

Full Length Research Article
A study on serological detection of Hepatitis A virus with associated risk factors in young kids
Aysha Iqbal Khan1, Rana Haider Ali1*, Hafiz Muhammad Usman Siddiq1, Suleman Irfan1, Noor Fatima2, Ramla Zafar3
Adv. life sci., vol. 9, no. 1, pp. 54-59, May 2022
*- Corresponding Author: Rana Haider Ali (Email: ranahaiderali94@gmail.com)
Authors' Affiliations
2. Faculty of Veterinary sciences, University of Veterinary and Animal Sciences, Lahore – Pakistan
3. Star Produce (Food processing company), Kelowna, British Columbia – Canada
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Hepatitis A virus (HAV) is a major concerning issue for human health that causes acute viral hepatitis. Hepatitis A virus is non enveloped RNA virus which is a member of the family Picornaviridae and genus Hepatovirus. HAV is more prevalent in developing countries like Pakistan with poor sanitation and economic status. The virus is present in young kids of age 1 to 15 years old associated with many risk factors.
Methods: A total of 100 blood samples (1-2 ml) were collected from the hospitals of Lahore. After serum collection, indirect ELISA was performed on a commercially available kit. The Optical density (OD) was taken from the ELISA reader. Positive and negative samples were also run along with the samples and samples OD was compared with the OD of positive and negative controls. Cut off value was calculated by multiplying negative control (NC) with 2.1. The absorbance value of specimen/cutoff <1: samples having a value less than cut-off value were considered negative and samples having a value greater than or equal to cut-off value were considered positive. The apparent prevalence of Hepatitis A virus was measured by dividing the number of children positive to the total number of children included in the study.
Results: Of the 100 samples tested, 37% were positive for IgM and 100% were positive for IgG. Statistical Analysis SPSS 21.0 version was applied to analyze the data and a correlation test was applied to see the association of risk factors with disease status.
Conclusion: This study was done to appraise the overall status of HAV prevalence in young kids in association with potential risk factors.
Keywords: Hepatitis A; ELISA; Risk assessment; Prevalence; Hygiene
Introduction![]()
Hepatitis A virus is thought to be an epidemiologically important virus that causes viral acute hepatitis worldwide [1]. HAV is responsible for infections that transfer through the feco-oral route, parenteral route, and sexual contact. Countries having intermediate endemicity level are at high risk of Hepatitis A virus infections, where HAV infection is commonly spread by direct contact with infected people and by intake of contaminated food and beverages [2]. HAV is characterized as a small, non-enveloped positive-strand RNA hepatotoxic virus comprised of family Picornaviridae and genus Hepatovirus. The geographical distribution of Hepatitis A virus is correlated with sanitary and hygiene conditions [3]. and the number of cases reported for this virus is 1.5 million each year [4]. Major studies have revealed that increasing age, poor socioeconomic status, and inappropriate hygiene conditions play an important role in the prevalence and transmission of hepatitis A virus [3]. It is estimated that if these conditions are improved worldwide, there can be a noticeable reduction in the occurrence of infection from an early age to young and even older ones [5]. This virus shows strong resistance to acidification and freezing that will increase the chances of foodborne transmission when cases of HAV infections are reported. The noticeable decrease in EU rate for HAV has been recorded over the last 15 years, despite some countries still experiencing high notification rate. We should adopt some preventive measures to control viral hepatitis such as good hygiene practices, avoiding contacting the infected person, and use of vaccines [6]. Diagnosis of HAV infection is done serologically by detecting anti-HAV-IgM and anti-HAV IgG using ELISA. This test comes positive for infected people and for those who have been vaccinated. For this purpose, HAV nonstructural protein 2A helps in the differentiation of immune status of infected and vaccinated persons [7]. High contamination concerns arise among exposed children who grow immunity without ever symptomatic in growing countries with bad sanitary infrastructure, and outbreaks are rare [8]. HAV infection is self-limiting, especially in children with developed immunity, and does not lead to chronic infections. It may intermittently evolve to severe disease, particularly among the elderly population [4]. A molecular technique such as PCR is used to determine the frequency and duration of Hepatitis A viremia in individuals with the disease [9]. The incubation period for HAV is 28 days and clinical manifestation differs. Some individuals may be asymptomatic, some show mild symptoms and others may have extreme hepatitis. HAV infection symptoms may include the abrupt onset of fever, malaise, loss of urge for food, nausea, stomach pain, and jaundice from weeks to several months [10]. Most cases of hepatitis have been reported during community wide outbreaks, the highest disease burden is reported among children, adolescents, and young adults. Countries suffering intermediate levels of disease experience an accelerated number of vulnerable adults and occasional big outbreaks [11]. The principal objective was to check the seroprevalence of Hepatitis A among children of age from one to fifteen years old and the association of various risk factors with the presence or absence of disease in children.
