

Full Length Research Article
Simultaneous intratracheal administration of surfactant and budesonide in the prevention of bronchopulmonary dysplasia in the treatment of respiratory distress syndrome in premature infants
Mandana Kashaki1, Elahe Norouzi2, Arezoo Aminyan Daryasari3*, Mahsa Maleki3, Fahimeh Farhanian3
Adv. life sci., vol. 10, no. 2, pp. 304-308, June 2023
*– Corresponding Author: Arezoo Aminyan Daryasari (A.aminyan@yahoo.com)
Authors' Affiliations
2. Pediatric Growth and Development Research Center, Rasoul-e-Akram Medical Center, School of Medicine, Iran University of Medical Sciences, Tehran – Iran
3. Department of Pediatrics, Aliasghar Children's Hospital, School of Medicine, Iran University of Medical Sciences, Tehran – Iran
[Date Received: 05/03/2023; Date Revised: 15/06/2023; Date Published Online: 30/06/2023; Date Updated: 11/09/2025]
This article has changed sequence of authors from the originally published version.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Premature birth is an important issue in developing and developed countries. The purpose of this study is to investigate the effect of budesonide and surfactant in the treatment of respiratory distress syndrome and the prevention of bronchopulmonary dysplasia (BPD).
Methods: In a randomized clinical trial study, 296 premature babies with a gestational age of less than 37 weeks and weigh below 1500 grams admitted to Shahid Akbarabadi Hospital in Tehran (Iran) who were hospitalized with a diagnosis of respiratory distress syndrome and needed treatment with surfactant were included in the study. In one group (surfactant), 4 cc/kg surfactant (Beraksurf) was injected intratracheally, and in the other group (surfactant + budesonide), in addition to surfactant (Beraksurf), 0.25 mg/kg of budesonide was prescribed along with intratracheal surfactant. Descriptive statistics including Kaplan-Meier, Chi-square test and t-Student test were used for data analysis.
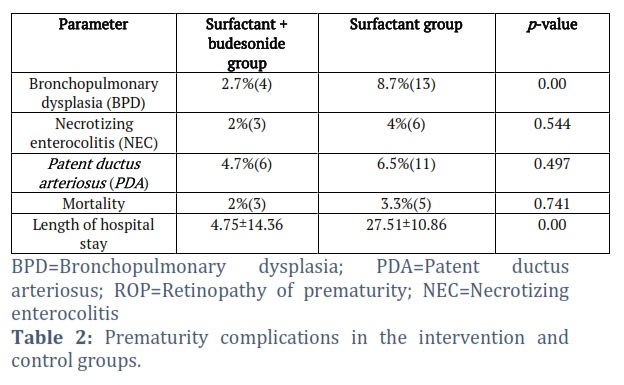
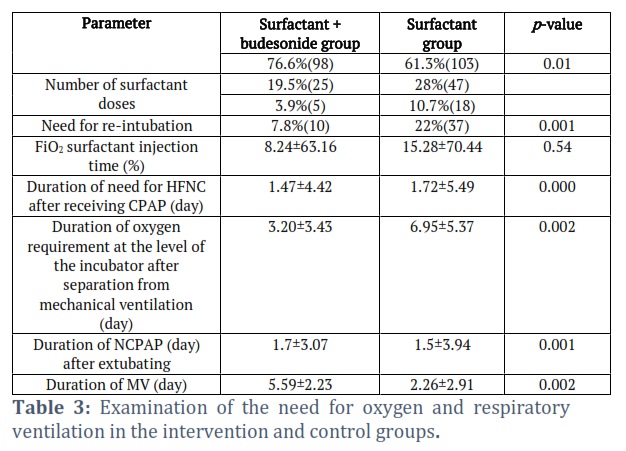
Result: In infants who were administered budesonide with surfactant through a tracheal tube, the duration of mechanical ventilation, the duration of high-flow nasal cannula (HFNC), continuous positive airway pressure (CPAP) and the need to receive peripheral equipment or through channel The nose was significantly less than the babies who received only surfactant. In the surfactant group, 13 infants (8.7%) and in the surfactant + budesonide group, 4 infants (2.7%) had bronchopulmonary dysplasia.
