

Short Communication
Frequency of Helicobacter Pylori Infections and Its Associated Risk Factors in Patients Attending Tertiary Care Hospital of Bhakkar, Pakistan
Haider Nadeem, Aiman Nawaz, Arooj Nawaz, Komal Shams, Bushra Mubarak*
Adv. life sci., vol. 9, no. 3, pp. 323-327, October 2022
*– Corresponding Author: Bushra Mubarak (Email: bushra.mubarik@yahoo.com)
Authors' Affiliations
[Date Received: 22/06/2022; Date Revised: 22/08/2022; Date Published: 31/10/2022]
Editorial Note on Version of Record
24 June 2025: This article has been corrected. See https://doi.org/10.62940/als.v13i0.4239 for more information.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Helicobacter Pylori is a gram-negative bacteria that is the main cause of chronic gastritis and plays a significant role in peptic ulcers, gastric carcinoma, and gastric lymphoma. The prevalence of H. pylori cases is 75-90% worldwide. The objective of the study was to determine the frequency of H. pylori and its associated risk factors in the Bhakkar district.
Methods: A total of 102 participants with problems in the gastrointestinal tract were taken from June 2021 to May 2022. Stool antigen was performed to confirm H. pylori infection. A complete blood count (CBC) was also performed on the blood sample.
Results: The current study showed that a total of 102 samples were collected in this study. It was concluded that out of 102 participants, 63 (61.8%) were H. pylori positive and 39 (38.2%) were H. pylori-negative participants. Females were more infected with H. pylori 38 (60.3%) as compared to males 25 (39.7). The frequency of factors such as smoking (52% vs 51%), weekly consumption of junk food (52.4% vs 43.6%), fizzy drinks (33.3% vs 23.1%) and drinking of unfiltered water (54% vs 53%) was more in H. pylori-infected group compared with the uninfected group but difference was not statistically significant with odds ratio less than 1.
Conclusion: The current study concluded that female genders, ethnicities, and history of stomach infection are risk factors for H. pylori. Exposure to Smoking, unfiltered drinking water, fizzy drinks, and Junk food is more in the affected group than in the unaffected group.
Keywords: Helicobacter pylori; Stool antigen test; Risk factors; CBC
Introduction![]()
Helicobacter pylori (H. pylori), gram-negative bacteria are an inhabitant of the gastric mucosa of humans. H. pylori is the most common cause of stomach infections. 50% of the population gets infected globally with H. pylori. It was identified in 1982 by Dr. Barry Marshall and Dr. Robin Warren [1]. Self-ingestion experiments also documented that colonization of the human stomach by H. pylori leads to an inflammatory reaction in the gastric mucosa [2]. H. pylori mostly affect childhood, and it is asymptomatic most of later life. H. pylori penetrate the mucosal lining of the stomach resulting in gastrointestinal diseases mainly peptic ulcers, gastric ulcers, gastric cancer, mucosal lymphoid tissue lymphoma [MALT], and gastritis [1]. H. pylori is responsible for 80% of gastric ulcer cases. 60% of gastric ulcers lead to gastric cancer. Gastric cancer is sixth in terms of global cancer cases and second according to deaths by type of cancer. World Health Organization (WHO) has added H. pylori to the class I human carcinogen list. Screening of H. pylori at early stages helps prevent gastric cancer and peptic ulcer in most cases [3,4]. The worldwide prevalence of H. pylori is almost 50% with a relative increase in risk in underdeveloped countries [5]. The prevalence of H. pylori in Pakistan is 56-60% [6]. Prevalence fluctuates between countries and population groups within the same country. H. pylori remains highly prevalent among immigrants from countries with high prevalence in the coming decades [7]. Monitoring risk factors is very important to control the disease. Despite advancements in the medical field, infectious diseases can be disastrous claiming many lives and costing huge economic losses. H. pylori risk factors include crowded residences, low-quality food (including restaurant food or junk food), and unfiltered drinking water. People living in rural areas are highly affected because of no access to clean drinking water [8]. Poor personal hygiene and sanitary conditions are also leading to H. pylori infection. Poverty makes health care and necessary medication unaffordable for people with below-average income, as a result, they are more prone to H. pylori infections [9]. Age is also a risk factor for an increased rate of gastrointestinal diseases. H. pylori, affects children and persons above 50 years of age more, as compared to the young population.
