

Full Length Research Article
Repeated Subcutaneous Granulocyte Colony Stimulating Factor Effect in Clinical Pregnancy Rate
Aseel Alfil*, Lubna Al Anbari
Adv. life sci., vol. 10, no. 4, pp. 639-643, December 2023
*- Corresponding Author: Aseel Alfil (aseelalfil@gmail.com)
Authors' Affiliations
[Date Received: 18/07/2023; Date Revised: 26/08/2023; Date Published: 31/12/2023]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: One of the most important challenges to the mother during pregnancy is the implantation of a semi-allogenic fetus. Granulocyte Colony Stimulating Factor is a polypeptide glycoprotein mainly used in hematological diseases and post-chemotherapy, but it has recently gained some popularity as an immune-modulating agent in reproductive medicine. The study aimed to define the influence of repeated subcutaneous G-CSF administration in infertile females submits to intracytoplasmic sperm injection.
Method: Ninety patients were taken from an outpatient infertility clinic and divided into two groups on the day of embryo transfer. The control group (49 patients) received no extra intervention, while the G-CSF group (41 patients) received a subcutaneous injection of G-CSF the first hour after embryo transfer, followed by weekly injections until a positive fetal heartbeat was detected.
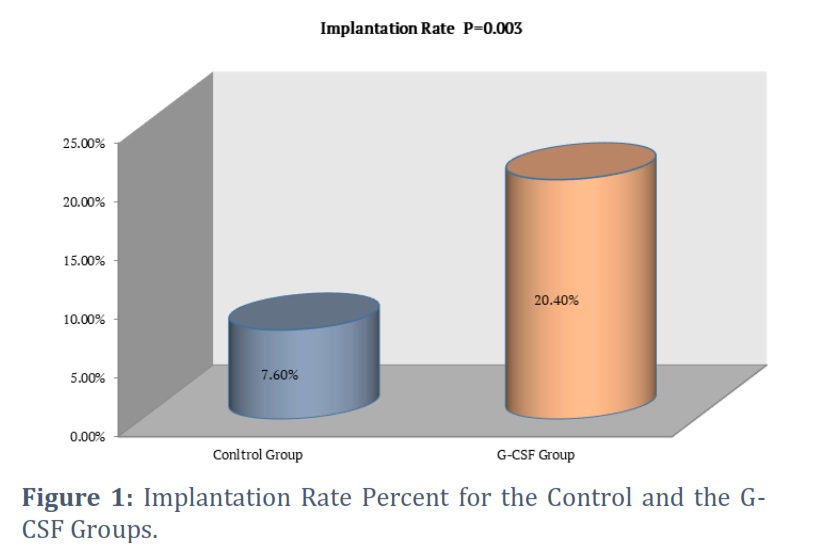
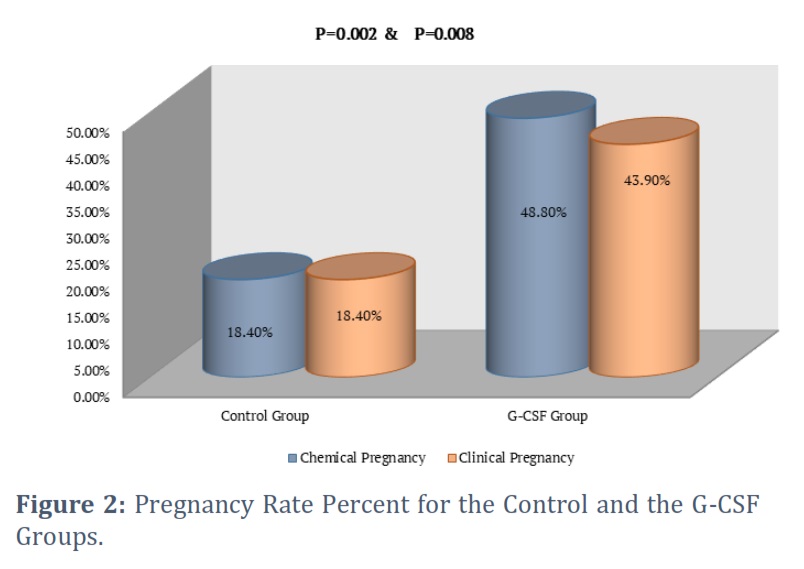
Result: In the G-CSF group, the implantation rate was 20.4% compared to 7.6% in the control. In the control group, the rates of both chemical and clinical pregnancy were 18.4%, whereas they were 48.8% and 43.9%, respectively, in the G-CSF group.