Conclusion: The use of the combination of surfactant (Beraksurf) with budesonide compared to surfactant alone in the treatment of premature infants significantly reduced the need for respiratory support and the need for intubation and duration of hospitalization and bronchopulmonary dysplasia.
Keywords: Budesonide; Surfactant; Premature babies; Respiratory Distress Syndrome; Bronchopulmonary dysplasia
Introduction![]()
A preterm birth is a birth that occurs before the 37th week of pregnancy [1]. The use of mechanical ventilation in the past decades for the treatment of premature infants with severe respiratory distress syndrome (RDS) led to a change in the natural pattern of the disease and as a result increased the survival probability of premature infants with lower birth weight [1]. With the increase in survival probability of very premature babies, the number of patients at risk of bronchopulmonary dysplasia (BPD) has also increased [2].
Pulmonary dysplasia (BPD) is a serious complication of the lungs that affects babies, especially premature babies. Clinically, BPD is defined as persistent respiratory distress with hypoxia, hypercapnia, and oxygen dependence for more than 4 weeks, and there is involvement of the lung parenchyma [3]. The annual mortality rate due to BPD in premature infants varies between 10% and 15%. From the point of view of pathology, the disease is in the form of progressive adhesion of alveoli and atelectasis of adjacent alveoli, interstitial edema, increased thickness of the mucous membrane and extensive hyperplasia and metaplasia of the mucous membrane of the trachea and bronchi, cyanotic skin color, rapid breathing, cough. And wheezing and difficulty in eating and vomiting are frequent [4]. Extreme weight loss and gestational age are important factors in the occurrence of BPD. Many infants with lung dysplasia have respiratory distress syndrome (RDS) [5].
Infants with pulmonary dysplasia should use nasal continuous positive airway pressure (NCPAP) or ventilator for a long time [6, 7]. Given the high prevalence of BPD and its high mortality rate, effective prevention and treatment of this disorder in infants is very important and helps to reduce the morbidity and mortality caused by it.
Currently, among the treatment methods used for respiratory distress syndrome and finally BPD include the use of intratracheal administration of surfactant, the use of NCPAP or ventilator, oxygen therapy and drugs that treat fluid accumulation in the lungs [8, 9]. But long-term use of corticosteroids causes high blood pressure, diabetes, osteoporosis, arteriosclerosis, atrophy, and depression [8, 9]. The results of recent research have shown that the use of surfactant for the remedy of RDS reduces the mortality rate but does not reduce the incidence of bronchopulmonary dysplasia [1, 2]. Studies show that lung inflammation and host responses play a major role in the pathogenesis of BPD, which is caused by chorioamnionitis, postpartum infection, tracheal intubation, and neonatal oxygen therapy. In infants with BPD, there is a possibility of long-term complications, neurodevelopmental problems, and disorders. The respiratory rate increases and the probability of hospitalization in the first year of life more than doubles [10, 11]. There are several reports of rapid recovery in lung function after the administration of corticosteroids, which makes it easier for infants to be weaned from the ventilator [12]. Anti-inflammatory compounds and corticosteroids can stimulate the secretion of surfactant, reduce bronchospasm, edema and fibrosis of the lung and reduce the response to cells and inflammatory mediators in the damaged lung [13, 14].
