

Full Length Research Article
Thyroid Dysfunction and Vitamin D Deficiency among Females of Punjab, Pakistan; A Cross Sectional Analysis
Jamil Ahmad1*, Altaf Hussain2, Lubna Humayun3, Muhammad Ahtisham Azhar4, Fariha Zafarullah5, Irfan Ullah4, Jamal Shah6
Adv. life sci., vol. 9, no. 1, pp. 75-79, May 2022
*- Corresponding Author: Jamil Ahmad (Email: jamilahmad2424@gmail.com)
Authors' Affiliations
2. Saidu Group of Teaching Hospital, Swat- Pakistan
3. Department of Pathology, University College of Medicine and Dentistry University of Lahore, Lahore – Pakistan
4. Faculty of Allied Health Sciences University of Lahore, Lahore – Pakistan
5. Sargodha Medical College, Sargodha – Pakistan
6. Armed Forces Institute of Pathology, Rawalpindi – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Thyroid gland is an important gland which plays a vital role in the stimulation of normal growth and central nervous system (CNS), metabolism regulation, elevated vitamin requirements, metabolism of phosphorus and calcium, promote sexual metabolism, increases mitochondrial metabolism, stimulates the adrenergic activity with myocardial contractility and increase heart rate. In this era, one of the important health issues is vitamin D and calcium deficiency. A large number of populations in all over world are vitamin D or calcium deficient or insufficient. The objective of this study was to evaluate the prevalence of thyroid dysfunction and vitamin D deficiency in females.
Methods: A cross sectional study was designed to check the prevalence of thyroid disease and its correlation with vitamin D levels in females. Venous blood was drawn from the female’s patients (11—80 years of age) using gel disposable vials (3.5 ml) in aseptic condition. Samples were centrifuged at four thousand revolutions per minute for five minutes and serums were separated. After the separation of serum, the samples were transferred to the laboratory for the automated estimation of Thyroid Stimulating Hormone (TSH), Triiodothyronine (T3), Thyroxine and Vitamin D.
Results: It was observed that out of 79 females who had gone through thyroid profile testing, 70% females had normal thyroid profile. However, hypothyroidism was found in 23% females and 7% females had the condition of hyperthyroidism. Out of 18 (23%) reported cases of hypothyroidism, 8 cases were of mild (subclinical) hypothyroidism, 3 cases indicated non-thyroidal illness; rare pituitary hypothyroidism. Out of 79 female participants, only 20 (25.31%) females had normal serum vitamin D levels. Overall, 59 (74.68%) females had vitamin D deficiency. When the vitamin D deficiency was correlated with thyroid dysfunction, it was observed that vitamin D levels were non-significantly (p = 0.35) associated with hypothyroidism.
Conclusion: Hypothyroidism was found prevalent in the tested female population, as 23% of the tested population had hypothyroidism while 9% of them have hyperthyroidism. Moreover, majority of the population had vitamin D deficiency.
Keywords: Thyroid Dysfunction; Vitamin D Deficiency; Females
Introduction![]()
Thyroid gland is situated among C5 and T1 vertebrae in front of the neck. Thyroid gland is present below the sternohyoid, platysma, and sternothyroid muscles. The weight of thyroid is about 15 to 20 grams. In females, the weight of thyroid is less as compared to males. In infants, weight of thyroid is about 1g. As the age increases, the weight of thyroid increases approximately 1g. Thyroid gland is a bilobed, red colored, delicate, H shaped, parenchymal structure. Both lobes of thyroid gland are about 4cm long, 2cm wider and about 2 to 3cm broad. Isthmus is about 2cm long, 2 to 6 mm broad, and 2 cm wider [1].
Thyroid gland consists of two lobes and the right lobe of thyroid gland is larger as compared to the left lobe and these lobes are linked together by isthmus. The secretory unit of thyroid gland is known as acinus or thyroid follicle. The outer layer of each follicle has epithelial cells and amorphous material known as colloid and is enclosed with epithelial cells and is made up of thyroglobulin (Tg). In colloid near the surface of epithelial cells some important reactions such as, formation of thyroid hormone like iodination and secretion of hormones take place. Thyroid gland also consists of C cells or parafollicular cells. These cells produce calcitonin, which is a polypeptide hormone. These cells are only present within the basement lamina or is present in form of clusters with in the interfollicular spaces [2].
