnancy cite its chances of reducing the incidence of congenital heart block. On the other hand, evidence from other studies reports potential teratogenic effects like respiratory anomalies, urinary defects, oral clefts, and possible miscarriage, among other issues.
To decipher HCQ's therapeutic effects in pregnancy, pregnant women with a history of RM were treated with 400 mg of HCQ for 90 days and assessed at baseline, 3 months and 6 months. One of the primary findings of the study is that HCQ has positive effects on escalating live births or successful pregnancies among women who experienced RM. A preliminary analysis of the study outcomes strongly indicates a steady increase in live births from baseline to 3 months and 6 months following administration of 400 mg of HCQ for 90 days among pregnant women with RM. Even though the increase in live births is not tremendously large, the outcomes suggest that HCQ treatment is directly associated with improved pregnancy success. The finding poses a significant clinical significance and a breakthrough for women with RM.
Our outcomes agree with reports from some of the previous studies. HCQ has been reported to improve successful births among pregnant women with a history of RM by 57 to 67% [6,9]. These studies report that HCQ prevents flares during pregnancy, increasing the chances of successful births. Flares caused by systemic lupus erythematous cause adverse outcomes in pregnancy, like pre-eclampsia, loss of the fetus, or pre-term birth. Conclusive remarks regarding HCQ’s treatment among pregnant women with RM are improved neonatal and pregnancy outcomes [8,22]. In these studies, termination of HCQ treatment was recommended if pregnancy loss occurred within one year of treatment.
Despite a consistent increase in live births, the present study found inconsistent miscarriages among women receiving 400 mg of HCQ intervention for 90 days. A preliminary analysis of the clinical results revealed relatively stable miscarriages at baseline, 3 months, and 6 months. The highest number of incidences of miscarriage was reported at 3 months, a total of 7 miscarriages, then at 3 months and 6 months, each posting 6 miscarriages. The relatively stable rates of miscarriages raise questions on HCQ's mechanism of influencing pregnancy outcomes and underscore the need for further studies to obtain more data on HCQ's effects on miscarriage. HCQ is generally considered safe when used at appropriate doses for approved indications. However, its safety profile can vary among individuals and rare but serious side effects such as retinal toxicity has been reported. Healthcare providers must monitor patients regularly for potential adverse effects, especially considering the duration of treatment. While HCQ is generally well-tolerated, it is not without risks. Potential risks include adverse effects on the cardiovascular system, gastrointestinal issues, and skin reactions. Additionally, it is important to consider potential drug interactions and contraindications, especially if patients have pre-existing medical conditions or are taking other medications. Common side effects of HCQ may include gastrointestinal disturbances, skin reactions, and headaches.
Our study supports results from previous investigations and the position taken by HCQ's literature on miscarriage among pregnant women with RM. Literature and previous investigations report that HCQ does not increase miscarriage among pregnant women with a history of RM [7,23]. The main mechanism of reduced incidence of RM is the treatment of rheumatic illnesses and their related systematic complications affecting the kidneys. The treatment of rheumatic conditions and the kidney-related effects support pregnancy, setting grounds for successful pregnancy and live births. However, the previous studies and literature do not discredit possible pre-eclampsia that can be caused by HCQ among pregnant women. The possible incidence of pre-eclampsia suggests caution and prompts the need for further investigations into potential countermeasures.
The study revealed important outcomes indicating HCQ's adverse effects, crucial indicators of therapeutic outcomes. The study revealed a mixture of positive and adverse effects among the participants. A preliminary analysis of the outcomes indicated a decrease in some adverse effects, including diarrhea, prolonged QT intervals, nausea, and an increase in other adverse effects like arthritis. Interestingly, these adverse effects were not reported at baseline assessment, suggesting eradication and relief among participants. The varying incidence of adverse effects hinders conclusive remarks regarding the safety among pregnant women with RM. The decreasing adverse effects point to HCQ's key therapeutic effects among pregnant women with RM. The literature on HCQ's treatment among pregnant women with RM strongly indicates reduced adverse effects like diarrhea, prolonged QT intervals in the electrocardiogram, and nausea [8,22].