Smoking is the most important cause of cancer worldwide. Smoking affects differently aiding H. pylori to cause infections and cancer. Instead of direct effect, smoking hinders the treatment and eradication of H. pylori and becomes a risk factor for its infections. Smoking affects metabolic activity thus in human and act as an important risk factor in case of stomach cancer. Because it contains many toxic and cancer-causing agents like nicotine and tar. More than 6000 toxic chemicals have been found in the smoke of cigarettes that affects the digestive tract and its functioning. Family history of having H. pylori infection and medication related to the digestive tract are also potential risk factors. H. pylori eradication treatment is becoming more challenging due to increasing antimicrobial resistance. Medications cause resistive patterns in H. pylori, due to which medicine to treat it proves ineffective. By keeping a check on risk factors spreading of disease can be minimized [10].
Practice good hygiene and hand washing, especially during food preparation. All patients with chronic gastrointestinal symptoms that may be associated with H. pylori infection should be tested and treated to prevent exposure to family members. Patients should complete the full course of therapy (antibiotics and acid blockers) to maximize the potential for a cure. Vaccine against H. pylori infections is in the early stages of clinical trials [11]. In the United States, Kumar S et al studied the risk factors and incidence of malignant tumors of the stomach in H. pylori-infected patients. They collected data from 371,813 patients from the Veterans Health Administration who had confirmed H. pylori infection from 1994 through 2018. The frequency of malignant growth at 5, 10, and 20 years after the recognition of H. pylori disease was 0.37%, 0.5%, and 0.65%. Patients who got therapy for the infection still had a risk of gastric cancer, but complete elimination of infection may reduce the risk of gastric cancer [12]. This study aims to find the frequency and risk factors associated with Helicobacter pylori.
Methods![]()
A descriptive observational study was conducted on 102 patients with gastric problems from DHQ hospital, Bhakkar. The study was approved by the Ethical review committee of the institute. Informed written consent was obtained from all patients during this period. The questionnaire was filled out by people who had gastric symptoms such as name, age, gender, area, smoking, consuming junk food, and diabetes, and information about signs and symptoms and modes of transmission. Patients of all age groups with symptoms such as burning sensation and severe persistent pain in the abdomen, nausea, vomiting, loss of appetite, bloating, difficulty swallowing, and weight loss were included in the study. 3ml of blood samples in an EDTA and gel vacutainer and stool samples in a dry container were collected from each patient according to standard protocol. The CBC test was performed on an automated hematology analyzer (Swelab alfa), which was made in Sweden with EDTA blood. The Accu-Tell® H. pylori kit was used for H. pylori antibodies testing in the patient’s serum separated by centrifugation of the gel vial samples. Stool samples were analyzed microscopically.
Statistical Analysis
Data entered into SPSS 23.0 (statistical package for social science, SPSS Ins., Chicago, IL, USA). For quantitative variables, mean ± standard deviation was used. Frequency and percentage were used for quantitative variables. A Chi-square test was used to find the association of factors between H. pylori positive and negative participants. The odd ratio was calculated by a logistic regression test. p-value less than 0.05 were considered statistically significant.
Results![]()
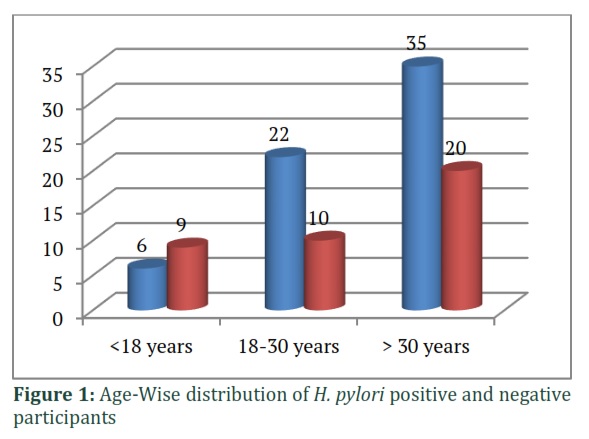
A total of 102 samples were collected in this study. Forty-Five (44%) participants were male and fifty-seven (56 %) were female. In H. pylori-infected participant (Positive cases), the female percentage (60.3%) were high than the male (39.7%) (OR: 1.68). In H. pylori-negative participants (negative group), males (51.3 %) were more prevalent than females (48.7%). The mean age of Cases was 35.60± 14.9. The mean age of negative cases (H. pylori-negative group) was 33.28±15.8 (p=0.252). Participants, more than 30 years of age were more infected with H. pylori (Figure 1). Thirty-five (55.6%) cases belong to rural areas and (44.4%) cases belonged to urban areas (OD: 1.39) (Table 1).
