

Full Length Research Article
Antimicrobial Compliance with CPAP in patients with obstructive sleep apnea: sleeping times with and without apparatus: A pilot study
Charles Geale1, Shahid Akhtar Akhund2*
Adv. life sci., vol. 9, no. 2, pp. 188-194, July 2022
*- Corresponding Author: Iqra Arooj (Email: akhundshahid@gmail.com)
Authors' Affiliations
2. Department of Medical Education, College of Medicine, Al-Faisal University Riyadh – Saudi Arabia
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: It has long been understood that Continuous Positive Airway Presssure CPAP adherence is not perfect in most patients, which may impact the long-term therapeutic benefits of treatment. This study aimed to investigate the sleep patterns and compliance with treatment of adults with obstructive sleep apnoea who are using CPAP and how these may affect the disease-modifying effects of CPAP.
Methods: A cross-sectional analysis of CPAP compliance in patients with moderate-to-severe OSA. The data of patients visiting regional general practice were collected by a survey.
Results: More than half (66%) of the participants recorded partial compliance with CPAP, removing the apparatus and returning to sleep without CPAP once per week or more. Most (83%) participants claimed that they were receiving four or more hours of CPAP therapy per night. For the sub-group with reduced CPAP compliance, the most significant factors which influenced use are mask discomfort (50%) and relief of daytime symptoms (63%).
Conclusion: This study demonstrated that CPAP users who met the criteria for adequate adherence to treatment may still have periods of sleep when they were exposed to disease triggering apnoeic episodes. The research in future should compare the long-term benefits of CPAP on morbidity and mortality between groups with perfect and partial compliance with treatment.
Keywords: CPAP; Sleep apnoea; Compliance
Introduction![]()
Obstructive sleep apnoea (OSA) is prevalent within the community, with moderate and severe OSA affecting an estimated 9.1% of the Australian population [1]. Risk factors for OSA include obesity, snoring, increased age, upper airway anatomical variations, and family history [2]. OSA is due to repetitive mechanical obstruction of the pharynx during sleep, preventing ventilation and gas exchange, resulting in fragmented sleep, systemic hypoxia, hypercapnia, and respiratory acidosis [3]. Apnoea are episodes of complete airway obstruction, and hypopneas are when there is partial airway obstruction. When these events last for over ten seconds and result in a 3% reduction in blood oxygen saturation, they are included in the Apnoea Hypopnea Index (AHI). The AHI is the rate of events per hour and is used to calculate the severity of OSA. Mild OSA is an AHI between 5-15/hour, moderate is between 15-25/hour, and severe is an AHI over 25/hour [4].
The effects of OSA range from the daily fatigue-related consequences of disrupted sleep to the longer-term outcomes of morbidity and mortality due to intermittent overnight hypoxemia. OSA increases the risk of developing systemic hypertension, pulmonary hypertension, coronary artery disease, heart failure, cerebrovascular disease, metabolic syndrome, atrial fibrillation, dementia, progression of some cancers, and sexual dysfunction [2,3,5-7]. A longitudinal study spanning over 18-years found 5.2 times increase in the relative risk of cardiovascular-related mortality, for persons with untreated severe OSA [8]. Despite the long-term complications of OSA, patients most commonly present to their primary care providers with the daytime symptoms of OSA: sleepiness, reduced concentration, fatigue, and low mood, or with reports from a partner who is concerned about their interrupted breathing patterns while asleep [9,10]. The Epworth Sleepiness Scale (ESS) is the industry-accepted tool for assessing daytime sleepiness and fatigue-related symptoms of OSA. A majority of OSA patients score above the normal range of 0-9, affecting their ability to drive, perform the executive function, and decision making [11].