Due to the systemic effects of these compounds and the negative impact on the neurological development of premature infants, the use of these treatments is limited, and it is better to use inhaled steroid compounds in infants instead of using systemic steroids [15]. When surfactant is injected into the lungs of infants with RDS, a direct current is produced that can help transport drugs such as budesonide to different parts of the lung [16]. Up to one week after intratracheal injection, budesonide remains 5-10% in the lung, and if absorbed in the liver, it is rapidly metabolized to 16-alpha-hydroxyprednisolone, which has low glucocorticoid activity and a plasma half-life of 4 hours [17]. Administering intratracheal steroid together with surfactant for premature infants with RDS, in addition to reducing the side effects of systemic steroids, can have favorable effects in preventing inflammation and the occurrence of BPD [18]. Considering the inflammatory nature of BPD and the anti-inflammatory property of budesonide, the simultaneous use of surfactant with budesonide may have a more effective effect in preventing the occurrence of BPD [19]. Given the above-cited findings and arguments, the aim of this study is to investigate the effect of budesonide and surfactant in the treatment of respiratory distress syndrome and the prevention of bronchopulmonary dysplasia admitted to Shahid Akbarabadi Hospital in Tehran city, Iran.
Methods![]()
Procedure
In this double-blind clinical trial study, premature babies with a weight of less than 1500 grams and symptoms of respiratory distress syndrome and admitted to Shahid Akbarabadi Hospital in Tehran (Iran) were included in the study.
The conditions for inclusion in the study include premature babies (prematurity) with a gestational age of less than 37 weeks and a weight of less than 1500 grams, who were admitted to the NICU due to RDS based on clinical and radiological symptoms and negative blood cultures at birth;
They were subjected to CPAP in the first minutes of birth, but they did not respond to the treatment, and based on RDS Score and ABG or oxygen requirement of more than 40% with CPAP, they were candidates to receive surfactant.
Exclusion criteria include major congenital anomalies that affect the newborn's breathing (severe pulmonary hypoplasia, congenital lung anomaly, congenital airway obstruction). The presence of asphyxia (Apgar score less than 7 at the 5th minute of birth), lack of parental consent.
Sample size calculation
The sample size was calculated based on the study of Tsu F. Yeh et al. {20] given p1, 0.29 and p2, 0.50, alpha error 0.05 and statistical power of 95% at 148 for each group and 296 in total, which were divided into two intervention and control group. Parents were ensured that all their information would be kept confidential. Also, this plan was first proposed in the ethics committee of Iran University of Medical Sciences and after approval in this committee, it started with the ethics code IR.IUMS.FMD.REC.1400.165. Written informed consent was obtained from the children's parents at the beginning of the project. The information of the patients was coded.
Intervention group: simultaneous intratracheal injection of surfactant (Beraksurf with an initial dose of 4 cc per kg of weight, equivalent to 100 mg per kg of weight) and budesonide (budesonide with a dose of 0.25 mg per kg of weight from Kushan Farmed Pharmaceuticals). Control group: Surfactant injection (Beraksurf with an initial dose of 4 cc per kilogram of weight, equivalent to 100 mg per kilogram of weight from Teksima Daro Alborz pharmaceutical company)
Data analysis
Descriptive statistics including frequency, frequency percentage, mean and standard deviation and Kaplan-Meier were used for data analysis. Intention to Treat approach was also used to analyze the data. Chi-square test or its non-parametric equivalent was used to analyze qualitative variables, and t-Student test or its non-parametric equivalent was used for quantitative variables. Also, the Risk Ratio index was used to compare the incidence of BPD and death in the two study groups. Survival analysis approaches such as COX regression were used to investigate the role of each variable in the occurrence of BPD and death. Data analysis was done using SPSS version 24 given the alpha error of 5%.
