

Short Communication:
Association patterns of volatile metabolites in urinary excretions among Type-2 Non-Insulin dependent diabetes patients
Muhammad Saqib Shahzad1*, Javed Iqbal Bajwa2, Javed Iqbal Wattoo1, Mushtaq A Saleem1
Adv. life sci., vol. 3, no. 3, pp. 71-74, May 2016
*- Corresponding Author: Muhammad Saqib Shahzad, (Email: dr.saqib@ucp.edu.pk)
Authors' Affiliation
2- Faculty of Dentistry, Punjab Medical College, Faisalabad – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Patterns of volatile metabolites in urine are important to detect abnormalities associated with diabetes. Present study was conducted to find out the excretion patterns of endogenously produced alcohols in urine for type 2 (Non-Insulin Dependent) diabetes mellitus. A cross sectional analytical study was conducted with duration extended from Jan to Mar 2015.
Methods: The current study included 40 patients with chronic type 2 diabetes mellitus. In total, 10 sex and age matched subjects with no history of any disease were considered as controls. Blood sugar was estimated by autoanalyzer using standard kit of Merck following manufacturer`s instructions. Urine sugar was quantitatively detected by biuret reagent using titration technique. Urinary alcohol was identified and estimated by gas chromatography. Urinary ketone bodies were estimated by urinary strip.
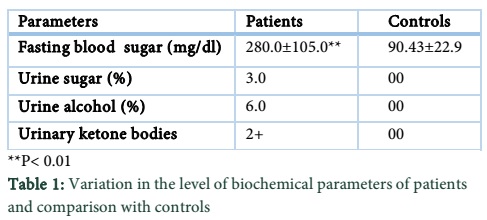
Results: It was observed that level of fasting blood sugar was significantly increased (P<0.001) in patients as compared to their controls. The blood sugar and urinary alcohol in patients were 3.0% and 6.0% respectively. Urinary ketone bodies were found to be 2+. On the other hand urine sugar, alcohol and ketone bodies were not detected in the negative control subjects.
Conclusions: It is concluded that urinary alcohol is endogenously produced in patients with type 2 diabetes due to uncontrolled hyperglycemia. However further work is needed to find out the ratio of urinary and blood alcohol which may confirm the present findings.
Keywords: Urinary alcohol, Urinary sugar, diabetes mellitus, Non-insulin dependent patient, Type 2 diabetes
Introduction
The organic volatile constituents of biological fluids contain clinically useful diagnostic information for the recognition of metabolic disorders in chronic diabetics [1]. Abnormalities in the urinary components in chronic cases of diabetes mellitus are already reported. Patterns of volatile metabolites in urine, are important to detect abnormalities associated with diabetes [2, 3].
Urine alcohol levels do have some relationship to impairment associated with diabetes. It is eliminated from the body mainly by oxidative metabolism in the liver by Class-I isoenzymes of alcohol dehydrogenase [4]. Low molecular weight aliphatic alcohols in urine of patients with diabetes mellitus have been earlier detected [5, 6]. Increased concentrations of ethanol, n-propanol, isobutanol, n-butanol and isopentanol were also detected in urine of patients [7]. Insulin deficiency results hyperglycemia and increased levels of certain hormones that act against insulin (counter regulatory). It also lead to the breakdown of triglycerides. The excess of free fatty acids from the triglycerides are converted to ketones while the glycerol is converted to more glucose [8]. Glucose, fructose and sucrose are converted into cellular energy. These forms of sugar thereby produce ethanol and carbon dioxide as metabolic waste products in the presence of yeasts in diabetic patients [9, 10].
Increased levels of ethanol in urine samples of diabetic patients, aged 50–69 years with glycosuria suggesting genito-urinary candidiasis [11]. Application of flocculating yeast in ethanol production in diabetic patients garnered attention. Increased ethanol tolerance of cells grown was due to the incorporation of the amino acids into the plasma membranes. Thus, resulting in enhanced ability of the plasma membranes to efficiently counteract the fluidizing effect of ethanol when subjected to ethanol stress [11] Alcohol that has been removed from the blood to the urine may pool in the urinary bladder for hours after its metabolism has been completed. Ethanol was either added to the samples or generated by inoculation with the fermenting yeast species Candida albicans and glucose as substrate. These findings are useful for the evaluation of postmortem ethanol production in subjects whose blood has been diluted by infusions with glucose [12, 13].
