

Review Article
A Review of the Effects of Omega-3 and Omega-6 on Alcoholic and Non-Alcoholic Fatty Liver
Mohammad Darvishi1, Khulood Majid Alsaraf2, Mariam Alaa Toama3, Salema K. Hadrawi4, Montather F. Ramadan5, Mohadeseh Pirhadi6, Omid-Ali Adeli7,8*
Adv. life sci., vol. 10, no. 4, pp. 530-536, December 2023
*- Corresponding Author: Omid-Ali Adeli (omidalieadeli@yahoo.com)
Authors' Affiliations
2. Department of Medical Engineering, Al-Esraa University College, Baghdad – Iraq
3. College of Pharmacy, National University of Science and Technology, Dhi Qar – Iraq
4. Refrigeration and Air-conditioning Technical Engineering Department, College of Technical Engineering, The Islamic University, Najaf – Iraq
5. College of Dentistry, Al-Ayen University, Thi-Qar – Iraq
6. Department of Environmental Health, Food Safety Division, School of Public Health, Tehran University of Medical Sciences, Tehran – Iran
7. Department of Pathology, School of Medicine, Lorestan University of Medical Sciences, Khorramabad – Iran
8. Razi Herbal Medicines Research Center, Lorestan University of Medical Sciences, Khorramabad – Iran
[Date Received: 03/05/2023; Date Revised: 11/09/2023; Date Published: 31/12/2023]
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Non-alcoholic fatty liver disease is a type of fatty fat that causes an increase in alcohol consumption. Excessive alcohol consumption causes inflammation, and liver damage. The certain fatty acids (FAs) may be involved in this liver damage. Anti-inflammatory and blood lipid lowering effects are the effects of omega-3 unsaturated fatty acids (n-3 PUFAs). NAFLD is the hepatic manifestation of metabolic syndrome because obesity and insulin resistance are the main pathogenic factors of both diseases. NAFLD is a disease associated with metabolic syndrome. Most patients with NAFLD are obese, although the disease can also affect non-obese people. Metabolic and genetic factors play an important role in the occurrence of this disease. Oxidative stress, lipotoxicity and inflammation play a key role in the development of NAFLD. There is a lot of evidence for the therapeutic potential of omega-3 PUFAs fatty acids (n-3 PUFA), mainly docosahexaenoic acid and eicosatetraenoic acid in the treatment of metabolic diseases due to their antioxidant and anti-inflammatory properties. Therefore, in this review article, we examined the effects of omega-3 and omega-6 on alcoholic and non-alcoholic fatty liver disease.
Keywords: Omega-3; Omega-6; NAFLD; EPA; DHA
Introduction![]()
The organs of the body suffer from chronic diseases [1-3]. One of these organs is the liver. The largest visceral organ of the human body is liver, which is the center of many physiological processes. The liver has double blood; the celiac artery, that supplies oxygenated blood directly through the hepatic artery, and the portal vein, which brings nutrient-rich blood from visceral organs, such as the intestines, to the liver [1]. Consumption of simple sugars, inactivity, and obesity are among the underlying factors for a person to suffer from liver diseases, and excessive production of glucose and triglycerides by the liver are known as two key factors in the increase of fatty liver disease [2].
Non-alcoholic steatohepatitis (NAFLD) and alcoholic steatosis (ALD) are the two main categories of steatohepatitis [2,3]. NAFLD is recognized as an emerging health problem in Asia, which is associated with diseases such as diabetes, obesity, cardiovascular disease, and atherosclerosis. According to statistics presented in various studies, the prevalence of NAFLD is high in Asia (15 -20%) and is increasing over time. Far countries such as Republic of China, Hong Kong and Japan report a higher prevalence in the population than South Asian countries including India, Sri Lanka. Among the reasons for the high prevalence of FLD in Asia can be mentioned:
- Asians are more sensitive to non-communicable metabolic syndrome diseases (atherosclerosis, diabetes, and hepatic steatosis) than other races.
- Alcohol consumption is higher among Asians
More than a quarter (27-34%) of the general American population has non-alcoholic fatty liver disease. Similar to Asia and North America, the prevalence of fatty liver disease is also very high in Europe. A quarter of Europeans suffer from this disorder, and its prevalence rates vary from 8% in Romania to 45% in Greece. Today, the prevalence of each type of alcoholic and non-alcoholic fatty liver disease is increasing. Both forms of the disease tend to cause cirrhosis and liver carcinoma [2].