Methods![]()
Sample Collection and Processing
To check the seroprevalence against Hepatitis A virus, a total of 100 blood samples were collected from the hospital of Lahore and the testing of samples were done at the Institute of Microbiology, University of Veterinary and Animal Sciences, Lahore. Subjects were characterized according to three age groups ≤5 years, ≥5 years, and ≥10 years. The blood (1-2 ml) was taken in golden yellow caped serum separator tubes and remained for a short time to get the serum. The serum samples were stored at -20ᵒC for further analysis. During sampling, a questionnaire was given to parents of children to get information including age, gender, economic status, feeding habits, vaccination status, or any other disease, etc.
Serological test for detection of IgM and IgG
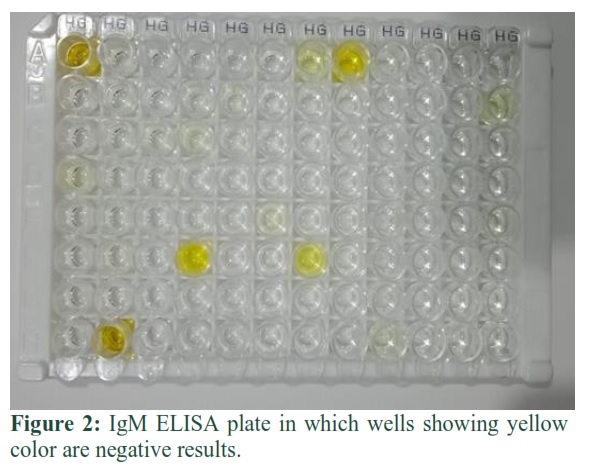
A commercially available ELISA kit was used for the detection of specific IgM and IgG antibodies against Hepatitis A virus in serum samples. IgM can be detected during the acute phase of infection [12]. Optical density (OD) values were comprehended and recorded at 450nm by iMarkTM Microplate Absorbance Reader (BIO-RAD) at serology lab in university diagnostic laboratory of UVAS, Lahore.
Results interpretation of ELISA
Cut-off value was calculated = NC × 2.1: (NC = the mean absorbance value for three negative control). Cut off value was calculated by multiplying NC with 2.1. The absorbance value of specimen/cutoff <1: Samples having value less than cut-off value were considered negative. Absorbance value of specimen/cut-off ≥1: samples having value greater than or equal to cut- off value were considered positive. Absorbance value of specimen/cut-off = 0.9-1.1: specimens having value to cut –off ratio between 0.9 and 1.1 are considered borderline.
Risk factors analysis associated with Hepatitis A infection
Risk factors analysis of Hepatitis was performed by careful analysis of the information contained in the questionnaire about the anticipated risk factors. The possible risk factors like age, sanitary conditions, economic status, vaccination status, feeding habits, quality of water were included in this study.
Statistical Analysis
The results obtained by sample analysis for detection of antibodies against Hepatitis A and the categorical measures for risk factors analysis were compiled into Microsoft Excel 16 spreadsheet. The data were analyzed through SPSS Pearson’s Chi square (x2) test was applied to analyze the association between the occurrence of Hepatitis A and its risk factors. The variables showing a significant association undergo binary logistic regression to predict the variables as a risk factor for the disease. The confidence interval was adjusted to 95%.
Results![]()
A total of 100 blood samples were taken and processed for detection of serum based prevalence of Hepatitis A through indirect ELISA. The apparent prevalence of Hepatitis was measured by dividing no of children positive to the total number of children included in the study. Of the 100 samples processed, 37% were tested positive for IgM by i-ELISA i.e. 37/100 while all samples were found positive for IgG by i-ELISA i.e. 100/100. The true prevalence was studied by the following formula given by Rogan Gladen.