The continuous positive airway pressure (CPAP) is used a s a primary method of treating moderate and severe OSA. The CPAP increases the air pressure inside the pharynx to maintain intraluminal dilation during muscle relaxation that occurs during sleep, preventing the collapse of the soft tissues, reducing the patient’s AHI [12]. It has been widely shown that by reducing the fragmented sleep patterns of OSA, CPAP effectively eliminates daytime sleepiness and fatigue [12,13]. Sleep physicians have previously treated patients with the assumption that CPAP’s role in the reversal of overnight hypoxemia, hypercapnia, and acidosis would also reduce the long-term complications and mortality associated with OSA. However, evidence to date has yielded inconsistent results, with larger reviews showing no changes in mortality for some patient groups [12,14-16]. Yu et al. [16] conducted a review of ten randomized control trials (RCTs) to assess changes in cardiovascular and mortality outcomes between populations with OSA treated with CPAP and control groups. The results showed no improvement in the CPAP groups for all-cause mortality (relative risk, 1.13 [95% CI, 0.99 to 1.29]; P= 0.08), with significant improvements only in sleepiness and other measures for quality of life. Four of the ten studies achieved average adherence levels of four hours per night, with the rest having average times of CPAP therapy below the accepted industry standards of adherence. Sub-group analysis of the studies with four or more hours of therapy per night still failed to show overall benefits to all-cause mortality. Guo et al. [17] also found no significant changes in mortality with the use of CPAP (odds ratio 0.85; 95% CI, 0.35-2.06; p=0.72), but did find improvements in blood pressure ( mean difference (MD) -2.03 mmHg; 95% CI -3.64 to -0.42; p=0.01) and symptoms (mean difference (MD), -1.78, 95% CI, -2.31 to -1.24; p<0.0001). They acknowledged that the use of CPAP for a longer duration may have improved outcomes.
Danish research by Jennum et al., [15] illustrates that CPAP may have a role in the reduction of mortality in specific population groups. A 17 yearlong observational study of 22,135 OSA patients compared the morbidity and mortality figures between patients treated with CPAP compared to no treatment. This study aimed to evaluate differences between men and women of different ages. No overall benefit to CPAP users was shown, however, it was found that CPAP did have a significant reduction in all-cause mortality for men over sixty years of age, once co-morbidity confounding factors were removed. These results indicate possible changes in the benefits of CPAP depending on demographics but are limited by no way of identifying what specifics about age and gender influence the results.
It is assumed that patients would use CPAP throughout their sleep time. . However, adherence to CPAP therapy has been reported as widely variable and compliance is an ongoing dilemma for clinicians and sleep researchers when assessing its long-term benefits [18]. The effectiveness of CPAP in relieving daytime symptoms could be achieved by two hours of therapy per night, leading to a reduced incentive for patients who become asymptomatic to remain compliant with CPAP for the entire night’s sleep. Other factors that have reduced compliance with CPAP include discomfort from the mask, feelings of claustrophobia, dry mouth, epistaxis, poor coping personality traits, and relief of daytime symptoms [12]. Most CPAP users have partial compliance. The adopted adherence standards in line with the patient’s recorded average daily CPAP use was 4.7 hours a night, with the accepted values for adherence reported now at 4 hours per night, on at least 70% of nights [18,19]. While this has allowed for consistency and accuracy when comparing research, authors have acknowledged that this level of CPAP adherence and compliance might be a factor reducing CPAP’s modifying effect on mortality and disease within the available data [16,20].
There is an increasing amount of research suggesting increased compliance with CPAP results in increased therapeutic benefit and a reduction of long-term complications. Outcomes for metabolic syndrome as well as cardiovascular disease are dose-dependent with improvements when participants had more than four hours of CPAP use per night and spent less time with low oxygen saturation [14,21]. A multi-centered RCT across 14 hospitals, including 723 participants, compared the incidence of blood pressure and cardiovascular events in patients with moderate to severe OSA following CPAP and those receiving no active therapy. A sub-group analysis of patients who used CPAP for more than four hours per night and spent less than 6% of time asleep with blood oxygen saturation below 90%, showed significant improvements in blood pressure and cardiovascular events. This study illustrates possible improvements with increased use, but also that residual hypoxia may have a role in limiting the therapeutic benefits of CPAP [14].
Within the existing literature, there are not many studies comparing perfect CPAP compliance with the industry-accepted four hours per night. Presumably, people using CPAP for only part of their sleep time, then return to sleep without the apparatus and experience the same level of OSA that they had before they were diagnosed and commenced treatment. This means that for the remainder of the night they are vulnerable to experiencing hypoxia, hypercapnia, and respiratory acidosis as well as a fragmented sleep cycle. While this may not be resulting in daytime symptoms for some patients, it remains unclear if this partial adherence is the reason OSA-related disease complication rates and mortality figures remain unchanged in populations receiving CPAP.
This study aimed to investigate the sleep patterns and CPAP compliance of adults with moderate and severe obstructive sleep apnoea. The time spent asleep with and without CPAP and what factors influenced reduced compliance will be measured. The research question was “what proportion of people using CPAP have periods of sleep without apparatus and what are the factors that influence this”. The expected outcomes are to validate the usefulness of the survey design and items in answering the research question; and show that people who use CPAP also spend a proportion of time asleep without apparatus/treatment and thus are still vulnerable to the effects of OSA.