The decrease in the incidence of diarrhea and nausea is a positive trend regarding the safety profile of HCQ. Gastrointestinal side effects, including diarrhea and nausea, are common concerns with HCQ use. Reducing these adverse effects over time may suggest that patients could adapt to the medication or healthcare providers may implement strategies to manage these side effects effectively. It is consistent with the notion that many patients experience gastrointestinal side effects early in treatment but may see improvement with continued use. The decrease in the incidence of prolonged QT is a crucial aspect of the safety profile. Prolonged QT intervals on electrocardiograms can be associated with serious cardiac arrhythmias. The reduction in prolonged QT suggests that, over time, patients may have adapted to the medication, and careful monitoring or adjustments in treatment may have contributed to minimizing this cardiac risk. It highlights the importance of vigilant cardiac monitoring, especially given the known cardiac side effects of HCQ. The increase in arthritis as an adverse effect is noteworthy and may prompt closer scrutiny. Arthritis-like symptoms, including joint pain, are known side effects of HCQ. The escalation in the incidence of arthritis may necessitate carefully evaluating the balance between therapeutic benefits and potential side effects. This emphasizes the importance of considering both the safety and efficacy of HCQ in patients with RM.
These perspectives credit HCQ's indication for pregnant women to treat RM due to the delicate nature of pregnancy. However, the varying incidence of adverse effects, especially the increased incidence of arthritis, raises alarm over HCQ's safety and efficacy in pregnancy. The increasing incidence of arthritis among the participants contradicts the literature and results from previous studies supporting HCQ's indication against rheumatic complications. HCQ's safety in pregnancy is strongly associated with positive effects and treatment of rheumatic conditions like arthritis [24]. Therefore, contradicting outcomes should be investigated further. They could be outliers that should not pose great concerns or should be studied for possible underlying conditions.
We investigated HCQ's ocular effects and changes in the retina to unmask the therapeutic effects therein. The assessment aimed at ascertaining whether HCQ is safe in pregnancy or is a potential cause of retinal toxicity that indices irreversible vision loss [4,20]. Our analysis began with examining the resulting retinal thickness at baseline, 3, and 6 months. Importantly, we found that the retinal measurements of the participants fell within the ideal limits of 249.2 μm [25]. In the literature, HCQ's effects on parafoveal EZ disruption appear progressive. In the early stage, there is no disruption of the foveal E. In contrast, obvious and severe damage entails parafoveal disruption with an intact foveal EZ and disruption of parafoveal and foveal EZ, respectively.
An examination of retinal thickness measurements revealed slight changes, supported by the minimal thickness variability among the participants: 10.56. We tested the null hypothesis by assessing the changes in retinal thickness in the three assessments. The ANOVA test provided statistically significant results: an F-statistic of 0.165 and a p-value of 0.848. These outcomes led to the rejection of null hypotheses and the assertion of negligible differences or changes in retinal thicknesses with the progressive HCQ treatment. Our study results confirmed assertions from previous investigations that HCQ does not affect retinal thickness despite claims of retinal toxicity [25,26,27]. Yet, again, these findings assert HCQ’s safety and therapeutic effects in pregnancy. The minimal difference in the patients’ average retinal thickness asserts HCQ’s safety among pregnant women with recurrent pregnancy. The study’s outcomes dispel contention around HCQ’s retinal effects, including retinal damage after 5 years (Figure 6). Further, we did not find statistically significant results regarding the correlation between retinal thickness and age. Again, these findings agree with previous studies on pregnancy, where no correlation was reported between age and retinal thickness [16,28]. The clinical implication of this outcome is the indiscriminate indication of HCQ to pregnant without fear of adverse effects in a particular age group.
The increase in retinal thickness at 3 months raises awareness of the potential risk of retinal toxicity associated with HCQ. Retinal toxicity is a known side effect of HCQ, and changes in retinal thickness can serve as an early indicator of ocular complications. Regular ophthalmological assessments become crucial, as they allow for detecting any early signs of retinal toxicity or other ocular issues. These assessments may include detailed examinations of the macula, perimetry testing, and other relevant tests to monitor retinal health. Timely detection of ocular complications is essential for minimizing the risk of long-term visual impairment and ensuring patient safety. While retinal thickness is a safety concern, it is essential to assess the overall efficacy of HCQ in managing RM. The fluctuations in retinal thickness should be interpreted alongside the observed benefits and potential risks in the context of the study's primary objectives. Evaluating the efficacy involves considering the impact of HCQ on reducing the recurrence of miscarriages and improving overall pregnancy outcomes.