When histological observations confirm more than 5% of liver cells containing lipid droplets, the person has NAFLD [4]. NAFLD is related to fatness, diabetes, and insulin resistance and is considered a hepatic manifestation of the metabolic syndrome [3,4]. This syndrome, by creating metabolic complications such as increased blood glucose, VLDLs and CRP has a negative effect on the patient’s survival and cause type 2 diabetes, cardiovascular diseases, and advanced liver disease [5, 6]. Although obesity seems to be an important factor in the creation of NAFLD disease, not all obese people are affected by this disease, and observations have confirmed that thin people are affected [6]. On the other hand, alcohol consumption can cause ALD. This disease is associated with the fat agglomeration in the liver and causing complications such as weakness, anorexia, weight loss, abdominal discomfort and jaundice appears, although sometimes it is asymptomatic. International Classification of Diseases has classified ALD into different types of fatty liver, alcoholic hepatitis, liver fibrosis and sclerosis, alcoholic liver cirrhosis and liver failure [7]. In case of conversion of alcoholic fatty liver disease to cirrhosis, the disease may remain silent for years and it can be diagnosed only by imaging, also Liver biopsy can help diagnose the disease in certain cases. Imaging of alcoholic cirrhosis with symptoms such as nodular appearance of the liver, and a higher volume index of the caudate lobe. In this people cirrhosis may cause weakness, peripheral edema, jaundice, symptoms of gastrointestinal bleeding or abdominal distension. Megaloblastic anemia is common in these patients. Steatosis is a characteristic of the tissue that is seen in all patients with NAFLD. This condition causes the accumulation of lipids in 5% of the hepatocytes. Vacuoles of hepatocytes can be seen in large and medium sizes using the light of a microscope and without the need for special techniques [8]. So far, no particular drug therapy has been discovered to treat this disease but actions that reduce alcoholic fatty liver disease include: dietary modification, regular exercise, stopping alcohol consumption for more than 3 to 12 months, drug treatments such as: acamprosate, naltrexone, disulfiram, and baclofen. On the other hand, to improve non-alcoholic fatty liver disease, doing things such as reducing 3 to 5 percent of the initial weight, doing exercise and fitness, taking vitamin E for 4 to 96 weeks, Increasing the use of Rosiglitazone and Metformin to increase insulin sensitivity, Statins and Fibrates to treat hypertriglyceridemia, Long-Chain Polyunsaturated Fatty Acids such as omega-3 and omega-6, Pentoxifylline and Exenatide and finally surgery are recommended as suggested and not definitive treatments.
Progression of alcoholic fatty liver disease: Normal ↔ Increased risk ↔ Fatty liver ↔ NASH ↔ Fibrosis → Cirrhosis → Death
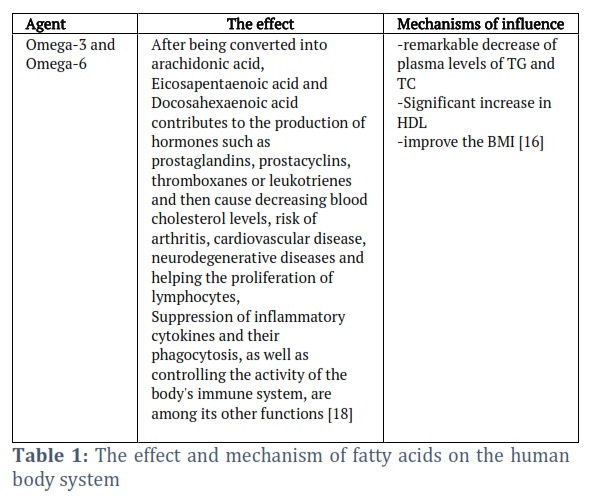
Deficiency of vitamin A, B12 and zinc is associated with alcoholic fatty liver, however, the data shows that increased intake of vitamin A can also be toxic to the liver and is a predisposing factor for alcoholic fatty liver, as well as excessive iron levels can cause an increase in mortality in people with alcoholic fatty liver Although there are data that suggest the effective role of some fatty acids in the therapy of hepatic steatosis and related metabolic disorders [5, 7]. Fatty acids omega-3 (a-linolenic acid) and omega-6 (linoleic acid) are part of polyunsaturated fatty acids (PUFAs) and essential, which are not made in the body of mammals and are obtained through diet. The most important biologically active fatty acids such as, Arachidonic acid from the Omega 6 family, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) from the Omega 3 family. Fish, seafood, and nuts have a high content of omega-3 fatty acids, whereas omega-6 fatty acids are found in animal foods and plant oils [9, 10]. Diets that have a very high content of omega-6 to omega-3 cause many diseases, including cardiovascular disease, inflammatory diseases, cancer, and autoimmunity. This is while enhancing the level of omega-3 to omega-6 has an inhibitory effect on the occurrence of many diseases [11-15]. Some fatty acids can affect inflammation through different mechanisms, they can change the signaling of inflammatory cells by affecting the fluidity of the cell membrane and the receptors inside the cell, and they can also control the gene expression patterns. Cells involved in the inflammatory response are usually rich in arachidonic acid, an omega-6 fatty acid, and eicosanoids derived from arachidonic acid are involved in inflammation. Meanwhile, EPA and DHA cause the production of resolving, which have anti-inflammatory effects [16]. In general, there are data based on the decrease in EPA and DHA levels in invalids with fatty liver disease compared to healthy people, such that the administration of omega-3 increases the amount of EPA and EHA in the blood and decreases omega-6. These changes cause positive effects on it becomes hepatic steatosis [4, 17]. In table 1, you can see the mechanism of action and how these two fatty acids affect the human body.