Methods![]()
Study design
This study is designed to trial the usefulness and validity of the survey (appendix 1) in the assessment of CPAP adherence, which is the first of its kind to assess whether people using CPAP are also asleep for significant times without therapy. This pilot study was also used to identify trends and correlations between individuals and the characteristics of their CPAP use that can be expanded as part of a larger trial. Ethics approval for conducting the study was granted by the Human Research Ethics Committee and the University of Wollongong. To address the research question, a cross-sectional study was designed to include participants from a regional general medical practice who currently use CPAP for the treatment of OSA. Inclusion criteria: using CPAP for treatment of moderate and severe OSA
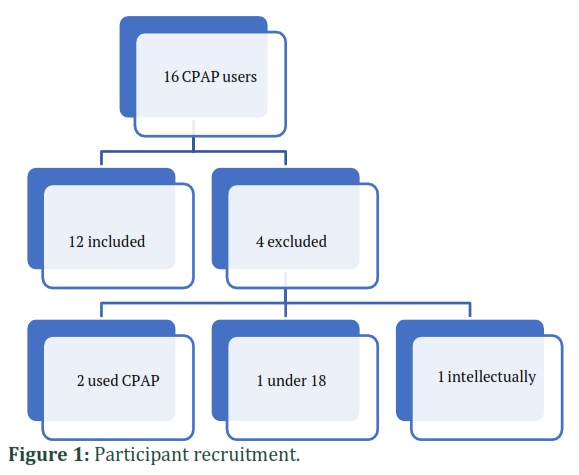
Exclusion criteria were using CPAP for less than one year; adherence less than one night a week of CPAP use; intellectual disability preventing phone survey being completed, and under age 18. Thirty-six participants were identified for inclusion from the practice medical records and were contacted by the practice nurse for recruitment into the study. Those who gave permission to be included in the study were contacted to answer the survey over the phone. All surveys were de-identified after completion to protect participant confidentiality and their anonymous status within the study.
The survey assessed the participant demographics of age and gender, allowing for characterization of CPAP use between men and women and changes in use with increasing age. Survey questions included: years using CPAP, type of CPAP mask used, whether the machine was fitted with an air humidifier, use of a chin strap, fixed or variable air pressure setting, the time they fall asleep and time they wake in the morning, whether they ever remove the CPAP mask throughout the night and return to sleep, what time do they usually remove the mask, how often per week do they remove the CPAP mask and return to sleep, and whether they sleep during the day without CPAP. To identify factors influencing reduced adherence, validated factors from a study by Sawyer et al., [18] were listed as options within the survey, including mask discomfort, claustrophobia, dry mouth, and relief of daytime symptoms.
Statistical methods
The data were entered, and analyses were conducted in the IBM SPSS version 25 statistics software. Characteristics of continuous variables were assessed using descriptive statistics, with survey results presented as mean ± standard deviation for normally distributed variables and as median ± minimum and maximum for non-normally distributed variables. Correlation analysis between demographics and CPAP adherence was assessed using the Spearman test. An r correlation coefficient of 0.7 or greater indicated a strong relationship and was used to assess links between the data groups. Results were considered statistically significant if p<0.05.
Participants
Sixteen participants were granted permission to be included in the study, of which 4 met the exclusion criteria, leaving twelve to complete the survey and be included in the analysis.