True prevalence=AP+Sp-1/Se+Sp-1
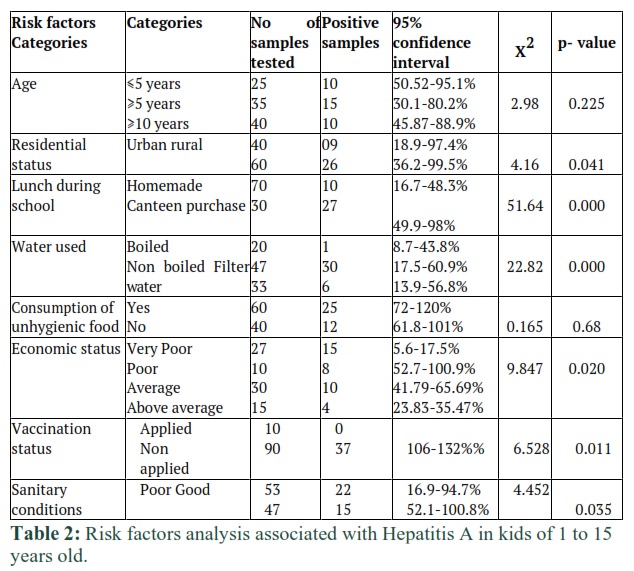
Where Sp =specificity of ELISA kit, Se = sensitivity of ELISA kit. In the current study, apparent prevalence is also the test prevalence as the specificity and sensitivity of ELISA kit for Hepatitis A is same and 100%. Of the positive 37 samples, 10 children of less than or equal to 5 years (CI 95%:50.25-95.1), 15 were of more than or equal to five years (CI: 95% 30.1-80.2%) and remaining were of more than 10 years (CI: 95% 45.87-88.9). As the infection was seen more in children of age six to ten years as the out of total positive samples 15 samples were positive (CI: 95% 30.1-80.2%). The number of children belonging to urban areas were 09 positive out of total positive samples as the (CI: 95% 18.9- 97.4) and the children belonging to rural areas were 26 positives out of total positive samples (CI: 95% 36.2-99.5) that shows that HAV was more prevalent in children belonging to rural areas. It was observed that out of 37 total positive samples, 27 were positive for children those eat canteen purchased lunch (CI: 95% 49.9-98) and remaining were of homemade lunch users. Quality of water is important in prevalence of HAV as out of total positive samples 30 samples were positive for children that drink non boiled (tap water) as (CI: 95% 17.5-60.9) and 6 samples were positive for children those drink filter water (CI: 95% 13.9-56.8) and remaining were of boiled water users. The disease was seen more seen in poor family belonging patients as out of total positive samples 15 samples were positive for children belonging to poor family status (CI: 95% 5.6-17.5), 10 samples were positive belonging to average family (CI: 95% 41.79-65.69) and rest positive samples belonging to very poor and above average family. The disease was more prevalent in non-vaccinated patients as 37 samples were positive in all non-vaccinated children. 37 samples were positive of non-vaccinated children and disease is more prevalent (CI: 95% 106-132). 22 samples were positive out of total samples tested for samples collected form children having poor sanitary conditions and HAV is more prevalent (CI: 95% 16.6-94.7). Out of total positive samples, more samples were positive for those using hygienic food from carts as 25 samples were positive (CI: 95% 72-120). Univariate analysis of HAV in children and their association to variables is shown in table 2.
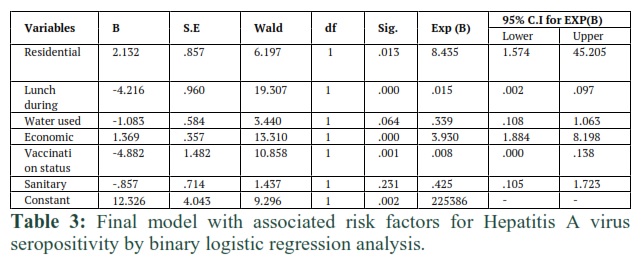
The results of Chi square analysis showed that residential status, lunch during school, water used, economic status, vaccination status, and sanitary conditions were indicated as significant factors for Hepatitis A as their p value is less than 0.05. These variables were further processed to binary logistic regression analysis. The results are shown in table 3. The final model also includes residential status, consumption of lunch and water, economic status, vaccination status, and sanitary conditions. The outcome of final model showed that odd of positivity to HAV were 8.435 times in children with residential status (CI: 95% 1.57-45.205).