Methods![]()
Literature Search and Selection Criteria
In this review study, Embase, Magiran, SID, Web of Science, Scopus, PubMed and Google Scholar databases were searched using the keywords "Omega-3; Omega-6, alcoholic and non-alcoholic fatty liver". For each Case, selected published clinical trial and review articles were used. Inclusion criteria included articles related to keywords, and exclusion criteria included articles with only abstracts, articles in languages other than English.
Discussion![]()
Several studies have stated that lifestyle changes, diet, quality and quantity of exercise and various drug treatments may have affected fatty liver disease [17, 23, 24]. Fatty liver disease tends to cirrhosis and liver carcinoma, so lifestyle changes such as daily exercise and proper diet can be an effective step in preventing this process [25]. There are no current FDA-approved therapies for this disease, but the use of traditional therapies including pioglitazone and vitamin E has been significant for inflammation and steatosis, but no effect on fibrosis, which is the strongest predictor of mortality in this disease [26]. The incidence rate of hepatic steatosis has been increased due to the increase of obesity in societies [27]. On the other hand, the findings show a significant correlation between the decrease of liver fat and weight reduction [28]. In obese patients with NAFLD who do not respond to weight reduction, bariatric surgery can be suggested as a suitable therapeutic solution because it can significantly improve steatosis, inflammation, and fibrosis [29-32]. Many studies emphasized the effects related to the consumption of omega-3 fatty acids on liver metabolism and reducing its inflammation [33-36]. The obtained evidence indicates that omega-3 supplements have an effective role in decreasing TG and LDL levels, improving disease and obesity in NAFLD patients [17, 37] . Jump et al., 2016 also stated the possible role of DHA in avoiding NASH and decreasing the risk of hepatocellular carcinoma [38]. In addition to improving liver function in patients with NAFLD, omega-3 unsaturated fatty acids (PUFA) reduce cardiovascular diseases [39]. Lytle et al., 2017 described that DHA supplementation had no effect on body weight or blood glucose levels. They also stated that this supplement has the effect of stopping the process of hepatic steatosis, inflammation, fibrosis, or liver damage [40]. Oscarsson et al., 2018 stated that omega-3 consumption reduces the amount of serum triglycerides levels but did not significantly reduce the content of liver fat in NAFLD patients without diabetes and hypertriglyceridemia [41]. Masterton et al., 2010 admitted that omega-3 fatty acids in addition to reducing inflammatory markers cause to decrease hepatic steatosis and improve insulin sensitivity of patients [42]. The levels of omega-3 fatty acids in the blood serum of patients with type 2 diabetes (T2DM) and non-alcoholic fatty liver disease (NAFLD) are lower than those of healthy people. Feeding these people with omega-3 supplements for 12 weeks showed a significant decrease in serum TG levels [43]. There were also studies that claimed no support for PUFA supplements in improving the symptoms of diabetics [44]. The process of oxidative stress in combination with inflammation has a significant effect on the progression of NAFLD to NASH among the elderly people. Therefore, antioxidant, immuno-modulatory and anti-inflammatory characteristics of omega-3 polyunsaturated fatty acids make this supplementation an effective option for reducing liver fat in elderly invalids with NAFLD, but the efficacy of this supplement in reducing liver fibrosis is still unclear [45]. In addition to these, other studies also showed the role of omega-3 supplementation in treating hepatic steatosis and improving liver function in children with NAFLD [46, 47]. Shpiro et al., 2011 supported the role of omega-3 supplement in improving of NAFLD/NASH patients and recommended histopathology evaluation before and after treatment with this supplement and also stated two meals a week of oily fish suitable for these patients [48]. Musa-Veloso et al., 2018 stated that omega-3 fatty acids showed their effectiveness in improving the performance of people with NAFLD, but histological characteristics of people with NASH did not improve after taking omega-3, therefore, more trials are needed