Conclusion: The multiple doses of G-CSF significantly improved the implantation and pregnancy rates, so it is considered a promising drug in reproductive medicine.
Keywords: Implantation; G-CSF; Subcutaneous; Invitro Fertilization
Introduction![]()
A zona-free blastocyst is said to have been implanted when it was attached to the endometrium and then penetrated there [1]. The period when the endometrium is best prepared for implantation is known as the “window of implantation,” and it lasts for 3-5 days, starting 6–10 days after ovulation [2]. When the endometrium reaches receptivity, one of the most significant changes is the plasma membrane’s conversion from a non-adhesive to an adhesive surface [3]. Other significant changes include the remodeling of the endometrial barrier function and the replacement of the microvilli in the apical membrane with ectoplasmic projections known as pinopodes [4]. The growing embryo will enter the uterus through the fallopian tube simultaneously. The embryo begins to produce a variety of substances in the uterus that will aid in attachment [5].
Natural synchrony is frequently lost with controlled ovarian stimulation in an IVF cycle because the stimulation parameters cause the increase in serum progesterone to occur earlier [6]. The window for implantation shifts as a result of hormonal signals that turn on the start of secretory transformation earlier than expected [7]. As a result, before the embryo reaches complete maturity, the endometrium is ready for the embryo implantation event [8].
Bone marrow cells, stromal cells, fibroblasts, macrophages, endometrial cells, and natural killer cells all produce the polypeptide glycoprotein known as granulocyte colony stimulating factor (G-CSF ) [9]. Granulocyte colony stimulating factor is secreted in the reproductive tract in three distinct manners: first, by the granulosa cells during ovulation, which promotes follicular development, steroidogenesis, and activation of leucocytes needed for ovulation [10]; second, by endometrium cells at the luteal phase, which results in vascular reconfiguration and decidualization; and third, by the placenta during pregnancy, which supports placental and embryonic development and maintains pregnancy [11]. The endometrium and the luteinized granulosa cells of the completely mature follicle exhibit increased expression of G-CSF receptors from ovulation to implantation. The content of G-CSF also increases over the same period of time in both the blood and follicular fluid [12]. From the day the embryo is transferred to the day of embryo implantation, and then again once the pregnancy is confirmed and beyond, serum levels gradually increase over the course of the gestation [13].
Granulocyte colony stimulating factor therapy has shown some promise for women with recurrent miscarriage and implantation failure [14], but further research is needed to determine the best protocol for administering it [15].
Methods![]()
Ethical Approval
The High Institute for Assisted Reproductive Technologies and Infertility Diagnosis at Al-Nahrain University was the site of the current prospective comparative study. The study comprised 90 patients who had a previous history of unsuccessful ICSI/embryo transfer rounds. All participants received detailed information regarding how to administer GCSF, and after providing written consent, they accepted to receive systemic G-CSF treatment.