Figures & Tables


Discussion![]()
Hepatitis A is an important viral disease of humans. It is caused by Hepatitis A virus which is a contagious naked nucleocapsid virus commonly present on the whole globe and is responsible for the infections that transfer through the fecal oral route. Although HAV was first successfully adapted to cell culture 20 years ago, its protein constituents have not been completely defined. Infected cells contain only low titers of virus. The P1 region encodes the three major proteins of the viral capsid, VP1, VP2, VP3. A fourth viral capsid protein VP4 essential for virion formation is not detected in mature viral particles. Each of the capsid protein is cleaved from the precursor polyprotein by the viral protease 3C, encoded in the P3 region. The native conformation of the capsid proteins VP1 and VP2 forms a single,
dominant, serologic epitope on the viral capsid and elicits a neutralizing antibody response. Nonstructural proteins encoded in the P2 and P3 regions are predicted to function in RNA synthesis and virion formation. VPG (virion protein genome linked), also encoded in the P3 region is covalently linked to the 5’ genome terminus and involved in initiation of RNA synthesis [13]. The study was carried out to assess IgM and IgG based seroprevalence of hepatitis A virus and different associated risk factors in children. The data collected indicated overall prevalence was high in children and prevalence was high in the case of IgG presence as IgG present in all serum samples. The survey gives significant proof of enormous categories of infection. Hepatitis A accounts for 50-60% of cases of kids with acute hepatitis. This infection is uncommon in adults but there is more convalescence and enhanced disease ratio in those who get affected. The children are exposed to this virus at some points of early age and continue to be immune for rest of their life. Different techniques used in detection of hepatitis A virus in different samples during acute or late phase of infection. In this study serological test ELISA (enzyme linked immunosorbent assay) was performed for the analysis of samples. As the type of sample was serum that collected from blood of children. The purpose was to find antibodies like IgM and IgG is serum that produced due to exposure of antigen in the blood. As the ELISA plate was coated with antigen against that antibodies supposed to be detected in the sample [14]. The indirect ELISA indicated high prevalence of IgG as compared to IgM because IgG persist for life time once appeared. IgM appeared after early infection and disappear after weeks and IgG produced after late infection and persist for long life and patient becomes immune for long life [15]. In comparison with the results of IgM plate and IgG, prevalence of IgM is only 37% and prevalence of IgG is 100%. The prevalence of Hepatitis A varied in case of presence of IgM and IgG antibodies. IgG antibody stays for long life in the body which may be produced as a result of vaccination. HAV does not produce long lasting infections, and the humans are natural reservoirs so the reduction in the disease can be done by maintaining high population immunity by vaccination [16]. Univariate analysis showed association of factors with positivity. Residential status, lunch during school, water, and, economic status, vaccination status and sanitary conditions are significant factors for ELISA positivity. Among all these factors lunch during school, water used are highly significant as compare to other variables. Age and consumption of unhygienic food were subjected as non-significant variables against HAV antibodies. The results of Chi square analysis showed that residential status, lunch during school, water used, economic status, vaccination status, and sanitary conditions were indicated as significant factors for Hepatitis A as their p value is less than 0.05. These variables were further processed to binary logistic regression analysis. Among all risk factors residential status, lunch during school, water quality, economic status and sanitary conditions are significant factors. Age is non-significant factor in prevalence of HAV, nevertheless almost 100% population in most regions of the developing world has been exposed to HAV by the age of 5 years [17]. Residential status plays a significant role in prevalence of HAV. 43 percent positivity was found for the children belonging to rural areas with 26 positive out of total positive samples that showed HAV was more prevalent in children belonging to rural areas. Quality of lunch and water are highly significant factors as compared to other factors. Quality of water is important in prevalence of HAV as out of total positive samples 30 samples were positive for children that drink non boiled (tap water) and 6 samples were positive for children those drink filter water and remaining were of boiled water users. This result also match with