to better discovery the impacts of omega-3 fatty acids on patients with NASH [49]. The study of animal models showed the improving effect of omega-3 fatty acid supplementation in reducing hepatic steatosis in murine [27]. de Castro et al., 2018 confirmed reduction of inflammatory markers in NAFLD due to the consumption of n-3 PUFAs and admitted that in cases where we see the ineffectiveness of these supplements, the reason can be sensitivity of the methods used, the short duration of use, patient-specific factors and poor compliance [50]. Several studies, while confirming the effective effects of omega-3 supplements, stated that the optimal dose of this supplement to produce the desired effects is currently not known [45, 51, 52]. Therefore, it is recommended to conduct clinical trials with a specific duration and a specific endpoint in order to investigate the long-term impacts of these supplements [53, 54]. On the other hand Cansancao et al., 2020, while confirming the role of DHA supplementation in reducing liver fibrosis and recommended the appropriate dose and duration for the treatment of NAFLD patients, although they emphasized that more experiments are needed to confirm these findings [55]. Sangouni et al., 2021 showed that treating patients with omega-3 supplements for 12 weeks improves fatty liver index, visceral obesity index and lipid accumulation product [56]. Chronic and non-chronic, infectious and non-infectious diseases such fatty liver, cancers and etc. are serious health problems and cause pain and suffering to the patient, and finding a treatment solution for them seems essential [57-64]. Chronic diseases are very common [65-67]. Today, the desire to use medicinal plants and therapeutic agents in the treatment of diseases has increased because they are rich in secondary medicinal substances and antioxidants and improve diseases [68-73]. Jump et al., 2018 confirmed the effective role of omega-3 in improving liver inflammation, but pointed out a number of limitations in the way of evaluating the effects of fatty acids on improving the process of liver activity, these limitations include: 1) The low number of participants in clinical trials, 2) Failure to prove the effect of omega-3 fatty acids in increasing the levels of EPA or DHA or reducing the amount of TAG in the blood, 3) Slow healing process of fibrosis compared to hepatic steatosis and 4) Successful reconversion of DHA to its derivatives in tissues and the opposite point, reconverting EPA to derivatives that have the inability to reduce inflammatory markers in fatty liver disease [52].
Figures & Tables
Epidemiological studies show that metabolic syndrome is a main concern in public health issue. By examining the studies conducted in the field of metabolic syndrome and fatty liver in this review article, the close relationship between fatty liver and metabolic syndrome as well as the undeniable role of nutrition and diet in their prevention and pathogenesis was shown. Finally, it seems that the reduction of omega-3 and omega-6 intake from food sources due to its association with incorrect eating habits can be the main reasons for the multifactorial nature of this disease. Also, taking its supplement can be useful for these patients along with modifying the food pattern and lifestyle.
Acknowledgement
The authors thankful from Shahid Beheshti University of Medical Sciences, Tehran, Iran for the support. The co-corresponding author of the article is Dr. Nasrullah Naghdi.
Conflict of Interest
The authors declare no conflict of interest.
Epidemiological study of Monkeypox: Khulood Majid Alsaraf, Mariam Alaa Toama, Salema K. Hadrawi, Montather F. Ramadan, Mohadeseh Pirhadi
Design the review article: Mohammad Darvishi, Mohadeseh Pirhadi, Omid-Ali Adeli Contributed to article writing: Seyedeh Mahsa Khodaei, Omid-Ali Adeli.
![]() References
References
- Falih BT, Mohammed ST, Mohammed NJ. Effects of the silver nanoparticle synthesis from the leaves of the Capparis spinosa plant on the liver of mice infected with visceral leishmaniasis. Caspian Journal of Environmental Sciences, (2022); 20(4): 785-791.
- Mandil O, Sabri H, Manouchehri N, Mostafa D, Wang HL. Root coverage with apical tunnel approach using propolis as a root conditioning agent: A case report with 2‐year follow‐up and review of the literature. Clinical and Experimental Dental Research, (2023); 9(4): 568-573.