To decipher the realities and first-hand information on HCQ's effects on retinal measurements, we deliberated the measurements of retinal nerve fibers, the ganglionic cell layers, and the inner plexiform layers in three different expectations. In the first inspection, the retinal nerve fiber layer was measured at baseline, at 3 months, and at 6 months, and no significant trend of an increase or decline was noted. The retinal nerve fiber layer was observed to increase from baseline to 3 months and would decrease later at 6 months. A preliminary analysis of this outcome was a strong fluctuation in the measurements of the retinal nerve fibers across the study population. With only about a third of the study participants reporting inconsistent fluctuations, a solid conclusion regarding HCQ's effects on changes in retinal nerve fibers' measurements could not be made. Our results concur with previous investigations regarding HCQ's effect on the retinal nerve fiber layers. Evidence strongly suggests negligible impacts on retinal thickness and measurements [26]. We proceeded to investigate HCQ’s effects on the measurements of the ganglionic cells’ layers. The first inspection found a consistent decline in the cell layer’s measurements from baseline to 6 months. In other studies, HCQ was reported to decrease the measurements of the ganglionic cell layers, posing crucial clinical questions set for further investigations [29]. The consistent decline posited a crucial trend regarding HCQ's effects on pregnancy.
As for the inner plexiform layers, the participants posted a constant measurement over the assessment period. This observation affirms that HCQ does not affect the measurements of the inner plexiform in pregnancy. Some of the previous studies support these outcomes by asserting that HCQ treatment does not affect the inner retinal layers [29,30]. Outcomes from these studies suggest that HCQ treatment only affects the outer nuclear layers, the photoreceptor layers, and the retina pigment epithelia [31].
We assessed the long-term effects of HCQ in pregnancy by focusing on retinal and ocular toxicity. A preliminary analysis revealed that some of the participants reported potential long-term effects, whereas others did not report any long-term effects. Interestingly, RHFL thickness was the basis of incidence for long-term effects among pregnant women with RM. We measured the central tendency of participants reporting the long-term effects versus those who did not and found a high variability in the incidence of the long-term adverse effects. The clinical report indicated that participants whose RNFL thickness exceeded ≥ 95µm posted the highest incidence of long-term adverse effects. HCQ is known to have ocular side effects, including retinal toxicity. An increase in RNFL thickness could be an early sign of retinal changes associated with toxicity. Regular monitoring of RNFL thickness becomes crucial in detecting these changes promptly. Our studies concur with previous investigations on HCQ's toxicity on the retina. The long-term effects substantiate the discussion around vision loss and changes in color vision [13,32]. This clinical outcome indicates the danger of HCQ indication in pregnancy. Our findings assert HCQ's ocular and retinal toxicity, and long-term effects, suggesting caution and potential contraindication.
Further, we examined the variation of RNFL thickness' variations among the participants to determine the degree of the distribution; by plotting violin plots of participants reporting long-term effects vs. those who did not report long-term effects, we noted RNFL's thickness associated with the highest population variation. A comparison at 3 and 6 months revealed a higher variability in the group that did not report long-term effects. The high variability was associated with RNFL thickness of 93µm and 98µm. As for the group reporting adverse effects, high variability was reported among participants whose RNFL thickness measured 92µm and 97µm. Interestingly, the minimum variability in the group reporting long-term effects was found among participants whose RNFL measured 95µm.
HCQ's therapeutic effects among pregnant women with RM feature positive and negative outcomes on the incidence of RM and ocular-related risks like vision. Despite several studies, shortcomings and knowledge gaps exist regarding HCQ's safety and efficacy in RM. Our study investigated HCQ's effects on RM and found a positive and upward trajectory regarding live births. The conclusive remarks regarding HCQ's interventions against RM are positive outcomes, including successful pregnancies. As for the ocular toxicities and retinal effects, HCQ treatment poses concerning health outcomes, especially deposition in the retina. Our study found that the long-term effect of HCQ deposition in the retina is loss of vision, especially loss of visual abilities. However, our results did not establish a particular trend regarding HCQ's effects on the retina nerve fiber layer, ganglionic cell layer, and the inner plexiform layer measurements. Generally, we found that HCQ is considerably safe in pregnancy, with a few safety concerns, including the long-term effects that depend on the RNFL thickness.