Sample Size and Calculations
All participants underwent basal hormonal screening and ultrasonography on cycle day two. Gonadotropin was used to initiate ovarian stimulation, and the dosage was adjusted based on the patient's clinical characteristics (age, body mass index (BMI), and antral follicle count). Gonadotropin releasing hormone (GnRH) antagonist (Cetrotide, 0.25 mg, Merck-Serono, Switzerland) was introduced daily when the leading follicle reach a diameter of 14 mm. Estradiol measurements and transvaginal ultrasound were used to track the growth of the follicle. Oocyte pick-up took place 36 hours after human chorionic gonadotropin induced the final stage of oocytes maturation. Intra cytoplasmic sperm injection ICSI was carried out following denudation of the oocyte-cumulus complexes. Embryo transfer was done three to five days after oocyte retrieval operations. The patients were split into two groups on the day of the embryo transfer. The control group (49 females) followed the intracytoplasmic sperm injection protocol without any additional interventions, while the G-CSF group (41 females) received 300 µg of recombinant human G-CSF subcutaneous injection (Reliance®, Filgrastrim TM, Life Sciences Ltd., India) one hour after the embryo transfer and then once weekly basis until a positive fetal heartbeat will be detected. Vaginal progesterone suppositories helped with the luteal phase. Implantation rate was determined by dividing the total number of transferred embryos by the number of gestational sacs seen by transvaginal ultrasonography at the fifth week of pregnancy [12]. Measuring human chorionic gonadotropin (hCG) level in the serum was performed 14 days after fresh embryo transfer to confirm the chemical pregnancy [16]. Clinical pregnancy was assessed five weeks following embryo transfer by confirming the presence gestational sac with a positive fetal echo [17].
Immunogenicity and safety analysis
Forty-one patients received five subcutaneous doses of G-CSF and forty-nine patients did not receive any treatment out of the conventional ICSI protocol. The entire patient in both groups asked about the common side effects of G-CSF, which fever, allergy, bone pain, fatigue, headache, nausea, chest pain, dyspnea, diarrhea, and congenital abnormalities in newborns.
Statistical Analysis
The Statistical Package for Social Sciences (SPSS) version 26 was used to conduct the analysis. Categorical data were presented as means±SD and ranges while continuous data were reported as frequencies and percentages. A paired t-test with two tails was used to compare the continuous variables. Categorical variables were subjected to the Chi-square test. A P ≤ 0.05 was regarded as significant.
Results![]()
This study includes ninety patients, divided into two groups. In the control group, forty-nine patients did not receive G-CSF, and forty-one patients in the G-CSF group received five doses of G-CSF weekly from the day of embryo transfer until a positive fetal heartbeat after receiving written consent from all patients participating in the study.
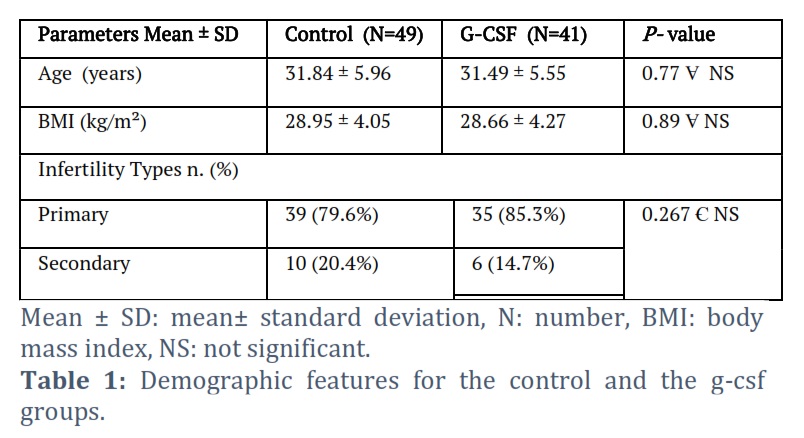
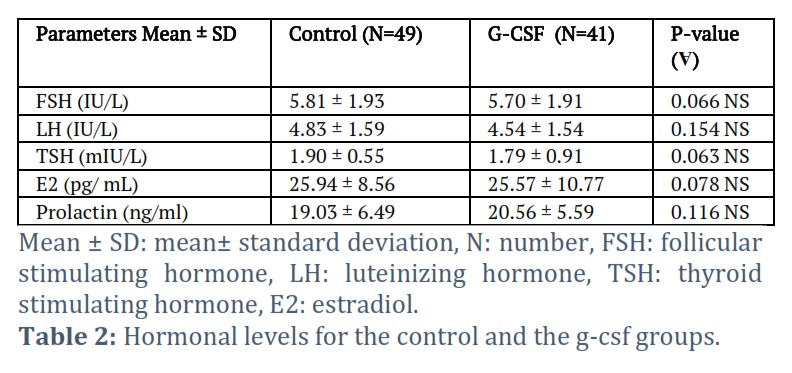
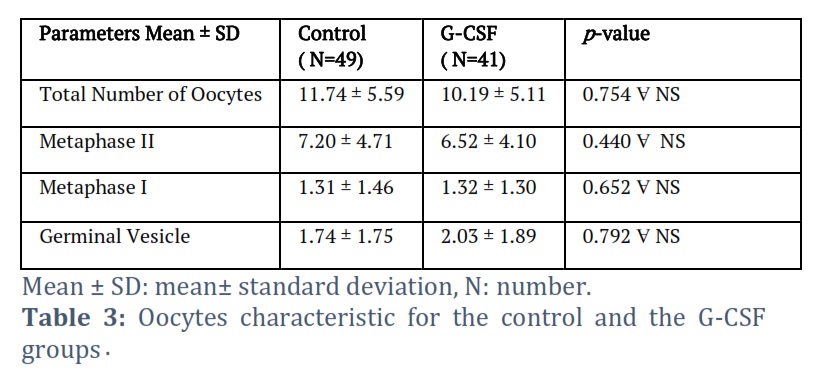
Table 1 displays the age, BMI, and infertility types of the females for the control and G-CSF groups, and as seen from (p values > 0.05), there were no significant differences between both groups. Table 2 displays the baseline hormonal level, which includes FSH, LH, TSH, E2, and serum prolactin, and as seen from the p values > 0.05, there were no significant differences between both groups. Table 3 displays the oocyte features, which are the total number of oocytes, metaphase I, metaphase II, and germinal vesical. According to p values, there were no significant differences between the control and G-CSF groups.