- Manouchehri N, Ghodsi S, Atri F, Sarraf P, Seyedi D, Valizadeh S. Effect of pretreatment of root dentin surface with cold atmospheric plasma on improving the bond strength of fiber post and resin cement: In vitro study. Clinical and Experimental Dental Research, (2023.);9(4):653-660.
- Tobin D. Evaluation of a High Concentrate Omega-3 for Correcting the Omega-3 Fatty Acid Nutritional Deficiency in Non-Alcoholic Fatty Liver Disease (CONDIN). Nutrients, (2018); 10(8): 3.
- Della Corte C, Iasevoli S, Strologo AD, Sanseviero M, Nobili V Chapter Two – Omega-3 Fatty Acids and Fatty Liver Disease in Children, in Advances in Food and Nutrition Research, F. Toldrá, Editor, (2018); 59-77.
- Kotronen A, Yki-Järvinen H. Fatty liver: a novel component of the metabolic syndrome. Arterioscler Thrombosis Vasccular Biolology, (2008); 28(1): 27-38.
- Rehm J, Samokhvalov AV, Shield KD. Global burden of alcoholic liver diseases. Journal of Hepatology, (2013); 59(1): 160-168.
- Chalasani N, Szabo G. Alcoholic and non-alcoholic fatty liver disease, Springer, (2015): 23(2): 5.
- Lee S, Gura KM, Puder M. Omega-3 fatty acids and liver disease. Hepatology, (2007); 45(4):841-845.
- El-Badry AM, Graf R, Clavien PA. Omega 3 – Omega 6: What is right for the liver? J Hepatology, (2007); 47(5): 718-25.
- Simopoulos AP. The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Experimental Biolology Medicine, (2008); 233(6): 674-88.
- Jiang H, Wang L, Wang D, Yan N, Li C, Wu M, Wang F, Mi B, Chen F, Jia W, Liu X Omega-3 polyunsaturated fatty acid biomarkers and risk of type 2 diabetes, cardiovascular disease, cancer, and mortality. Clinical Nutrition, (2022); 41(8): 1798-1807.
- Miura K, Hughes MC, Ungerer JP, Green AC. Plasma eicosapentaenoic acid is negatively associated with all-cause mortality among men and women in a population-based prospective study. Nutrition Research, (2016); 36(11): 1202-1209.
- Zhuang P, Wang W, Wang J, Zhang Y, Jiao J. Polyunsaturated fatty acids intake, omega-6/omega-3 ratio and mortality: Findings from two independent nationwide cohorts. Clinical Nutrition, (2019); 38(2): 848-855.
- Calder PC, Yaqoob P. Omega-3 (n-3) fatty acids, cardiovascular disease and stability of atherosclerotic plaques. Cell Molecular Biology, (2010); 56(1): 28-37.
- Calder PC. Fatty acids and inflammation: the cutting edge between food and pharma. Eur Journal of Pharmacology, (2011); 668(1): 50-8.
- Lee CH. Effects of Omega-3 Polyunsaturated Fatty Acid Supplementation on Non-Alcoholic Fatty Liver: A Systematic Review and Meta-Analysis. Nutritions, (2020); 12(9): 276.
- Szostak A, Ogłuszka M, Te Pas MF, Poławska E, Urbański P, Juszczuk-Kubiak E, Blicharski T, Pareek CS, Dunkelberger JR, Horbańczuk JO, Pierzchała M. Effect of a diet enriched with omega-6 and omega-3 fatty acids on the pig liver transcriptome. Genes Nutrition, (2016); 11(1): 1-17.
- Hodson LF. Rosqvist, and S.A. Parry, The influence of dietary fatty acids on liver fat content and metabolism. Proceture Nutrition Society, (2020); 79(1): 30-41.
- Lazo M, Clark JM. The epidemiology of nonalcoholic fatty liver disease: a global perspective. in Seminars in liver disease. 2008. Thieme Medical Publisher, (2008).
- Valantinas J, Apanaviciene DA, Maroziene L, Sveikata A. The prevalence of metabolic risk factors among outpatients with diagnosed nonalcoholic fatty liver disease in Lithuania. Medical Science Monitor: International Medical Journal of Experimental Clinical Research, (2012); 18(5): 57.
- Younossi ZM, Stepanova M, Negro F, Hallaji S, Younossi Y, Lam B, Srishord M.Nonalcoholic fatty liver disease in lean individuals in the United States. Medicne, (2012); 91(6): 319-327.