Results![]()
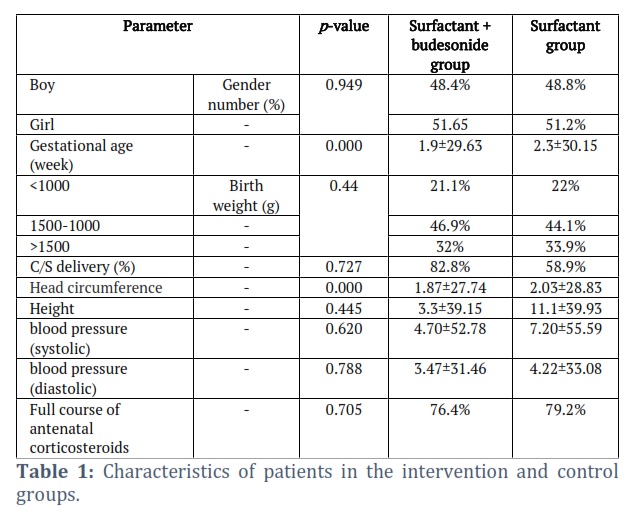
In the present study, 283 patients (95.6%) had a gestational age of less than 34 weeks, and 13 patients (4.4%) had a gestational age of 34-37 weeks. The average gestational age was obtained at 29.92±2.18 (range: 26 -35 weeks). 51.4% of babies were girls and 48.6% were boys.
In our study, 45.3% of infants weighed 1000 to 1500 g, 33.1% weighed more than 1500 g, and 21.6% weighed less than 1000 g. The results of patient characteristics, complications of prematurity and the need for oxygen and respiratory ventilation in the intervention and control groups are shown in Tables 1-3.
Figures & Tables
Discussion![]()
In the present study, gestational age and head circumference of infants were lower in the group that received budesonide, and these two variables had significant differences in the two groups. Babies with gestational age and smaller head circumference are expected to experience more incidence of BPD but given that the results were contrary to our expectations, these two variables were not considered as confounders.
In our study, BPD was defined as receiving oxygen for more than 4 weeks. The results of the present study showed that the incidence of BPD in infants who received only surfactant (Beraksurf) was 8.7% (n: 13) and in the group that received budesonide in addition to surfactant (Beraksurf) was 2.7% (4 patients), which was significantly The incidence of BPD was lower in the group receiving budesonide (p<0.05).
In a study conducted in 2021 in preterm infants, the results showed that the incidence of BPD in infants who received budesonide was 8.51% compared to 23.4% in the surfactant group, which was a significant difference, and the results of this study are consistent with our study. In our study, the duration of hospitalization, the need for re-intubation, the duration of the need for surface oxygen, HFNC, NCPAP and mechanical ventilation in the group that received budesonide was significantly less than the group that received surfactant (p<0.05).
The results of our study were consistent with other studies (2,6-8). In line with our study, it was observed in a study conducted in 2010 by Qi et al. that in the group receiving budesonide with surfactant compared to the group receiving surfactant alone, the amount of oxygen required during the first 28 days and also The duration of receiving oxygen is significantly less [21].
In a study conducted in 2008, in 116 babies weighing less than 1500 grams, in the intervention group (surfactant plus budesonide) the rate of complications and mortality was significantly lower than in the control group (surfactant) [22].
In our study, there was no significant difference in the incidence of mortality in the two groups. Consistent with our study, in a study conducted in 2016 by Nakamura et al. in the field of investigating the use of inhaled budesonide in premature infants, it was observed that the use of inhaled budesonide can lead to a reduction in the severity of BPD compared to the control group [23], which was consistent with the results of our studies.
Based on our results, the use of the combination of surfactant with budesonide compared to surfactant alone in the treatment of premature infants with low birth weight and suffering from respiratory distress syndrome significantly leads to a reduction in the need for respiratory support and Bronchopulmonary dysplasia, but it has no effect in reducing mortality or the frequency of surfactant administration. In another study, Sadeghnia et al., investigated the effect of budesonide inhalation in the prevention of chronic lung disease in premature infants [24].
The results of their investigation showed that inhalation administration of budesonide reduces the need for additional doses of surfactant. Also, inhalation administration of budesonide significantly reduces the incidence of chronic lung disease in premature infants. In the study of Heo et al., the effect of budesonide and intratracheal surfactant in preventing BPD was investigated, and the results show the positive effect of simultaneous early administration in preventing death and BPD in premature infants with severe RDS [25].