Alcohol is considered as one of many risk factors for developing nerve damage or neuropathy, which is one of the complications of diabetes [14]. Alcohol can interfere with the process of gluconeogenesis. This occurs during the metabolism of alcohol, in which there is depletion of the supply of pyruvate needed for gluconeogenesis [15]. As a result, alcohol by itself may lead to hypoglycemia or delay recovery from hypoglycemia. It is important to realize that the behavior-altering effects of alcohol can also complicate hypoglycemia. This may result a delayed recognition of hypoglycemia in the patient which ultimately delaying the treatment of hypoglycemia with prompt oral glucose [16]. The experiment concerns the use of urine as a biological specimen for determination of alcohol in clinical and forensic toxicology and discusses factors that might cause the presence of urinary alcohol in non-alcoholic diabetics.
The study was designed to find out the percentages of volatile metabolites (especially alcohol) associated with diabetes in urine of non-alcoholic patients.
Methods
A cross sectional analytical study was conducted in collaboration with Pakistan Council of Scientific and Industrial Research (PCSIR) laboratories with a duration extended from Jan to Mar 2015. Urinary excretion pattern of endogenously produced alcohol, such as ethanol, was evaluated in 40, type 2 diabetic patients. About 10 subjects with different sex and age portfolio without prevalence of any disease were considered as controls. Both male and female patients with age range 45-60 years were included in the study. Their blood sugar was >250 mg/dl and duration of diabetes was > 05 years. Patients with history of any disease and alcoholic patients were excluded from the study. The volunteers were fully informed of the aim and purpose of the study, and signed an informed consent.
Blood sugar was estimated by autoanalyzer using Merck kit method (Merck cat. # 14891) following the manufacturer`s instructions. Urine sugar was quantitatively detected by biuret reagent using titration technique. The biuret reagent was prepared using potassium iodide (30 mmol/L), potassium sodium tartrate (100 mmol/L), CuSo4 (30 mmol/L) and NaoH (3.8 mmol/L). Urinary alcohol was identified and estimated by gas chromatography. Before detection of urine alcohol, urine samples were diluted with aqueous propanol (25 mg/100 mL). Separate peaks were observed against ethanol and propanol. The urine alcohol ratio was finally recorded with integrator. Urinary ketone bodies were estimated by urinary strip.
Data Analysis
The data was analyzed by using SPSS-18.0. Mean and SD of blood sugar was calculated by using student ‘T’ test. P values (< 0.05) were taken statistically significant.
Results
The results clearly revealed that level of fasting blood sugar was significantly increased (P<0.01) of patients as compared to their controls. The blood sugar and urinary alcohol in patients were 3.0 and 6.0%, respectively. Urinary ketone bodies in patients were found to be 2+. On the other hand urine sugar, alcohol and ketone bodies were not detected in the controls subjects. All variables were reported by percentages. Variables were presented as tabulated form.
Data and Tables
Discussion
Distribution, metabolism and elimination of alcohol may be grouped together and called the post absorption stage which leads to empty GI track. The breakdown of body reserves yields energy. The post-absorption stage has a key role to maintain blood glucose levels. Absorption may take as long as 60 minutes depending on many factors, but the post absorption stage may be much longer since alcohol is removed from the body at a rate that is constant over time but which may vary from 0.003-0.030 mL/hour [17]. Volatile organic compounds including ethanol, isopropanol and acetone from endogenous and exogenous sources were observed in total nine samples from diabetic patients [18].