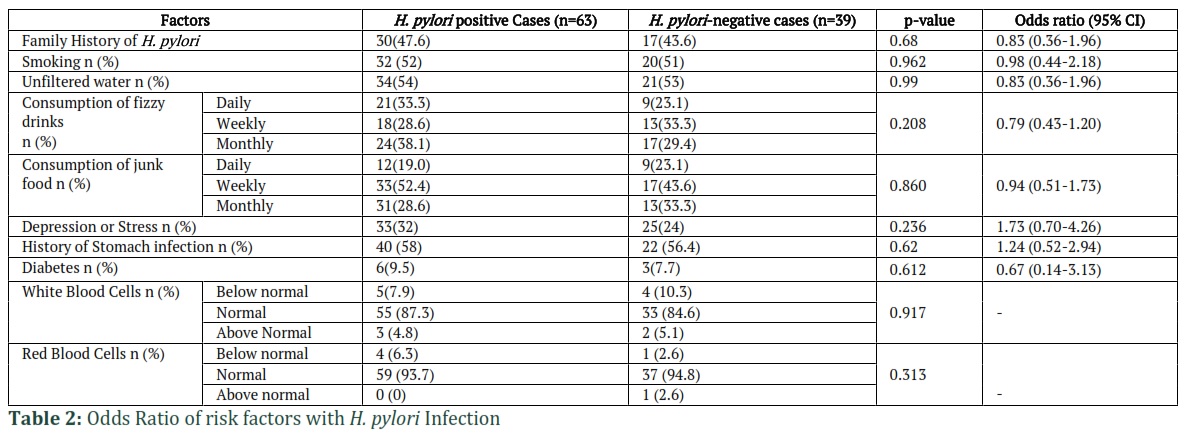
Thirty-two (52%) H. pylori-positive cases were smokers compared with H. pylori-negative cases 20 (51%) (OD=0.83). The frequency of positive cases that were drinking unfiltered water was high 34 (54.0%) as compared to negative cases 21 (53%) (OD=0.83). Participants having stress among H. pylori cases were 32 % while in negative cases, it was 24 % (OD:1.73). The frequency of positive patients consuming fizzy drinks and junk food was non-significantly high in comparison with the negative patients (33.3% vs 23.1% OD: 0.79 and 52.4% vs. 43.6% OD: 0.94 respectively. Diabetes was not significantly associated with H. pylori infection (OD: 0.67). Cases having a history of stomach infections were infected with H. pylori more frequently than the H. pylori-negative group (OD: 1.24) (Table 2). Most of the H. pylori-positive patients had normal white blood cells (87.3%) and red blood cell count (93.7%) with a non-significant difference from the H. pylori-negative group (84.6% and 94.8% respectively).
Figures & Tables

The prevalence of H. pylori varies from region to region. In the current study, 61.8% of participants were infected with H. pylori in Bhakkar. The frequency of H. pylori infection in Lahore was 7.9 % according to Sarwar et al study. This difference in frequency may be due to ethnicity differences because ethnicity is also associated with the H. pylori infection rate according to our study (OD:1.39) [13].
In the current study, patients were distributed into age groups such as under 18 years, 18-30, and above 30 years of age. The age group over 30 was the most affected group with 55.6% positive while under 18 years made 9.5% and 18-30 years was 34.9% positive. Subjects over 30 years of age were more infected with H. pylori bacteria in this study. This result is in agreement with Wawro N, et al. who reported that H. pylori infection increases with age [14].
In this current study, 52.0% of H. pylori-positive cases and 51 % of H. pylori-negative cases were smokers and smoking were not an associated risk factor with H. pylori in our study. Khalifa et al reported no statistically significant difference between smokers, non-smokers, and ex-smokers in the positivity rate of H. pylori [15].