Thyroid gland is an important gland which plays a vital role in the stimulation of normal growth and central nervous system (CNS), metabolism regulation, elevated vitamin requirements, metabolism of phosphorus and calcium, promote sexual metabolism, increases mitochondrial metabolism, stimulates the adrenergic activity with myocardial contractility and increase heart rate [2]. In this era, one of the worldwide health issue is vitamin D and calcium deficiency. A large number of populations in all over world is vitamin D or calcium deficient or insufficient [3].
Thyroid gland involves two conditions, hypothyroidism and hyperthyroidism. Hypothyroidism is the decrease in thyroid hormone production and secretion. This common disorder occurs in both forms mild and severe in 2% and 15% populations. Men are less affected than women and with the increase in age both gender affects more frequently. Many abnormalities in the functioning and structure of thyroid gland leading to the deficiency of thyroid hormone [2].
Vitamin D plays a vital role in health, specifically for the strengthening of healthy bones. It is also important for the proper functioning of the organs such as lungs, heart, muscles and brain. It boosts the immune system to fight against infectious organisms. Body gets its vitamin D from exogenous sources. It is converted from inactive vitamin D into a hormone called activated vitamin D or calcitriol. Vitamin D is also essential to absorb minerals such as phosphorus and calcium (4). The normal vitamin D level ranges from 30 to 100 ng/ml. The vitamin D level ranging from 20 to 29 ng/mL is deliberated deficient, if vitamin D level is <12 ng/ml, it is measured to be an indication of critical insufficient level of vitamin D. The circulating thyroid hormone and vitamin D are attached on identical receptors called steroid hormone receptors [5].
A couple of mechanisms describe the decreased vitamin D level in hypothyroid condition. One of these mechanisms is the malabsorption of vitamin D in the intestine and other one is that the incomplete activation of vitamin D. Low vitamin D levels was observed in patients suffered with Grave’s disease. Vitamin D status and malabsorption of vitamin D in the intestine can affect the onset or development of many autoimmune diseases. Furthermore, vitamin D supplementation play a vital role in the prevention of several autoimmune diseases in individuals [6].
Vitamin D level does not directly affect thyroid hormone level leading to hypothyroidism or hyperthyroidism. Immuno-regulation appears to be a more realistic explanation for this phenomenon. Vitamin D in the regulation of cytokines, for example interleukin IL-6, IL-17, (IL)-1, and tumor necrosis factor (TNF-α) play a vital role in autoimmune thyroid disease (AITD). Statistical analysis shown that the onset of postpartum thyroiditis (PPT) is associated lower serum vitamin D level. Vitamin D deficiency is a possible cause in the progress of AITD, but it did not correlate with the titers of thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TgAb) and nor with the levels of thyroid hormones [6]. Thyroid reactive antibodies (TRAb) titer in GD is fluctuated with vitamin D level; the highest vitamin D level are involved in the development of AITD. Vitamin D does not have strong relationship with the titers of thyroid antibodies in GD patients [7].
A different gene has been found in the Vitamin D receptor. It indicated that people are susceptible to Hashimoto thyroiditis and Grave’s disease. Vitamin D bind with the vitamin D receptor (VDR) and induced its effect and activated the VDR-responsive genes. Although, autoimmune thyroid diseases (AITDs) could be associated with VDR gene polymorphism [8].
The frequency of vitamin D deficiency has been considerably greater in patients suffered with AITDs as compared to healthy persons. Vitamin D deficiencies are associated with the increased incidence of autoimmune diseases, including rheumatoid arthritis and systemic lupus erythematosus, type I diabetes mellitus (T1DM) [8]. Latitude differences play a role in several autoimmune diseases. The incidence of multiple sclerosis (MS) is decreased as vitamin D level increased; the risk of multiple sclerosis is less in sunny areas. The incidence of type 1 diabetes mellitus (T1DM) has direct relation with latitude. It indicated that the less exposure of sun and the less intake of vitamin D supplements in early age, it cause greater risk of type 1 diabetes mellitus (T1DM) [8]. Stimulation of experimental autoimmune thyroiditis can be prevented by vitamin D supplementation and cyclosporine. Variation in thyroid function according to demographic characteristics was also observed. The dominant T-lymphocyte infiltration of the thyroid gland is characterized the Hashimoto’s thyroiditis and Graves’ disease [9].