In our study, in contrast to Heo et al.'s study, although it did not show a significant relationship in the mortality rate in the two groups, the incidence of BPD was lower in the budesonide group, similar to this study. In another study, a meta-analysis conducted by Rohini et al., showed that the intratracheal administration of budesonide surfactant was associated with a reduction in the incidence of BPD and death in VLBW infants [20] and the reduction in the incidence of BPD was similar to the results of our study.The results of the study by Huang T. Kuo showed that infants in the budesonide-treated group had higher PDI and MDI scores than infants in the control group (79 ± 20 vs. 74 ± 18 and 19 ± 80 vs. 75 ± 20), but These differences were not statistically significant [26].
Based on the findings of this study, the use of the combination of surfactant (Beraksurf) with budesonide compared to surfactant (Brexorf) alone in the treatment of premature infants significantly led to a reduction in the need for respiratory support and the need for re-intubation and the duration of hospitalization and bronchopulmonary dysplasia. It is suggested to consider a larger sample size in future studies and to compare the study groups in terms of weight, development and gestational age.
Conflict of Interest
The authors state that there is no conflict of interest here.
![]()
References
- Pan J, Chen M-W, Ni W-Q, Fang T, Zhang H, Chen Y, et al. Clinical efficacy of pulmonary surfactant combined with budesonide for preventing bronchopulmonary dysplasia in very low birth weight infants, Chinese Journal of Contemporary Pediatrics, (2017);19(2): 137-41.
- Hassanzadeh-Khanmiri H, Mohammad AA, Yousif RS, Jasim SA, Kzar HH, Lafta MH, Jalil AT, Romero Parra RM, Darvishi M. SARS-CoV2 neuroinvasive potential in respiratory failure in COVID-19 patients. Caspian Journal of Environmental Sciences, (2023); 21(2): 467-472.
- Karimi M, Gholami-Ahangaran M. A Brief Report on Current Evidence of Traditional Chinese Medicine in the Treatment of Patients Infected with SARS-CoV-2. Plant Biotechnology Persa, (2021); 3 (1) :34-36.
- Minji Heo, Ga Won Jeon. Intratracheal administration of budesonide with surfactant in very low birth weight infants to prevent bronchopulmonary dysplasia. Turkish Journal of Pediatrics, (2020); 62(4):551-559. doi: 10.24953/turkjped.2020.04.004.
- Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Nature reviews Disease primers, (2001); 163:1723–1729.
- Jobe AJ. The new BPD: An arrest of lung development. Pediatrics Research, (1999);46:641–643.25.
- Bancalari E, Claure N, Sosenko IR, editors. Bronchopulmonary dysplasia: changes in pathogenesis, epidemiology and definition. Seminars in neonatology; (2003): Elsevier.
- Hallman M, Merritt TA, Akino T, Bry K. Surfactant protein A, phosphatidylcholine, and surfactant inhibitors in epithelial lining fluid. Correlation with surface activity, severity of respiratory distress syndrome, and outcome in small premature infants. American Review of Respiratory Disease, (1991); 144:1376 –1384.
- Ballard PL, Merrill JD, Godinez RI, Godinez MH, Truog WE, Ballard RA. Surfactant protein profile of pulmonary surfactant in premature infants. American Journal of Respiratory and Critical Care Medicine, (2003); 168:1123–1128.
- Smedsaas‐Löfvenberg A, Nilsson K, Moa G, Axelsson IJAP. Nebulization of drugs in a nasal CPAP system. Acta Paediatrica, (1999);88(1):89-92.
- Bassler D, Plavka R, Shinwell ES, Hallman M, Jarreau P-H, Carnielli V, et al. Early inhaled budesonide for the prevention of bronchopulmonary dysplasia. New England Journal of Medicine, (2015); 373(16):1497-506.