The frequency of cases that were drinking unfiltered water was 34 (54.0%). The previous study conducted by Amara O on the association between the availability of clean water and H. pylori showed that 42.1 % of people who consume unfiltered water were infected with H. pylori [16]. Another study conducted previously by U. E. Rolle showed that out of the total, 80% of H. pylori-positive patients used contaminated water. The unfiltered water may be contaminated with H. pylori which caused infection in its consumers [17].
This study showed that in positive patients about 9.5% had diabetes while 55.9% were not diagnosed with diabetes. This showed that diabetes and H. pylori infection are not significantly related. A study conducted by Kamyar Mansori in 2020 showed that diabetic patients were 1.967 times more prone to developing H. pylori infection. H. pylori was diagnosed in 73.11% of the diabetic participants while 58.0% of non-diabetic patients [18].
About 32% of cases were stressed in our study. A previous study conducted by Takeoka in 2017 documented that there is a strong association between psychiatric disorders and H. pylori infection. Their study included 975 H. pylori-positive participants out of which 52.8% were with psychiatric disorders. 10.9% of patients who reported recurrence of infection had depression and stress while 6.2% of subjects who reported recurrence did not complain about any stress or depression [19]. A study by Zhang et al investigated H. pylori infection and associated risk factors in the general population in north-western China. They reported that the frequency of H. pylori was related to age, education level, profession, household earnings, and type of food [20]. In the Timergara community of Pakistan, smoking, snuff addiction, and regular soft drinks consumption have been linked to the increased risk of H. pylori infection [21]. An independent association between older age and increased salt consumption and H. pylori infection was found in the population of Kazakhstan. However, they reported no correlation between socioeconomic factors and H. pylori infection in the studied population [22]. CBC analysis showed a non-significant difference between the blood components of H. pylori-positive and the negative group. Bin Wahid et al have also reported that there is no difference in CBC parameters in the H. pylori-infected group [23]. The current study concluded that factors such as stress, female gender, history of stomach infection, and rural area demonstrated as risk factors for H. pylori infection. Exposure to smoking, fizzy drinks, unfiltered drinking water, and junk food was associated with H. pylori infections compared to the negative cases.
Author Contributions
Bushra Mubarak conducted the whole study from sample collection to data analysis and continuous monitoring of samples as well as wrote and edited the manuscript. Haider Nadeem and Arooj Nawaz collected and processed the samples. Komal Shams and Aiman Nawaz designed the study, searched the literature, and wrote the article.
![]()
We have read and understood ALS policy on declaration of interests and declare that we have no competing interests.
![]()
References
- McNicholl AG, O’Morain CA, Megraud F, Gisbert JP, Coordinators ASCotHEoBotN. Protocol of the European registry on the management of Helicobacter Pylori infection (Hp‐EuReg). Helicobacter, (2019); 24(5): e12630.
- Kusters JG, Van Vliet AH, Kuipers EJ. Pathogenesis of Helicobacter Pylori infection. Clinical microbiology reviews, (2006); 19(3): 449-490.
- Moayyedi P, Hunt RH. Helicobacter Pylori public health implications. Helicobacter, (2004): 11(5): 967-72.
- Khoder G, Muhammad JS, Mahmoud I, Soliman SS, Burucoa C. Prevalence of Helicobacter Pylori and its associated factors among healthy asymptomatic residents in the United Arab Emirates. Pathogens, (2019); 8(2): 44-53.
- Kuo C-H, Hu H-M, Kuo F-C, Hsu P-I, Chen A, et al. Efficacy of levofloxacin-based rescue therapy for Helicobacter Pylori infection after standard triple therapy: a randomized controlled trial. Journal of Antimicrobial Chemotherapy, (2009); 63(5): 1017-1024.
- Mehmood K, Awan AA, Muhammad N, Hasan F, Nadir A. Helicobacter Pylori prevalence and histopathological findings in dyspeptic patients. Journal of Ayub Medical College Abbottabad, (2014); 26(2): 182-185.
- Atif AB, Yasrul Izad AB, Khan M. Prevalence of Helicobacter Pylori infection in Pakistani population. Research Journal of Pharmacy and Technology, (2017); 10(12): 58-58.