Another reasonable explanation is that increased calcium loss from bones in hyperthyroid patients. It led to raised plasma calcium level, activated vitamin D synthesis and parathyroid hormone are does not effected by altered calcium level. The relation between hypothyroidism and vitamin D is stronger than hyperthyroidism. However, vitamin D deficiency has a primary role in the occurrence of thyroid dysfunction [10]. The objective of this study was to check the prevalence of thyroid dysfunction and vitamin D deficiency in females.
Methods![]()
A cross sectional study was designed to check the prevalence of thyroid disease and its correlation with vitamin D levels in females. The study was carried out at the University of Lahore Teaching Hospital, Lahore, Punjab. The study duration was from November 2019 to February 2020. Female patients with thyroid dysfunction were included in this study. Children and male patients were excluded from this study.
LABORATORAY ANALYSIS
Venous blood was drawn from patient in gel disposable vials (3.5 ml) in aseptic condition. Each sample was centrifuged at four thousand revolutions per minute for five minutes and serums were separated. After the separation of serum, the samples were transferred to the laboratory. Collected specimens were analyzed within 12 hours of collection by using electrochemiluminescence immunoassay (Roche Diagnostics, Indianapolis, Germany).
STATISTICAL ANALYSIS
All pertinent clinical and laboratory information were entered to SPSS version 25.0. categorical data were analyzed using Chi Square test (degree of freedom = 0.5).
Results![]()
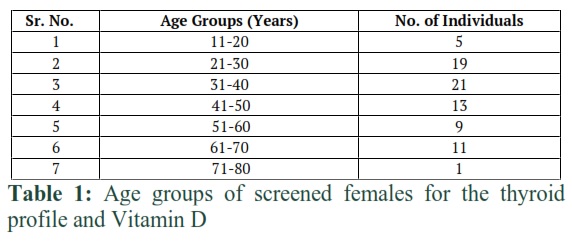
In the present study, females were screened for thyroid profile and their vitamin D level was also measured. Blood samples were obtained from 79 individuals (females) for the estimation of thyroid profile and vitamin D level. Patients were divided into seven age groups. Group 1 (11-20yrs), group 2 (21-30yrs), group 3 (31-40yrs), group 4 (41-50yrs), group 5 (51-60yrs), group 6 (61-70yrs) and group 7 (71-80yrs).
Out of total screened females, the TSH level was lower than 0.4 µIU/ml in 5 females (6.329%), however normal TSH level was observed in 59 females (74.68%). On the other hand, abnormally high level of TSH was recorded in 15 females (18.98%). When T3 level was tested, it was observed that out of 79 females, 75 (95%) females had normal T3 level however, 4 females (5%) had high level of T3. Decreased level of T3 was not observed in any case. When T4 levels of the selected female population was tested, it was found that 6 females (7.59%) had low level of T4, 57 females (72.1%) females had normal, and 16 females (20.25%) had high level of T4.
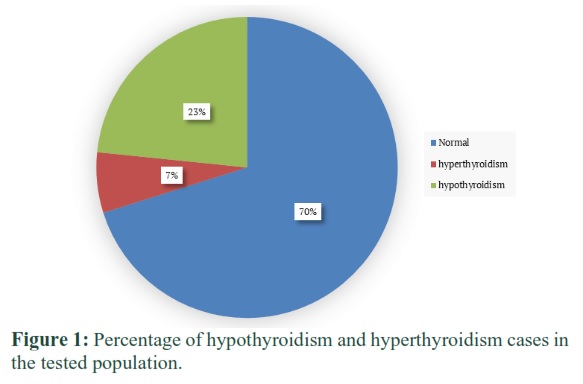
The serum TSH level >5.5mIU, T3 level <2.4pg/ml and T4 level <0.61ng/dl was considered to be hypothyroid and patients with serum TSH level less than 0.4mIU, T3 level>3.8pg/ml and T4 level >1.1ng/dl was considered to be hyperthyroid. When the results were evaluated, it was observed that out of 79 females who had gone through thyroid profile testing, 70% females had normal thyroid profile. However, hypothyroidism was found in 23% females and 7% females had the condition of hyperthyroidism (Figure 5.1). Out of 18 (23%) reported cases of hypothyroidism, 8 cases were of mild (subclinical) hypothyroidism, 3 cases indicated non-thyroidal illness; rare pituitary hypothyroidism.