Conflict of Interest
The authors declare that there is no conflict of interest.
All co-authors contributed significantly to designing and executing this study; and writing this manuscript.
![]() References
References
- Rajender S, Farghali M, Mohanty G, Uchenna Eleje G, Ugwu EO, et al. Prevalence and associated factors of recurrent pregnancy loss in Nigeria according to different national and international criteria. Frontiers in Reproductive Health, (2023); 5: 1049711.
- Basak S, Das RK, Banerjee A, Paul S, Pathak S, Duttaroy AK. Maternal obesity and gut microbiota are associated with fetal brain development. Nutrients, (2022); 14(21): 4515.
- Turesheva A, Aimagambetova G, Ukybassova T, Marat A, Kanabekova P, et al. Clinical medicine recurrent pregnancy loss etiology, risk factors, diagnosis, and management. fresh look into a full box. Journal of Clinical Medicine, (2023); 12: 4074.
- Yusuf IH, Sharma S, Luqmani R, Downes SM. Hydroxychloroquine retinopathy. Eye, (2017); 31: 828-845.
- Yusuf IH, Charbel Issa P, Ahn SJ. Hydroxychloroquine-induced retinal toxicity. Frontiers in Pharmacology, (2023); 14: 1196783.
- Abd Rahman R, Min Tun K, Kamisan Atan I, Mohamed Said MS, Mustafar R, Zainuddin AA. New benefits of hydroxychloroquine in pregnant women with systemic lupus erythematosus: a retrospective study in a tertiary centre. Revista Brasileira de Ginecologia e Obstetricia, (2020); 42(11): 705-711.
- de Moreuil C, Alavi Z, Pasquier E. Hydroxychloroquine may be beneficial in pre-eclampsia and recurrent miscarriage. British Journal of Clinical Pharmacology, (2020); 86(1): 39-49.
- Elisabeth P, de Saint-Martin L, Marhic G, Chauleur C, Bohec C, Bretelle F, Mottier D. Hydroxychloroquine for prevention of recurrent miscarriage: study protocol for a multicentre randomised placebo-controlled trial BBQ study. BMJ open, (2019); 9(3): e025649.
- Yang S, Ni R, Lu Y, Wang S, Xie F, Zhang C, Lu L. A three-arm, multicenter, open-label randomized controlled trial of hydroxychloroquine and low-dose prednisone to treat recurrent pregnancy loss in women with undifferentiated connective tissue diseases: Protocol for the Immunosuppressant regimens for LIving FEtuses (ILIFE) trial. Trials, (2020); 21(1): 1-9.
- Huybrechts KF, Bateman BT, Hernandez-Diaz S. Hydroxychloroquine early in pregnancy and risk of birth defects: absence of evidence is not the same as evidence of absence. American Journal of Obstetrics and Gynecology, (2021); 224(5): 549-550.
- Das RK, Datta T, Biswas D, Duss R, O’Kennedy N, Duttaroy AK. Evaluation of the equivalence of different intakes of Fruitflow in affecting platelet aggregation and thrombin generation capacity in a randomized, double-blinded pilot study in male subjects. BMC Nutrition, (2021); 7: 1-9.
- Barin A, Das RK, Bastani NE, Iversen PO, Duttaroy AK. Extracts of tamarillo, horned melon, and raspberries, but not extract of pear, inhibit human blood platelet aggregation: Investigating the underlying factors for their differential mechanisms. Research Square, (2023); 1-15.
- Mondal K, Porter H, Cole II J, Pandya HK, Basu SK, Khanam S, Chiu CY, Shah V, Stephenson DJ, Chalfant CE, Mandal N. Correction: Hydroxychloroquine causes early inner retinal toxicity and affects autophagosome–lysosomal pathway and sphingolipid metabolism in the retina. Molecular Neurobiology, (2022); 59(10): 3873-3887.
- Mititelu M, Wong BJ, Brenner M, Bryar PJ, Jampol LM, Fawzi AA. Progression of hydroxychloroquine toxic effects after drug therapy cessation: New evidence from multimodal imaging. JAMA Ophthalmology, (2013); 131(9): 1187-1197.
- Laarne P, Zaidan MA, Nieminen T. Non-linear correlation detection with mutual information. SoftwareX, (2021); 14: 100686.