- Mohamed HS, Meguid MM. Effect of nebulized budesonide on respiratory mechanics and oxygenation in acute lung injury/acute respiratory distress syndrome: Randomized controlled study. Saudi Journal of Anaesthesia, (2017); 11(1): 9.
- Basu S, Kumar A, Bhatia B, Satya K, Singh TJ. Role of steroids on the clinical course and outcome of meconium aspiration syndrome—a randomized controlled trial. Journal of tropical pediatrics, (2007); 53(5):331-7.
- Festic E, Carr GE, Cartin–Ceba R, Hinds RF, Banner–Goodspeed V, Bansal V, et al. Randomized clinical trial of a combination of an inhaled corticosteroid and beta agonist in patients at risk of developing the acute respiratory distress syndrome. Critical Care Medicine, (2017);45(5):798.
- Santos AR, Heidemann SM, Walters III HL, Delius REJPCCM. Effect of inhaled corticosteroid on pulmonary injury and inflammatory mediator production after cardiopulmonary bypass in children. Pediatric Critical Care Medicine, (2007); 8(5):465-9.
- Bickel TJSM. Spreading dynamics of reactive surfactants driven by Marangoni convection. Soft Matter, (2019); 15(18):3644-8.
- Yeh TF, Chen CM, Wu SY, Husan Z, Li TC, Hsieh WS, et al. Intratracheal administration of budesonide/surfactant to prevent bronchopulmonary dysplasia. American Journal of Respiratory and Critical Care Medicine, (2016); 193(1):86-95.
- Yang CF, Jeng MJ, Soong WJ, Lee YS, Tsao PC, Tang RBJP, et al. Acute pathophysiological effects of intratracheal instillation of budesonide and exogenous surfactant in a neonatal surfactant-depleted piglet model. Pediatrics & Neonatology, (2010); 51(4):219-26.
- Cole CH, Colton T, Shah BL, et al. Early inhaled glucocorticoid therapy to prevent bronchopulmonary dysplasia. New England Journal of Medicine, (1999); 340(13):1005–1010.
- Yeh TF, Lin HC, Chang CH, Wu TS, Su BH, Li TC, et al. Early intratracheal instillation of budesonide using surfactant as a vehicle to prevent chronic lung disease in preterm infants: a pilot study. Pediatrics, (2008); 121(5): 1310-e8.
- Sadeghnia A, Beheshti BK, Mohammadizadeh M. The effect of inhaled budesonide on the prevention of chronic lung disease in premature neonates with respiratory distress syndrome. International Journal of Preventive Medicine, (2018); 9:15.
- Yeh TF, Chen CM, Wu SY, Husan Z, Li TC, Hsieh WS, et al. Intratracheal administration of budesonide/surfactant to prevent bronchopulmonary dysplasia. American Journal of Respiratory and Critical Care Medicine, (2016); 193(1):86-95.
- Rohini Venkataraman MD et al: Intratracheal Administration of Budesonide‐Surfactant in Prevention of Bronchopulmonary Dysplasia in Very Low Birth Weight Infants: A Systematic Review and Meta‐Analysis. Pediatric Pulmonology, (2017); 52(7): 23680.
- Wen JJ, Wan X, Thacker J, Garg N. Chemotherapeutic efficacy of phosphodiesterase inhibitors in chagasic cardiomyopathy. Basic to Translational Science, (2016); 1(4): 235-50.
- Minji Heo, Ga Won Jeon .Intratracheal administration of budesonide with surfactant in very low birth weight infants to prevent bronchopulmonary dysplasia. Turkish Journal of Pediatrics, (2020); 62(4): 551-559.
- Kuo HT, Lin HC, Tsai CH, Chouc IC, Yeh TF. A follow-up study of preterm infants given budesonide using surfactant as a vehicle to prevent chronic lung disease in preterm infants. The Journal of Pediatrics, (2010); 1; 156(4):537-41.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0
![]()