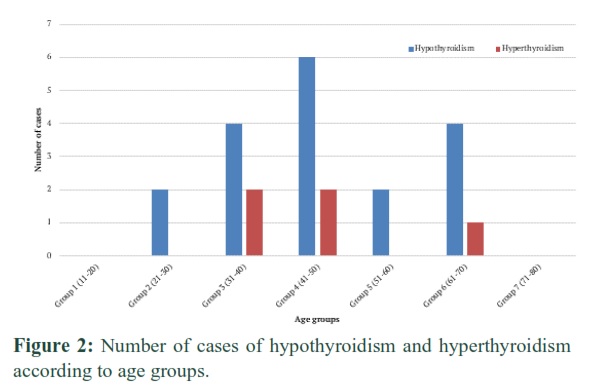
When the results were analyzed based on number of thyroid abnormalities and age groups, it was observed that no cases were found in the age group (11-20 years) and age group (71-80 years). However, maximum cases were observed in group (41-50 years) followed by group (31-40 years) and group (61-70 years) as shown in figure 5.2. When the results were analyzed based on number of thyroid abnormalities and age groups, it was observed that no cases were found in the age group (11-20 years) and age group (71-80 years).
However, maximum cases were observed in group (41-50 years) followed by group (31-40 years) and group (61-70 years) as shown in figure 5.2. The vitamin D levels of studied population was also determined. The level of vitamin D from 20 to 29 ng/mL was considered to be deficient and the vitamin D level was less than 12 ng/ml, it was considered to be an indication of severe vitamin D deficiency. Out of 79 female participants, only 20 (25.31 %) females had normal serum vitamin D levels. Overall, 59 (74.68%) females had vitamin D deficiency as indicated in figure 5.3. When the vitamin D deficiency was correlated with thyroid dysfunction, it was observed that vitamin D levels were non-significantly (p = 0.35) associated with hypothyroidism.
The vitamin D levels of studied population was also determined. The level of vitamin D from 20 to 29 ng/mL was considered to be deficient and the vitamin D level was less than 12 ng/ml, it was considered to be an indication of severe vitamin D deficiency. Out of 79 female participants, only 20 (25.31 %) females had normal serum vitamin D levels. Overall, 59 (74.68%) females had vitamin D deficiency as indicated in figure 5.3. When the vitamin D deficiency was correlated with thyroid dysfunction, it was observed that vitamin D levels were non-significantly (p = 0.35) associated with hypothyroidism.
Figures & Tables
Discussion![]()
In the present study, it was observed that majority cases were of hypothyroidism and the age group that is most affected was of females of 41 to 50 years of age. Similarly, Mammen et al, has also suggested that in older populations TSH level was high. It was suggested that changing in thyroid tests occur due to many reasons e.g: aging or changing in thyroid and pitutary functions [11].
On the other hand, in china a study was conducted, it revealed that TSH level or serum thyrotropin level were increased with the increase of age independent of thyroid disorders. Females and older adults have low T3 and T3/T4 ratio in relation to increased TSH level, while FT4 values remain normal. Both the females and males showed progressive changes in TSH levels with age [12].
A couple of mechanisms describe the decreased vitamin D level in hypothyroid condition. One of these mechanisms is the malabsorption of vitamin D in the intestine and other one is that, the incomplete activation of vitamin D. Low vitamin D levels was observed in patients suffered with Grave’s disease. Vitamin D status and malabsorption of vitamin D in the intestine can affect the onset or development of many autoimmune diseases. Furthermore, vitamin D supplementation play a vital role in the prevention of several autoimmune diseases in individuals.(6) Latest researches have describe the influence of vitamin D on Grave’s Disease (GD) and the role of vitamin D binding protein gene in GD. The inflammatory responses were inhibited by vitamin D in human thyroid cells and T cells [13].
It proposed that serum calcium level and vitamin D deficiency has positive correlation with degree and severity of the hypothyroidism [14]. Vitamin D insufficiency was associated with AITD and HT, especially overt hypothyroidism. Low serum vitamin D levels were independently associated with high serum TSH levels [15]. Hashimoto Thyroiditis patient were presented with decreased activated vitamin D level, independently fluctuated TSH level can cause HT. vitamin D level had negative correlation with TSH level. FT4 and FT3 level had positive correlation with vitamin D level [16]. Mackawy et al, studied that low vitamin D level was seen in hypothyroid patient. Study showed positive correlation with vitamin D and negative correlation with TSH level. It was observed vitamin D deficiency depend on the severity of hypothyroid [17].