- Liu C, Wei P, Li J. The thickness changes of retina in high myopia patients during the third trimester of pregnancy: a pilot study. BMC Ophthalmology, (2021); 21: 1-8.
- Yu Z, Guindani M, Grieco SF, Chen L, Holmes TC, Xu X. Beyond t test and ANOVA: applications of mixed-effects models for more rigorous statistical analysis in neuroscience research. Neuron, (2022); 110(1): 21-35.
- Saha A, Basu S, Datta A. RandomForestsGLS: an r package for random forests for dependent data. Journal of Open Source Software, (2022); 7(71): 3780.
- Zharbossyn A, Berkinova Z, Boribayeva A, Yermukhambetova A, Golman B. Numerical modeling of transport properties in battery electrodes. ECS Meeting Abstracts, (2020); 1(4): 529.
- Huybrechts KF, Bateman BT, Zhu Y, Straub L, Mogun H, Kim SC, Desai RJ, Hernandez-Diaz S. Hydroxychloroquine early in pregnancy and risk of birth defects. American Journal of Obstetrics and Gynecology, (2021); 224(3): 290.e1-22.
- Das D, Adhikary S, Das RK, Banerjee A, Radhakrishnan AK, Paul S, Duttaroy AK. Bioactive food components and their inhibitory actions in multiple platelet pathways. Journal of Food Biochemistry, (2022); 46(12): e14476.
- Pasquier E, De Saint-Martin L, Marhic G, Chauleur C, Bohec C, Bretelle F, Lejeune-Saada V, Hannigsberg J, Plu-Bureau G, Cogulet V, Merviel P, Mottier D. Hydroxychloroquine for prevention of recurrent miscarriage: Study protocol for a multicentre randomised placebo-controlled trial BBQ study. BMJ Open, (2019); 9(3): e025649.
- Albert CR, Mulla MJ, Han CS, Brosens JJ, Chamley LW, Abrahams VM. Hydroxychloroquine prevents antiphospholipid antibody-induced inhibition of trophoblast migration. American Journal of Reproductive Immunology, (2014); 71: 154-164.
- Bérard A, Sheehy O, Zhao JP, Vinet E, Quach C, Bernatsky S. Chloroquine and hydroxychloroquine use during pregnancy and the risk of adverse pregnancy outcomes using real-world evidence. Frontiers in Pharmacology, (2021); 12: 722511.
- Alamouti B, Funk J. Retinal thickness decreases with age: an OCT study. Brazilian Journal of Ophthalmology, (2003); 87: 899-901.
- Lee EJ, Kim SJ, Han JC, Eo DR, Lee MG, Ham DI, Kang W, Kee C, Lee J, Cha HS, Koh EM. Peripapillary retinal nerve fiber layer thicknesses did not change in long-term hydroxychloroquine users. Korean Journal of Ophthalmology, (2018); 32(6): 459-469.
- Uslu H, Gurler B, Yildirim A, Tatar MG, Kantarcj FA, et al. Effect of hydroxychloroquine on the retinal layers: a quantitative evaluation with spectral-domain optical coherence tomography. Journal of Ophthalmology, (2016); 2016: 8643174.
- Bozzo P, Chua-Gocheco A, Einarson A. Safety of skin care products during pregnancy. Canadian Family Physician, (2011); 57(6): 665-667.
- Bulut M, Erol MK, Toslak D, Akidan M, Kaya Başar E, Çay HF. A new objective parameter in hydroxychloroquine-induced retinal toxicity screening test: Macular retinal ganglion cell-inner plexiform layer thickness. Archives of Rheumatology, (2018); 33(1): 52.
- De Sisternes L, Hu J, Rubin DL, Marmor MF. Analysis of inner and outer retinal thickness in patients using hydroxychloroquine prior to development of retinopathy. JAMA Ophthalmology, (2016); 134(5): 511-519.
- Polat OA, Okçu M, Yılmaz M. Hydroxychloroquine treatment alters retinal layers and choroid without apparent toxicity in optical coherence tomography. Photodiagnosis and Photodynamic Therapy, (2022); 38: 102806.
- Geamănu Pancă A, Popa-Cherecheanu A, Marinescu B, Geamănu CD, Voinea LM. Retinal toxicity associated with chronic exposure to hydroxychloroquine and its ocular screening. Review. Journal of Medicine and Life, (2014); 7(3): 322.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