Figures 1 and 2 demonstrate that the G-CSF group has higher implantation and pregnancy rates (chemical and clinical), with p values equal to 0.003, 0.002, and 0.008, respectively. As seen from the p values, there were significant differences between the control and G-CSF groups.
Regarding the drug safety, only one patient in the G-CSF group developed a mild fever with the first dose of G-CSF, which was treated with a paracetamol tablet (500 mg/8 hours) orally for three days, and no fever developed with subsequent doses of G-CSF in the same patient.
Figures & Tables
The onset and maintenance of a healthy pregnancy require a number of different factors, including cytokines and chemokines [18]. Cell proliferation, immunological tolerance, and the creation of conditions for embryonic development, differentiation, and function can all be regulated by cytokines [19]. Due to the fetus’ semi-allogenic origin, pregnancy poses an immunological challenge to the mother [20]. According to Gao et al., G-CSF may play a part in the creation of adaptive changes that promote immune tolerance. It encourages the development of tolerogenic dendritic cells and regulatory T-cells that produce IL-10, which are crucial components of the immunoregulatory mechanisms that take place throughout the implantation phase [21]. Furthermore, it alters the pattern of T-cell cytokine production for Th2 responses [22]. The High Institute for Infertility Diagnosis and Assisted Reproductive Technologies has approved the trial. Signed consent was obtained from each patient receiving G-CSF. There are ninety individuals in the study: forty-nine patients in the control group and forty-one patients in the G-CSF group. Patients who get G-CSF have noticeably better chances of implantation and pregnancy; claim Zhang and his colleagues [23]. In systemic review, Liu and his associates found that giving G-CSF in multiple dosages and subcutaneously produced better results [24]. Sen and Khastgir came to the conclusion that a multiple dose of G-CSF has a more significant effect than a single dose on the rate of implantation and pregnancy [25]. These study results, which demonstrate that the G-CSF group has greater implantation and pregnancy rates (chemically and clinically), are consistent with this. Gao and his coworkers provide evidence that G-CSF helped to maintain pregnancy and decreased the rate of abortion, indicating that it might be utilized as a treatment for those who suffer repeated abortions [26]. These findings agree with the current study, which shows that the G-CSF group has a higher rate of implantation and pregnancy rates. However, G-CSF can increase implantation and pregnancy rates while having no effect on abortion rates, according to research by Torky and colleagues [27]. The use of G-CSF during fresh or frozen IVF cycles has been found to dramatically increase the rate of pregnancy, according to Miralaei and his colleague [28]. This is consistent with the findings of this study, which demonstrated significantly increased rates of pregnancy and live birth among those who got G-CSF subcutaneous injections in multiple doses. Before G-CSF can be recognized as a conventional treatment for patients with recurrent implantation failure, more research on its use and efficacy is required [22]. According to certain research, it is still unclear whether G-CSF helps patients with repeated implantation failure achieve successful implantation [29].