the findings of [18] that says drinking water should be properly treated to make virus free but unfortunately current water treatment strategies are unable to provide virus free effluents. This result also corporate with the study of [19] that represent in developing countries HAV is sporadic disease and as large outbreak linked with fecal contaminated drinking water. The data collected indicated overall prevalence was high in children and prevalence was high in case of IgG presence as IgG present in all serum samples. Out of total positive samples, more samples were positive for those using unhygienic food from carts as seropositivity was 41%. The result was accordance with results of [20] who also indicated that HAV is transmitted through consumption of contaminated food. The results are also in accordance with the findings of [21] that indicated that consumption of unhygienic food, raw shellfish and drinking water play an important role in prevalence of HAV infection. The results are also matched with the findings of [22] who observed that the infection could have resulted from the other contact by which feco-oral transmission can occur such as non-sexual personal contact or consumption of contaminated food. The disease was more prevalent in non-vaccinated patients as 37 samples were positive in all non-vaccinated children. Out of 100, 37 samples were positive from non-vaccinated children and disease is more prevalent in them. The results are in accordance with the results of [23] that children should be vaccinated in one to ten years of age. But vaccination is not universally implemented in most of the underdeveloped and developing countries because infection spreads often via contaminated water and food is generally asymptomatic and occur at an early age. As sanitation and living conditions improve, limited exposure of children occurs over time with HAV. The results are also in accordance with the findings of [16] who observed that IgM is the only antibody that can be detected in early phase of infection. Sanitary conditions play a key role in HAV prevalence as seropositivity was found 42% in case of poor sanitary conditions as in this study that justify with the study of [24] that reflect the trend of lower HAV infection rates in recent years is decrease which is associated with several indicators, including higher socioeconomic status as measured by the improved sanitation facilities and hygienic practices.
Indirect ELISA is good tool in diagnosis of antibodies present in serum obtained from blood sample. IgM is present at initial stage after infection and disappear after few weeks but IgG is produced at late infection and persist for long life and sample becomes positive for life and person becomes immune for long life. Various risk factors involved in prevalence of Hepatitis A virus e.g. quality of water, poor sanitary conditions, consumption of unhygienic food e.g. contaminated fruits, vegetables, under cooked foods from carts. The samples which are negative for IgM but are positive for IgG means that persons affected with Hep A once in life and remain positive for whole life.
Author Contributions
All the authors have contributed dedicatedly in terms of giving their technical expertise to give a tenable shape to this manuscript.
The Authors have declared that they have no conflict of interest.
References
- Syed R, Mohammed AH, Sindiri PK, Nathani AA, Rao RV, Satti VP, Chandra M, Khaja MN. Seroepidemiology of hepatitis A virus in Hyderabad, South India. Journal of Medical & Allied Sciences, (2012); 2(2): 58.
- Bonanni P, Boccalini S, Bechini A. Vaccination against hepatitis A in children: A review of the evidence. Therapeutics and Clinical Risk Management, (2007); Dec;3(6):1071.
- Ciaccia MC, Moreira RC, Ferraro AA, Lemos MF, Oba IT, Porta G. Epidemiological and serological aspects of hepatitis A among children and teenagers in the city of Santos: a cross-sectional study. São Paulo Medical Journal, (2012);130(4):230-5.
- Ayouni, K., Naffeti, B., Ben Aribi, W. et al. Hepatitis a virus infection in Central-West Tunisia: an age structured model of transmission and vaccination impact. BMC Infectious Disease (2020); 20, 627.
- Lemon, Stanley M., and David L. Thomas. "Vaccines to prevent viral hepatitis." New England journal of medicine 336.3 (1997): 196-204.
- European Food Safety Authority (EFSA). Update: Outbreak of Hepatitis A virus infection in Italy and Ireland (2013); (Vol. 10, No. 7, p. 459E).
- Bohm K, Filomena A, Schneiderhan-Marra N, Krause G, Sievers C. Validation of HAV biomarker 2A for differential diagnostic of hepatitis A infected and vaccinated individuals using multiplex serology. Vaccine, (2017); Oct 13;35(43):5883-9.
- Hofmeister, Megan G., Monique A. Foster, and Eyasu H. Teshale. "Epidemiology and transmission of hepatitis A virus and hepatitis E virus infections in the United States." Cold Spring Harbor perspectives in medicine 9.4 (2019): a033431.