- Keating SE, Hackett DA, Parker HM, O’Connor HT, Gerofi JA, Sainsbury A, Baker MK, Chuter VH, Caterson ID, George J, Johnson NA. Effect of aerobic exercise training dose on liver fat and visceral adiposity. Journal of Hepatology, (2015); 63(1): 174-82.
- Sung, K.C. Effect of exercise on the development of new fatty liver and the resolution of existing fatty liver. Journal of Hepatology, (2016); 65(4): 791-797.
- Liu CH, Ampuero J, Gil-Gómez A, Montero-Vallejo R, Rojas Á, Muñoz-Hernández R, Gallego-Durán R, Romero-Gómez M. Lifestyle changes in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis. PloS one, (2022); 17(2): 0263931.
- Oseini AM Sanyal AJ. Therapies in non-alcoholic steatohepatitis (NASH). Liver International, (2017); 37 (1): 97-103.
- Alwayn IP.Omega-3 fatty acids improve hepatic steatosis in a murine model: potential implications for the marginal steatotic liver donor. Transplantation, (2005); 79(5): 606-8.
- Šmíd V.Effect of Omega-3 Polyunsaturated Fatty Acids on Lipid Metabolism in Patients With Metabolic Syndrome and NAFLD. Hepatology Communications, (2022); 6(6): 1336-1349.
- Bonsembiante L, Targher G, Maffeis C. Non-alcoholic fatty liver disease in obese children and adolescents: a role for nutrition? Euopean Journal of Clinical Nutrition, (2022); 76(1): 28-39.
- Nobili V. Indications and limitations of bariatric intervention in severely obese children and adolescents with and without nonalcoholic steatohepatitis: ESPGHAN Hepatology Committee Position Statement. ournal of Pediatrics Gastroenterology Nutrition, (2015); 60(4): 550-61.
- Bower G, Toma T, Harling L, Jiao LR, Efthimiou E, Darzi A, Athanasiou T, Ashrafian H. Bariatric Surgery and Non-Alcoholic Fatty Liver Disease: a Systematic Review of Liver Biochemistry and Histology. Obesity Surgery, (2015); 25(12): 2280-9.
- Lassailly G, Caiazzo R, Buob D, Pigeyre M, Verkindt H, Labreuche J, Raverdy V, Leteurtre E, Dharancy S, Louvet A, Romon M. Bariatric Surgery Reduces Features of Nonalcoholic Steatohepatitis in Morbidly Obese Patients. Gastroenterology, (2015); 149(2): 379-88; quiz e15-6.
- Calder PC. Marine omega-3 fatty acids and inflammatory processes: Effects, mechanisms and clinical relevance. Biochimical Biophys Acta, (2015); 1851(4): 469-84.
- Jump DB, Tripathy S, Depner CM. Fatty acid-regulated transcription factors in the liver. Annual Nutrition, (2013); 33: 249-69.
- Cussons AJ, Watts GF, Mori TA, Stuckey BG. Omega-3 fatty acid supplementation decreases liver fat content in polycystic ovary syndrome: a randomized controlled trial employing proton magnetic resonance spectroscopy. Journal of Clinical Endocrinology Metabolism, (2009); 94(10): 3842-8.
- Yan JH, Guan BJ, Gao HY, Peng XE. Omega-3 polyunsaturated fatty acid supplementation and non-alcoholic fatty liver disease: A meta-analysis of randomized controlled trials. Medicines, (2018); 97(37): e12271.
- He XX, Wu XL, Chen RP, Chen C, Liu XG, Wu BJ, Huang ZM. Effectiveness of Omega-3 Polyunsaturated Fatty Acids in Non-Alcoholic Fatty Liver Disease: A Meta-Analysis of Randomized Controlled Trials. PLoS One, (2016); 11(10): 0162368.
- Jump, D.B., et al., Potential for dietary ω-3 fatty acids to prevent nonalcoholic fatty liver disease and reduce the risk of primary liver cancer. Advanced Nutrition, 2015; 6(6): 694-702.
- Yu L, Yuan M, Wang L. The effect of omega-3 unsaturated fatty acids on non-alcoholic fatty liver disease: A systematic review and meta-analysis of RCTs. Pakistan Journal of Medical Sciences, (2017); 33(4): 1022-1028.
- Lytle KA, Wong CP, Jump DB. Docosahexaenoic acid blocks progression of western diet-induced nonalcoholic steatohepatitis in obese Ldlr-/- mice. PLoS One, (2017); 12(4): e0173376.