Only one patient in the multiple G-CSF group developed a mild fever with the first dose of G-CSF, which was treated with paracetamol tablet 500 mg/ 8 hours orally for three days, and no fever developed with subsequent doses of G-CSF in the same patient. This is consistent with the findings of Li et al., [15], who conducted a meta-analysis of six studies on the G-CSF effect in infertile females and discovered that none of the included studies mentioned any significant side effects of G-CSF and all concluded that it was a safe drug.
Multiple doses of G-CSF subcutaneous injection have been shown to improve clinical ICSI outcomes (implantation and both chemical and clinical pregnancy rates). In the field of reproductive medicine, G-CSF is regarded as a promising medication.
Author Contributions
All authors contributed equally.
The authors declare no conflict of interest.
![]() References
References
- Mascarenhas M. Management of recurrent implantation failure. Human Fertility,(2021); 25(5): 813-837.
- Sebastian-Leon P. Asynchronous and pathological windows of implantation: Two causes of recurrent implantation failure. Human Reproduction, (2018); 33(4): 626–635.
- Valdes CT, Schutt A, Simon C. Implantation failure of endometrial origin: it is not pathology, but our failure to synchronize the developing embryo with a receptive endometrium. Fertility and Sterility, (2017); 108(1): 15–18.
- Quenby S. Miscarriage matters: the epidemiological, physical, psychological, and economic costs of early pregnancy loss. The Lancet, (2021); 397(10285): 1658–1667.
- Tournaye H. Clinical performance of a specific granulocyte colony stimulating factor ELISA to determine its concentration in follicular fluid as a predictor of implantation success during in vitro fertilization. Gynecological Endocrinology, (2019); 36(1): 1–5.
- Khurshid A, Amin R, Aziz A, Ahmed O, Mahmoud E F. Deciphering the Potential Therapeutic Intervention Points of 2019-nCoV: A Pharmacological Perspective. Advancements in Life Sciences, (2022); 9(4): 412-428.
- Singal S, Sharma R, Ahuja N. GCSF in patients with thin endometrium − subcutaneous or intrauterine?. Fertility Science and Research, (2020); 7(1): 43.
- Cimadomo D. Definition, diagnostic and therapeutic options in recurrent implantation failure: an international survey of clinicians and embryologists. Human Reproduction, (2021); 36(2): 305–317.
- Aponte P, Gutierrez-Reinoso M, Sanchez-Cepeda E, Garcia-Herreros M. Differential role of r-met-hu G-CSF on male reproductive function and development in prepubertal domestic mammals. Plos one, (2019); 14(9): 222871.
- Hoff HS. Complex differential expression of colony stimulating factor (CSF) ligands and receptors in the human endometrium. Fertility and Sterility, (2016); 106(3): 11–12.
- Hou Z. What is the impact of granulocyte colony-stimulating factor (G-CSF) in subcutaneous injection or intrauterine infusion and during both the fresh and frozen embryo transfer cycles on recurrent implantation failure: a systematic review and meta-analysis?. Reproductive Biology and Endocrinology, (2021); 19(1): 1–10.