- Aziz RK, Khalifa MM, Sharaf RR. Contaminated water as a source of Helicobacter Pylori infection: A review. Journal of advanced research, (2015); 6(4): 539-547.
- Kotilea K, Bontems P, Touati E. Epidemiology, diagnosis and risk factors of Helicobacter Pylori infection. Helicobacter Pylori in Human Diseases, (2019); 178(31): 17-33.
- Ferro A, Morais S, Pelucchi C, Aragonés N, Kogevinas M, et al. Smoking and Helicobacter Pylori infection: an individual participant pooled analysis (Stomach Cancer Pooling-StoP Project). European Journal of Cancer Prevention, (2019); 28(5): 390-396.
- Papastergiou V, Georgopoulos SD, Karatapanis S. Treatment of Helicobacter Pylori infection: meeting the challenge of antimicrobial resistance. World Journal of Gastroenterology: WJG, (2014); 20(29): 9898-9909.
- Kumar S, Metz DC, Ellenberg S, Kaplan DE, Goldberg DS. Risk factors and incidence of gastric cancer after detection of Helicobacter Pylori infection: a large cohort study. Gastroenterology, (2020); 158(3): 527-536. e527.
- Sarwar N, Ahmed R, Saadullah M. ullah Khan K, Kamran S, Baig FA, et al. Prevalence of Helicobacter Pylori infection and its associated diseases in low socio-economic workers in tertiary care hospital of Lahore, Pakistan. Biomedical Letters, (2019); 5(1): 1-6.
- Wawro N, Amann U, Butt J, Meisinger C, Akmatov MK, et al. Helicobacter Pylori Seropositivity: Prevalence, Associations, and the Impact on Incident Metabolic Diseases/Risk Factors in the Population-Based KORA Study. Frontiers in Public Health, (2019); 7.
- Khalifa MAAA, Abd Almaksoud A. Cigarette smoking status and Helicobacter Pylori infection in non-ulcer dyspepsia patients. Egyptian Journal of chest diseases and tuberculosis, (2014); 63(3): 695-699.
- Amaral O, Fernandes I, Veiga N, Pereira C, Chaves C, et al. Living conditions and Helicobacter Pylori in adults. BioMed research international, (2017); 17(3): 89-103.
- Rolle-Kampczyk U, Fritz G, Diez U, Lehmann I, Richter M, et al. Contaminated well water: a risk factor for Helicobacter Pylori infection. WIT Transactions on Ecology and the Environment, (2004); 77(17): 675-691.
- Mansori K, Dehghanbanadaki H, Naderpour S, Rashti R, Moghaddam AB, et al. A systematic review and meta-analysis of the prevalence of Helicobacter Pylori in patients with diabetes. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, (2020); 14(4): 601-607.
- Takeoka A, Tayama J, Kobayashi M, Sagara I, Ogawa S, et al. Psychological effects of Helicobacter Pylori ‐associated atrophic gastritis in patients under 50 years: A cross‐sectional study. Helicobacter, (2017); 22(6): e12445.
- Zhang F, Pu K, Wu Z, Zhang Z, Liu X, et al. Prevalence and associated risk factors of Helicobacter Pylori infection in the Wuwei cohort of north‐western China. Tropical Medicine & International Health, (2021); 26(3): 290-300.
- Shah SRH, Almugadam BS, Hussain A, Ahmad T, Ahmed S, et al. Epidemiology and risk factors of Helicobacter Pylori infection in Timergara city of Pakistan: A cross-sectional study. Clinical Epidemiology and Global Health, (2021): 167(21): 789-803
- Mezmale L, Polaka I, Rudzite D, Vangravs R, Kikuste I, et al. Prevalence and potential risk factors of Helicobacter Pylori infection among asymptomatic individuals in Kazakhstan. Asian Pacific Journal of Cancer Prevention: APJCP, (2021); 22(2): 597-606.
- Wahid SB, Waqar M, Rehman Z, Wasim M, Idrees M. Prevalence of HCV-Helicobacter Pylori co-infection and its effects on liver function enzymes of patients in Lahore, Pakistan. BioScientific Review, (2019); 1(3): 09-14.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0