- Oscarsson J, Önnerhag K, Risérus U, Sundén M, Johansson L, Jansson PA, Moris L, Nilsson PM, Eriksson JW, Lind L. Effects of free omega-3 carboxylic acids and fenofibrate on liver fat content in patients with hypertriglyceridemia and non-alcoholic fatty liver disease: A double-blind, randomized, placebo-controlled study. Journal of Clinical Lipidology, (2018); 12(6): 1390-1403.e4.
- Masterton GS, Plevris JN, Hayes PC. Review article: omega-3 fatty acids – a promising novel therapy for non-alcoholic fatty liver disease. Alimental Pharmacological Thereapeutics, (2010); 31(7): 679-92.
- Oboodiat M, Bakhtiari R, Shakib P, Manoocheri N, Khakpour, A. The Most Important Native Iranian Medicinal Plants Affecting The Bacteria that Cause Tooth Decay; A Systematic Review. Indian Journal of Forensic Medicine & Toxicology, (2021); 15(3): 3421–3425.
- Dasarathy S, Dasarathy J, Khiyami A, Yerian L, Hawkins C, Sargent R, McCullough AJ. Double-blind randomized placebo-controlled clinical trial of omega 3 fatty acids for the treatment of diabetic patients with nonalcoholic steatohepatitis. Journal of Clinical Gastroenterology, (2015); 49(2): 137-44.
- Song Q, Chen Y, Zhao L, Ouyang H, Song J. Monitoring of sausage products sold in Sichuan Province, China: A first comprehensive report on meat species’ authenticity determination. Scientific Reports, (2019); 9(1): 1-9.
- Chen, L.H., et al., Omega-3 fatty acids as a treatment for non-alcoholic fatty liver disease in children: A systematic review and meta-analysis of randomized controlled trials. Clinical Nutrition, (2018); 37(2): 516-521.
- Dionysopoulos G, Kalopitas G, Vadarlis A, Bakaloudi DR, Gkiourtzis N, Karanika E, Tsekitsidi E, Chourdakis M. The effect of omega-3 fatty acids supplementation on pediatric patients with non-alcoholic fatty liver disease: a systematic review and meta-analysis. Clinical Nutrition Espain, (2021); 46: 54-55.
- Shapiro H, Tehilla M, Attal-Singer J, Bruck R, Luzzatti R, Singer P. The therapeutic potential of long-chain omega-3 fatty acids in nonalcoholic fatty liver disease. Clinical Nutrition, (2011); 30(1): 6-19.
- Musa-Veloso K, Venditti C, Lee HY, Darch M, Floyd S, West S, Simon R. Systematic review and meta-analysis of controlled intervention studies on the effectiveness of long-chain omega-3 fatty acids in patients with nonalcoholic fatty liver disease. Nutrition Research, (2018); 76(8): 581-602.
- de Castro GS Calder PC. Non-alcoholic fatty liver disease and its treatment with n-3 polyunsaturated fatty acids. Clinical Nutrition, (2018); 37(1): 37-55.
- Parker HM, Johnson NA, Burdon CA, Cohn JS, O’Connor HT, George J. Omega-3 supplementation and non-alcoholic fatty liver disease: a systematic review and meta-analysis. Journal of Hepatology, (2012); 56(4): 944-51.
- Jump DB, Lytle KA, Depner CM, Tripathy S. Omega-3 polyunsaturated fatty acids as a treatment strategy for nonalcoholic fatty liver disease. Pharmacology Therapeutics, (2018); 181: 108-125.
- Ghiasi S, Falahatkar B, Sajjadi M. Short- and long-term effect of feeding with flaxseed meal on biochemical parameters and plasma enzymes in cultured Siberian sturgeon (Acipenser baerii). Aquatic Animals Nutrition, )2021(; 7(1): 69-82.
- Hosseinnia E, Khara H, Farokhroz M, Yousefi Jourdehi A, Kazemi R. Effects of dietary olive oil and butyl hydroxytoluene (BHT) on digestive and hepatic enzymes, liver and intestinal histology in young Persian sturgeon, Acipenser persicus in brackish water. Aquatic Animals Nutrition, )2020(; 6(1): 27-41.
- Cansanção K. Impact of Long-Term Supplementation with Fish Oil in Individuals with Non-Alcoholic Fatty Liver Disease: A Double Blind Randomized Placebo Controlled Clinical Trial. Nutriton, (2020); 12(11): 3.