Results
![]()
Characteristics
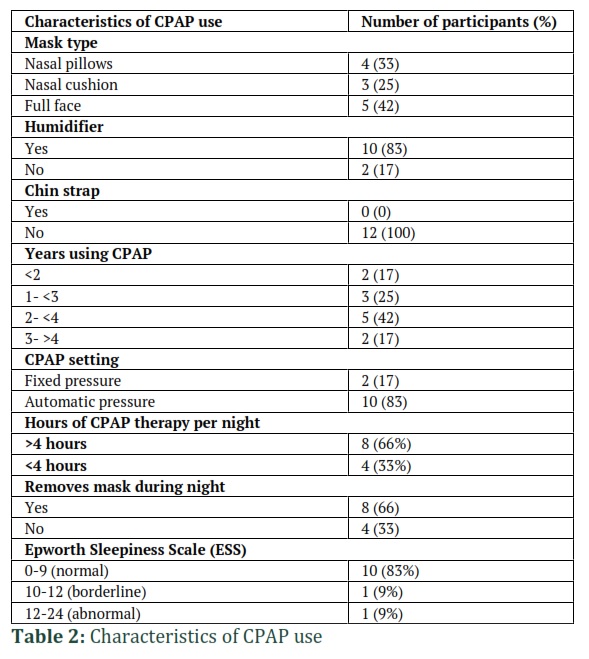
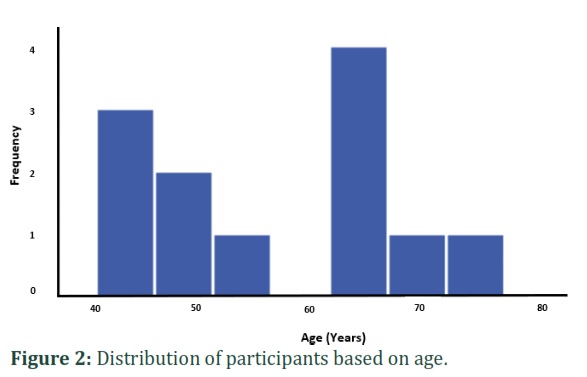
The participants had a median age of 59 years, with a peak of participants aged between 40 and 50 and a second peak between 60 and 70 (Figure 2). Participants were equally distributed between genders (Table 1). Survey results of the characteristics of CPAP (Table 2) found participants use a range of mask types, most participants (83%) use a machine with an air humidifier attached, and none of the participants used a chin strap. There was a range of time periods using CPAP between 1 year and greater than 4 years, most users (66%) use CPAP for four hours per night, and most users (66%) reported removing the mask during the night and returning to sleep. Most participants (83%) scored within the normal range for the Epworth Sleepiness Scale (ESS).
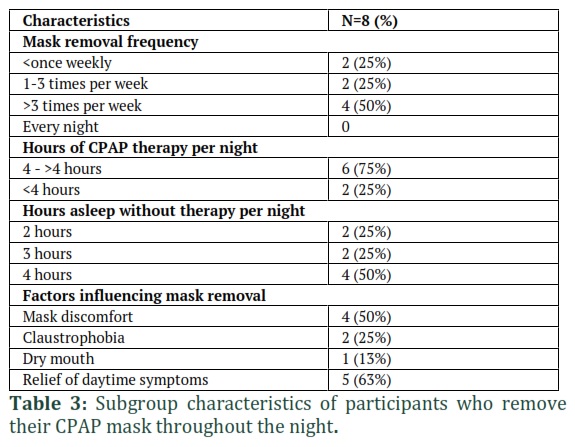
Of the subgroup of participants who reported removing their CPAP mask and returning to sleep (Table 3), fifty percent do so more than three nights per week, most (75%) use CPAP apparatus for four or more hours a night, and half report sleeping another four hours without CPAP therapy. The mask removal subgroup also reported factors that influenced removing the mask, with half (50%) claiming mask discomfort was a reason for removal, and more than half (63%) reporting that they had relief of their daytime OSA symptoms with the current usage.
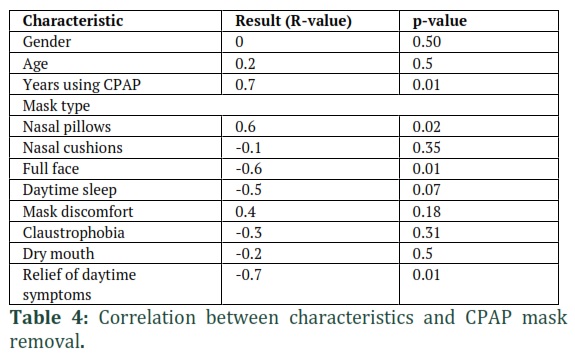
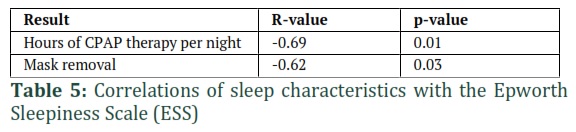
Inferential statistical tests like Spearman correlation and Chi-square were used to analyze characteristics of individual’s CPAP use and the likelihood of removing the mask throughout the night (Table 3) found no significant correlation between the participant’s gender, age, or the need for daytime sleep, and the removal of apparatus during the night. There was a strong negative relationship between the number of years using CPAP and the likelihood of removing the mask (r=0.7, p=0.01), a positive relationship between using the nasal pillows mask and removing it through the night (r=0.6, p=0.02), a negative relationship between using the full-face mask and removing the mask (r=-0.6, p=0.01), and a strong positive relationship between relief of daytime symptoms and removing the mask (r=-0.7, p=0.01). There was a moderate correlation between users who removed the mask and those with a lower ESS (r=-0.62, p=0.03) as well as a moderate negative correlation between hours of therapy and the recorded ESS (r=-0.69, p=0.01) (Table 5).