- Bower, William A., Omana V. Nainan, Xiaohua Han, and Harold S. Margolis. "Duration of viremia in hepatitis A virus infection." The Journal of infectious diseases 182, no. 1 (2000); 12-17
- Steffen, Robert, Mark A. Kane, Craig N. Shapiro, Nils Billo, K. Janine Stellhorn, and Pierre van Damme. "Epidemiology and prevention of hepatitis A in travelers." Jama 272, no. 11 (1994); 885-889.
- Staes, C.J, Schlenker, T.L, Risk, I., Cannon, K.G, Harris, H., Pavia, A.T, Shapiro, C.N, Bell, B.P. Sources of infection among persons with acute hepatitis A and no identified risk factors during a sustained community-wide outbreak. Pediatrics. (2000); 106(4): e54-e54.
- Locarnini SA, Coulepis AG, Stratton AM, Kaldor JA, Gust ID. Solid-phase enzyme-linked immunosorbent assay for detection of hepatitis A-specific immunoglobulin M. Journal of Clinical Microbiology, (1979); Apr;9(4):459-65.
- Pintó RM, Pérez-Rodríguez FJ, D’Andrea L, de Castellarnau M, Guix S, Bosch A. Hepatitis A virus codon usage: implications for translation kinetics and capsid folding. Cold Spring Harbor perspectives in medicine, (2018); Oct 1;8(10): a031781.
- Coulepis, A. G., S. A. Locarnini, N. I. Lehmann, and I. D. Gust. "Detection of hepatitis A virus in the feces of patients with naturally acquired infections. Journal of Infectious Diseases 141, 2 (1980); 151-156.
- Møller, A. M., and L. R. Mathiesen. "Detection of immunoglobulin M antibodies to hepatitis A virus by enzyme-linked immunosorbent assay." Journal of clinical microbiology 10, no. 5 (1979); 628-632.
- Mao S, Ou X, Zhu D, Chen S, Ma G, Wang M, Jia R, Liu M, Sun K, Yang Q, Wu Y. Development and evaluation of indirect ELISAs for the detection of IgG, IgM and IgA1 against duck hepatitis A virus 1. Journal of virological methods, (2016); Nov 1;237:79-85.
- Shah U, Habib Z. Liver failure attributable to hepatitis A virus infection in a developing country. Pediatrics, (2000); Feb 1;105(2):436-8.
- Thébault A, Le Saux JC, Pommepuy M, Guyader SL, Lailler R, Denis JB. Quantitative approach of risk management strategies for hepatitis A virus–contaminated oyster production areas. Journal of food protection, (2012); Jul;75(7):1249-57.
- Hofmeister MG, Foster MA, Teshale EH. Epidemiology and transmission of hepatitis A virus and hepatitis E virus infections in the United States. Cold Spring Harbor perspectives in medicine, (2019); Apr 1;9(4): a033431.
- Sattar SA, Tetro J, Bidawid S, Farber J. Foodborne pread of hepatitis A: Recent studies on virus survival, transfer and inactivation. Canadian Journal of Infectious Diseases, (2000); May 1;11(3):159-63.
- Mele A, Stroffolini T, Palumbo F, Gallo G, Ragni P, Balocchini E, Tosti ME, Corona R, Marzolini A, Moiraghi A, SEIEVA Collaborating Group. Incidence of and risk factors for hepatitis A in Italy: public health indications from a 10-year surveillance. Journal of hepatology, (1997); Apr 1;26(4):743-7.
- Cotter SM, Sansom S, Long T, Koch E, Kellerman S, Smith F, Averhoff F, Bell BP. Outbreak of hepatitis A among men who have sex with men: implications for hepatitis A vaccination strategies. The Journal of infectious diseases, (2003); Apr 15;187(8):1235-40.
- Brundage SC, Fitzpatrick NA. Hepatitis A. American family physician, (2006); Jun 15;73(12):2162-8.
- Sa-nguanmoo P, Posuwan N, Vichaiwattana P, Vuthitanachot V, Saelao S, Foonoi M, Fakthongyoo A, Makaroon J, Srisingh K, Asawarachun D, Owatanapanich S. Declining trend of hepatitis A seroepidemiology in association with improved public health and economic status of Thailand. PLoS One, (2016); Mar 23;11(3): e0151304.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