- Sangouni AA, Orang Z, Mozaffari-Khosravi H. Effect of omega-3 supplementation on fatty liver and visceral adiposity indices in diabetic patients with non-alcoholic fatty liver disease: A randomized controlled trial. Clinical Nutrition Espain, (2021); 44: 130-135
- Darvishi M, Nazer MR, Alipour MR. Investigating the end of patients suffering from diabetic foot hospitalized in Be'sat hospital of IRIAF from 2009 to 2014. Biomedical Research India, (2017); 1;28:4630-3.
- Forootan M, Tabatabaeefar M, Mosaffa N, Ashkalak HR, Darvishi M. Investigating esophageal stent-placement outcomes in patients with inoperable non-cervical esophageal cancer. Journal of Cancer, (2018);9(1):213.
- Darvishi M, Ziari K, Mohebbi H, Alizadeh K. Association between iron deficiency anemia and Helicobacter pylori infection among children under six years in Iran. Acta Medica Iranica, (2015); 220-4.
- Jalalmanesh S, Darvishi M, Rahimi M, Akhlaghdoust M. Contamination of senior medical students’ cell phones by nosocomial infections: a survey in a university-affiliated Hospital in Tehran. Shiraz E-Medical Journal, (2017); 30;18(4).
- Darvishi M, Forootan M, Nazer MR, Karimi E, Noori M. Nosocomial Infections, Challenges and Threats: A Review Article. Iranian Journal of Medical Microbiology, (2020); 10;14(2):162-81.
- Miri, M., Khandan Barani, H. Determination of aluminium bioaccumulation in liver, gill and muscle tissues of the common carp (Cyprinus carpio). Aquatic Animals Nutrition, 2017; 3(2): 1-12.
- Darvishi M. Antibiotic resistance pattern of uropathogenic methicillin-resistant staphylococcus aureus isolated from immunosuppressive patients with pyelonephritis. Journal of Pure Applied Microbiology, (2016); 1;10(4):2663-7.
- Manouchehri N. Most important medicinal plants with anti-halitosis property: An overview. Journal of Biochemical Phytomedicine, (2023); 2(1): 1–2.
- Geramizadeh B , Adeli OA, Rahsaz M, Maral Mokhtari, Sefidbakht S. Comparison of the Expression of Cell Adhesion Molecule Markers (E-Cadherin and Syndecan-1) between Young and Older Age Patients with Gastric Carcinoma. Journal of Gastrointestinal Cancer, (2010);41(3):193-6.
- Seyed-Ahmad Seyed-Alagheband SA , Sharifian M , Adeli OA, Sohooli M, Shekouhi R. Primary synovial sarcoma of thyroid gland: A case report and review of literature. International Journal of Surgery Case Report, (2021); 85: 106245.
- Seyed-alagheband SA, Shahmoradi MK, Adeli OA, Shamsi T, Sohooli M, Shekouhi R. Case Report Oncology, (2021); 14(3): 1698–1705.
- Mussavi M, Asadollahi K, Janbaz F, Mansoori E, Abbasi N. The evaluation of red reflex sensitivity and specificity test among neonates in different conditions. Iranian Journal of Pediatrics, (2014);24(6):697.
- Bahmani M, Saki K, Asadbeygi M, Adineh A, Saberianpour S, Rafieian-Kopaei M, Bahmani F, Bahmani E. The effects of nutritional and medicinal mastic herb (Pistacia atlantica). Journal of Chemical Pharmamaceutical Research, (2015);7(1):646-53.
- Karimi E, Abbasi S, Abbasi N. Thymol polymeric nanoparticle synthesis and its effects on the toxicity of high glucose on OEC cells: involvement of growth factors and integrin‐linked kinase. Drug design, Development and Therapy, (2019); 25: 2513-32.
- Sedighi M, Bahmani M, Asgary S, Beyranvand F, Rafieian-Kopaei M. A review of plant-based compounds and medicinal plants effective on atherosclerosis. Journal of Research in Medical Sciences, (2017); 22: 1.
- Abbasi N, Akhavan MM, Rahbar‐Roshandel N, Shafiei M. The effects of low and high concentrations of luteolin on cultured human endothelial cells under normal and glucotoxic conditions: involvement of integrin‐linked kinase and cyclooxygenase‐2. Phytotherapy Research, (2014);28(9): 1301-7.
- Manouchehri N. A review of the most widely used medicinal plants in the treatment of dental and oral disorders and diseases. Journal of Biochemicals and Phytomedicine. (2022); 1(1): 3–7.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