Figures & Tables

Discussion![]()
CPAP adherence and consequences
Most (66%) participants in this study use CPAP for four or more hours most nights, including most (75%) of the participants in the sub-group of participants who sleep for some of the night without using the CPAP apparatus. This is consistent with long-term data showing that adherence averages at 4.7 hours per night and is in line with the adopted industry requirements for CPAP use at four hours on 70% of nights [18,22]. These adherence requirements allow consistency between studies but are based on knowledge of how most people use CPAP, not necessarily what is required to achieve the desired therapeutic outcomes.
A meta-analysis that measures the effects of CPAP from studies that meet these standards of four hours of CPAP per night, consistently show improvements to the short-term daytime sleepiness and fatigue-related consequences of OSA but fail to show significant improvements in overall morbidity and mortality [16,17]. Therefore, the current dilemma is that clinicians don’t have an evidence-based way of reducing the risks of morbidity and mortality in their patients with OSA. It is well established that the intermittent episodes of hypoxemia related to OSA are a cause of elevated rates of cardiovascular disease, arrhythmias, and hypertension. Reduction in blood oxygen levels, along with other biochemical changes to blood-gas partial pressures, is the hypothesized link between OSA and elevated risks of metabolic syndrome, stroke, dementia, and progression of some cancers [3,23,24]. The survey used in this study cannot show that participants who remove CPAP apparatus and return to sleep have hazardous apnoeic and hypoxic episodes for the rest of the sleep period, but it is likely that once the positive pressure is removed, patients with OSA are likely to return to having the same level of disease that occurred prior to diagnosis and the commencement of treatment. This then implies that a significant number of people using CPAP, 66% in this paper, are still vulnerable to episodes of hypoxemia and the associated pathological consequences. This may be the cause of unchanged figures on disease and mortality in recent reviews and analyses of people who use CPAP [16,17].
This study found no significant correlation between age or gender and the patterns of adherence with CPAP, and equal numbers of men and women removing apparatus throughout the night. This is consistent with the findings of a review by Sawyer et al. [18], reporting that gender and age were not consistent factors for influencing adherence. Observational data finding that older males experience reductions in their mortality figures were thought to be potentially related to greater compliance with treatment, but this is in contrast to our findings which demonstrate no difference in compliance [15]. Sawyer et al. [18] did identify certain higher-risk groups within the population for reduced adherence including school-age children, patients with claustrophobia, patients who have an initial poor CPAP experience, and persons with upper limb weakness.
This study did not evaluate patients with these characteristics but did record those two (25%) participants in the subgroup with reduced adherence experienced claustrophobia from the apparatus.
The presence of daytime symptoms and mask discomfort have previously been identified as common factors for reduced CPAP compliance [18]. This is consistent with the results of this study, which shows that 50% of participants have reduced CPAP use due to mask discomfort, and 63% report relief of daytime symptoms as a factor. The ESS is a validated tool for comparing daytime symptoms of fatigue and sleepiness before and after receiving CPAP therapy [11,12]. This study found that 83% of the CPAP users scored within the normal range on the ESS and statistical analysis showed that increased time using CPAP each night correlates with a lower score on the ESS. This study was however unable to demonstrate a causative link due to the cross-sectional nature of the study, but results add to the overwhelming pool of evidence that people with OSA who are receiving CPAP treatment have low levels of daytime symptoms [12,13]. The analysis of data in this study did demonstrate a significant link between those with a low ESS and the tendency to remove the CPAP mask throughout the night as seen in table 4. All participants of this study used CPAP for at least two hours per night, and it is known from previous studies that this level can be effective in reducing patients’ ESS. It is also known that a primary motivation for receiving CPAP treatment for OSA is the desire to relieve their debilitating daytime symptoms [9,12]. It is therefore not surprising that patients who identify that they can have improvements in their quality of life without having to use CPAP all night adopt a pattern of use that matches their requirements. Non-sleepy OSA patients are therefore an important target group within the population who should be encouraged to have full compliance with CPAP therapy to achieve all the potential therapeutic benefits.