- Li J, Mo S, Chen Y. The effect of G-CSF on infertile women undergoing IVF treatment: A meta-analysis. Systems Biology in Reproductive Medicine, (2017); 63(4): 239–247.
- Wu W. Study on the protective effect of G-CSF on RIF and RA patients with low HCG level in early pregnancy. Fertility and Sterility, (2018); 110(4): 257–258.
- Kim CH, Moon J, Sungwook C, Moon S. Iintrauterine Infusion of g-csf just before Embryo Transfer may Improve the Embryo Implantation Rate Following ivf/icsi in Patients with Recurrent Implantation Failure. Fertility and Sterility, (2022); 118(4): 168–169.
- Li, J., Mo, S. and Chen, Y. The effect of G-CSF on infertile women undergoing IVF treatment: A meta-analysis. Systems Biology in Reproductive Medicine, (2017); 63(4): 239–247.
- Michikawa T. Exposure to chemical components of fine particulate matter and ozone , and placenta-mediated pregnancy complications in Tokyo. Journal of exposure science & environmental epidemiology. Journal of exposure science & environmental epidemiology, (2022); 32(1): 135–145.
- Eftekhar M, Mohammadi B, Mangoli E, Mortazavi M. Is there any correlation between estradiol supplementation, as luteal phase support, and clinical pregnancy in art cycles? A cross-sectional study. International Journal of Reproductive BioMedicine, (2020); 18(11): 969–974.
- Zilberberg E. Endometrial compaction before frozen euploid embryo transfer improves ongoing pregnancy rates. Fertility and Sterility, (2020); 113(5): 990–995.
- Mehta H M, Corey SJ. G-CSF, the guardian of granulopoiesis, in Seminars in Immunology. Elsevier, (2021); 54(1): 101515.
- Ding J. Granulocyte colony-stimulating factor in reproductive-related disease: Function, regulation and therapeutic effect. Biomedicine & Pharmacotherapy, (2022); 150: 112903.
- Vieira LA. Comparing pregnancy outcomes and loss rates in elective twin pregnancy reduction with ongoing twin gestations in a large contemporary cohort. American Journal of Obstetrics and Gynecology, (2019); 221(3): 253-e1.
- Işık G. The impact of granulocyte colony-stimulating factor (G-CSF) on thin endometrium of an animal model with rats. Gynecological Endocrinology, (2021); 37(5): 438–445.
- Zhang L. Therapeutic role of granulocyte colony-stimulating factor (G-CSF) for infertile women under in vitro fertilization and embryo transfer (IVF-ET) treatment: a meta-analysis. Archives of Gynecology and Obstetrics, (2018); 298(5): 861–871.
- Liu M. The effectiveness of immunotherapies for patients with repeated implantation failure: a systematic review and network meta-analysis, (2022); 1(1): 78-90.
- Sen U, Khastgir G. Comparative Study of The Role of Single Versus Double Dose of GCSF in Poor Endometrial Thickness Before Frozen Embryo Transfer. Bangladesh J, (2021); 1(1): 23–29.
- Gao P. G-CSF: A vehicle for communication between trophoblasts and macrophages which may cause problems in recurrent spontaneous abortion. Placenta, (2022); 121(1): 164–172.
- Torky H. Effect of intra uterine granulocyte colony stimulating factor vs. human chorionic gonadotropin at ovum pick up day on pregnancy rate in IVF/ICSI cases with recurrent implantation failure. JBRA Assisted Reproduction, (2022); 26(2): 274.
- Miralaei S. The incidence rate of unresponsive thin endometrium in frozen embryo transfer cycles: A case-series of therapy with granulocyte colony stimulating factor. International Journal of Reproductive BioMedicine, (2019); 17(12): 923.
- Banerjee K, Singla B, Verma P. Efficacy of subcutaneous granulocyte colony-stimulating factor infusion for treating thin endometrium. Clinical and Experimental Reproductive Medicine, (2022); 49(1): 70–73.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