Hypothyroidism was found prevalent in the tested female population as 23% of the tested population had hypothyroidism while 9% of them has hyperthyroidism. Moreover, majority of the population had vitamin D deficiency.
Authors' Contribution
All the authors have contributed dedicatedly in terms of giving their technical expertise to give a tenable shape to this manuscript.
The Authors have declared that they have no conflict of interest.
References
- Benvenga S, Tuccari G, Ieni A, Vita R. Thyroid Gland: Anatomy and Physiology: Encyclopedia of Endocrine Diseases, (2018); 2 (4): 382-390.
- Burtis CA, Bruns DE. Thyroid Disorders: Tietz fundamentals of clinical chemistry and molecular diagnostics. 2014; 7: 806-826. Elsevier Health Sciences.
- Aparna P, Muthathal S, Nongkynrih B, Gupta SK. Vitamin D deficiency in India. Journal of family medicine and primary care, (2018); 7(2): 324-330.
- Niafar M, Pourafkari L, Aminmozaffari S, Nader ND. Association of vitamin D deficiency and thyroid function in postmenopausal women. Advanced pharmaceutical bulletin, (2016); 6(4): 639-644.
- Talaei A, Ghorbani F, Asemi Z. The effects of Vitamin D supplementation on thyroid function in hypothyroid patients: A randomized, double-blind, placebo-controlled trial. Indian journal of endocrinology and metabolism, (2018); 22(5): 584-588.
- Kim D. The role of vitamin D in thyroid diseases. International journal of molecular sciences, (2017); 18(9): 1949-1967.
- Nilsson M, Fagman H. Development of the thyroid gland. Development, (2017); 144(12): 2123-40.
- Wang J, Lv S, Chen G, Gao C, He J, Zhong H, et al. Meta-analysis of the association between vitamin D and autoimmune thyroid disease. Nutrients, (2015); 7(4): 2485-98.
- Pearce SH, Dayan C, Wraith DC, Barrell K, Olive N, Jansson L, et al. Antigen-specific immunotherapy with thyrotropin receptor peptides in Graves' hyperthyroidism: a phase I study. Thyroid, (2019); 29(7): 1003-11.
- Amer AH, Chaudhari K, Trivedi R, Patel R. STUDY OF THE SERUM LEVELS OF VITAMIN D AND CALCIUM IONIZED IN THYROID DISORDERS. International Journal of Medical and Biomedical Studies, (2019); 3(7): 93-99.
- Mammen JS, McGready J, Ladenson PW, Simonsick EM. Unstable thyroid function in older adults is caused by alterations in both thyroid and pituitary physiology and is associated with increased mortality. Thyroid, (2017); 27(11): 1370-7.
- Chen X, Zheng X, Ding Z, Su Y, Wang S, Cui B, et al. Relationship of gender and age on thyroid hormone parameters in a large Chinese population. Archives of Endocrinology and Metabolism, (2020); 64(1): 52-8.
- Simsek Y, Cakır I, Yetmis M, Dizdar OS, Baspinar O, Gokay F. Effects of Vitamin D treatment on thyroid autoimmunity. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences, (2016); (21): 85-91.
- Sonawane S, Bora B, Shrikhande D, Bansal S, Kumar P. Vitamin D deficiency and its association with thyroid diseases. International Journal of Contemporary Medical Research, (2017); 4(8): 1765-7.
- Kim D. Low vitamin D status is associated with hypothyroid Hashimoto’s thyroiditis. Hormones, (2016); 15(3): 385-93.
- Chao G, Zhu Y, Fang L. Correlation Between Hashimoto's Thyroiditis–Related Thyroid Hormone Levels and 25-Hydroxyvitamin D. Frontiers in Endocrinology, (2020); 11: 4.
- Mackawy AMH, Al-Ayed BM, Al-Rashidi BM. Vitamin D deficiency and its association with thyroid disease. International journal of health sciences, (2013); 7(3): 267-275.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