This study also found a correlation between an increased number of years since commencing CPAP and a lower rate of partial compliance with therapy. This contrasts with another study looking at predictors for reduced adherence which found time since starting therapy to be a negative predictor [19]. This study suggests that over four or more years of use, patients become less likely to remove the CPAP mask through the night, increasing the potential health and symptom benefits of greater adherence to treatment. Other predictors of increased adherence in previous data included auto-titration settings (APAP), female gender, and history of hypertension [19]. There was no statistical significance found in this study when correlating APAP to adherence or gender (as outlined above), and hypertension status was not evaluated.
Validation of the survey and limitations of the study
This pilot study will direct further expanded trials of a similar nature to assess CPAP treatment adherence and sleep patterns for patients with moderate and severe OSA. Possible errors associated with the survey include a potential sampling error by only collecting data of patients from one general practice. The small sample size in this study is another limitation and a possible source for sampling error in survey collected data [25]. While the study characterizes the behavior of CPAP patients within one practice, there is a limited capacity to extrapolate the significance of the results across the broader population. Future studies should incorporate patients from multiple practices and a variety of geographical locations.
The error of measurement is a factor for survey data, which can be reduced by using validated and reliable questionnaires that accurately reflect the nature of the topic [25]. The strengths of the qualitative components of this survey involving CPAP compliance, as well as specifics about individual’s machine settings and masks, are that they were drawn from validated questionnaires from previous research into CPAP adherence [18,19]. Another strength of this survey is using the ESS, which is an industry-standard tool for measuring sleepiness and daytime symptoms of OSA and has been validated by previously published literature [11].
Quantitative data can be less reliable when using self-reported questionnaires, due to participant recall error, truthfulness, and estimation error [25]. Self-reported times for CPAP use have previously been shown to be overestimated by approximately 1/hour [26]. CPAP devices have software to record information about use and adherence and would form more accurate data for future studies. This study was limited by not having access to software capable of analyzing data from different brands of CPAP machines. Funding for future studies would allow the purchase of the appropriate software. This study sought to demonstrate that there is a large proportion of CPAP users who have inadequate compliance with their therapy for optimal treatment. Within this sample population with moderate and severe OSA, compliance was reduced, and most participants have times of sleep when they are vulnerable to experiencing hypoxia and biochemical disturbances. These changes are known to be associated with the many complications of OSA. It has long been understood that CPAP adherence is not perfect in most patients, which may impact the long-term therapeutic benefits of treatment. The findings of this study highlight a potential flaw in the research to date that evaluates CPAP’s effectiveness in reducing morbidity and mortality because most participants are still likely to experience daily episodes of apnoea and hypoxia. Future research needs to compare patients with perfect compliance to CPAP with those whom have partial compliance and how this may affect long-term outcomes.
Author Contributions
The author declares that there is no conflict of interest regarding the publication of this paper.
References
- Simpson L, Hillman DR, Cooper MN, Ward KL, Hunter M, et al. High prevalence of undiagnosed obstructive sleep apnoea in the general population and methods for screening for representative controls. Sleep and Breathing, (2013); 17(3): 967-973.
- Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. The Lancet, (2014); 383(9918): 736-747.
- Dewan NA, Nieto FJ, Somers VK. Intermittent hypoxemia and OSA: implications for comorbidities. Chest, (2015); 147(1): 266-274.
- Manuel A, Hardinge M. Obstructive sleep apnoea. Medicine, (2012); 40(6): 287-292.
- Gottlieb DJ, Yenokyan G, Newman AB, O'Connor GT, Punjabi NM, et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the sleep heart health study. Circulation, (2010); 122(4): 352-360.
- Yang D, Liu Z, Yang H, Luo Q. Effects of continuous positive airway pressure on glycemic control and insulin resistance in patients with obstructive sleep apnea: a meta-analysis. Sleep and Breathing, (2013); 17(1): 33-38.
- Kwon Y, Koene RJ, Johnson AR, Lin G-M, Ferguson JD. Sleep, sleep apnea and atrial fibrillation: questions and answers. Sleep medicine reviews, (2018); 39134-142.
- Young T, Finn L, Peppard PE, Szklo-Coxe M, Austin D, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep, (2008); 31(8): 1071-1078.
- Farrell PC, Richards G. Recognition and treatment of sleep-disordered breathing: an important component of chronic disease management. Journal of translational medicine, (2017); 15(1): 1-12.
- Olaithe M, Bucks RS, Hillman DR, Eastwood PR. Cognitive deficits in obstructive sleep apnea: insights from a meta-review and comparison with deficits observed in COPD, insomnia, and sleep deprivation. Sleep medicine reviews, (2018); 3839-49.
- Kendzerska TB, Smith PM, Brignardello-Petersen R, Leung RS, Tomlinson GA. Evaluation of the measurement properties of the Epworth sleepiness scale: a systematic review. Sleep medicine reviews, (2014); 18(4): 321-331.
- McDaid C, Durée KH, Griffin SC, Weatherly HL, Stradling JR, et al. A systematic review of continuous positive airway pressure for obstructive sleep apnoea–hypopnoea syndrome. Sleep medicine reviews, (2009); 13(6): 427-436.
- Batool‐Anwar S, Goodwin JL, Kushida CA, Walsh JA, Simon RD, et al. Impact of continuous positive airway pressure (CPAP) on quality of life in patients with obstructive sleep apnea (OSA). Journal of sleep research, (2016); 25(6): 731-738.
- Barbé Illa F, Durán-Cantolla J, Sánchez de la Torre M, Martínez Alonso M, Carmona C, et al. Effect of Continuous Positive Airway Pressure on the Incidence of Hypertension and Cardiovascular Eventsin Nonsleepy Patients With Obstructive Sleep Apnea. JAMA, 2013, vol 307, núm 20, p 2161-2168, (2013).
- Jennum P, Tønnesen P, Ibsen R, Kjellberg J. Obstructive sleep apnea: effect of comorbidities and positive airway pressure on all-cause mortality. Sleep medicine, (2017); 3662-66.
- Yu J, Zhou Z, McEvoy RD, Anderson CS, Rodgers A, et al. Association of positive airway pressure with cardiovascular events and death in adults with sleep apnea: a systematic review and meta-analysis. Jama, (2017); 318(2): 156-166.
- Guo J, Sun Y, Xue L-J, Huang Z-Y, Wang Y-S, et al. Effect of CPAP therapy on cardiovascular events and mortality in patients with obstructive sleep apnea: a meta-analysis. Sleep and Breathing, (2016); 20(3): 965-974.
- Sawyer AM, Gooneratne NS, Marcus CL, Ofer D, Richards KC, et al. A systematic review of CPAP adherence across age groups: clinical and empiric insights for developing CPAP adherence interventions. Sleep medicine reviews, (2011); 15(6): 343-356.
- Campos-Rodriguez F, Martinez-Alonso M, Sanchez-de-la-Torre M, Barbe F, Network SS. Long-term adherence to continuous positive airway pressure therapy in non-sleepy sleep apnea patients. Sleep medicine, (2016); 171-6.
- Lamberts M, Nielsen OW, Lip GY, Ruwald MH, Christiansen CB, et al. Cardiovascular risk in patients with sleep apnoea with or without continuous positive airway pressure therapy: follow‐up of 4.5 million Danish adults. Journal of internal medicine, (2014); 276(6): 659-666.
- Stanchina ML, Welicky LM, Donat W, Lee D, Corrao W, et al. Impact of CPAP use and age on mortality in patients with combined COPD and obstructive sleep apnea: the overlap syndrome. Journal of Clinical Sleep Medicine, (2013); 9(8): 767-772.
- Engleman HM, Martin SE, Douglas NJ. Compliance with CPAP therapy in patients with the sleep apnoea/hypopnoea syndrome. Thorax, (1994); 49(3): 263-266.
- Sforza E, Roche F. Chronic intermittent hypoxia and obstructive sleep apnea: an experimental and clinical approach. Hypoxia, (2016); 499.
- Javaheri S, Barbe F, Campos-Rodriguez F, Dempsey JA, Khayat R, et al. Sleep apnea: types, mechanisms, and clinical cardiovascular consequences. Journal of the American College of Cardiology, (2017); 69(7): 841-858.
- Ponto J. Understanding and Evaluating Survey Research. Journal of the advanced practitioner in oncology, (2015); 6(2): 168-171.
- Epstein LJ, Kristo D, Strollo PJ, Jr., Friedman N, Malhotra A, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med, (2009); 5(3): 263-276.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