Present study observed that the level of blood and urine sugar was significantly increased in patients with diabetes as compared to their controls. Our study is in accordance with already conducted studies in this respect. Several studies have shown that ethanol can be produced in urine infected with yeast or bacteria in vitro. A study proposed that sugar present in the urine of diabetics is fermented by the yeast Candida albican also present in diabetics urine. This produce the alcohol via its enzyme alcohol oxidase [19,20]. A group of workers also confirmed the presence of alcohol in non-alcoholic diabetic and suggest that this may be the indicative of fermentation process [9,10]. However, it is known that all tissues, except urinary tract, showed that it is under normal conditions [21]. It is reported that alcohol is eliminated from the body mainly by oxidative metabolism in the liver by Class-I isoenzymes of alcohol dehydrogenase [18]. Another study reported that unusually in urine of some diabetics, ethanol was produced with blood sugar > 400 mg/dL. Their ketone bodies are present with large budding yeast strains. Toxicology analysis revealed a urine ethanol level 0.32 mL/dL, although no ethanol was detected in blood [22]. It is confirmed by a group of workers that in the type 2 diabetic patients, urinary excretion of (alcohol) propanol was significantly elevated compared with the control subjects [7]. Some studies also reported the effect of poorly controlled hyperglycemia to multiple primarily vascular complications [21]. The mechanisms by which vascular disease develops include glycosylation of proteins, superoxide production, activation of protein kinase C, that increases vascular permeability and causes endothelial dysfunction; accelerated polyol pathways leading to sorbitol accumulation within tissues [21].
It is therefore, concluded that urinary alcohol is endogenously produced in patients with type-2 diabetes due to uncontrolled hyperglycemia. However, further research is needed to find out the ratio of urinary alcohol/blood alcohol which may confirm the present study that urinary alcohol is not due to the fermentation of sugar by candida but it may be due to the uncontrolled long term hyperglycemia.
References
- Zlatkis A, Brazell RS, Poole CF. The role of organic volatile profiles in clinical diagnosis. Clinical Chemistry, (1981); 27(6): 789-97.
- Rhodes G, Miller M, McConnell ML, Novotny M. Metabolic abnormalities associated with diabetes mellitus, as investigated by gas chromatography and pattern-recognition analysis of profiles of volatile metabolites. Clinical Chemistry, (1981); 27 (4): 580-5.
- Patel HP. The Abnormal Urinalysis. Pediatric Clinics of North America, (2006); 53(3): 325-337.
- Jones AW, Kugelberg FC. Relationship between blood and urine alcohol concentrations in apprehended drivers who claimed consumption of alcohol after driving with and without supporting evidence. Forensic Science International, (2010); (1-3): 97-102.
- Liebich HM, Al-Babbili O, Zlatkis A, Kim K. Gas-chromatographic and mass-spectrometric detection of low-molecular-weight aliphatic alcohols in urine of normal individuals and patients with diabetes mellitus. Clinical Chemistry, (1975); 21(9): 1294-6.
- Lewis GD, Laufman AK, McAnalley BH, Garriott JC. Metabolism of Acetone to Isopropyl Alcohol in Rats and Humans. Journal of Forensic Sciences, (1984); 29(2): 541-549.
- Krönert K, Künzel M, Reutter B, Zimmermann C, Liebich HM, et al. Urinary excretion patterns of endogenously produced alcohols in type 1 (IDDM) and type 2 (NIDDM) diabetes mellitus compared with healthy control subjects. Diabetes Research and Clinical Practice, (1990); 10(2): 161-5.
- Muoio DM, Newgard CB. Fatty Acid Oxidation and Insulin Action When Less Is More. Diabetes, (2008); 57(6): 1455-1456.
- Høiseth G, Kristoffersen L, Larssen B, Arnestad M, Hermansen NO, et al. In vitro formation of ethanol in autopsy samples containing fluoride ions. International Journal of Legal Medicine, (2008); 122(1): 63-6.
- Yajima D, Motani H, Kamei K, Sato Y, Hayakawa M, et al. Ethanol production by Candida albicans in postmortem human blood samples: effects of blood glucose level and dilution. Forensic Science International, (2006); 164(2-3): 116-21.
- Alexander WD, Wills PD, Eldred N. Urinary Ethanol and Diabetes Mellitus. Diabetic Medicine, (1988); 5(5): 463-64.
- Petrovska B, Winkelhausen E, Kuzmanova S. Ethanol and Polyol production from glucose by Candida boidinii NRRL Y-17213. Bulletin of the Chemists and Technologists of Macedonia, (2000); 19(1): 57-63.
- Helander A, Olsson I, Dahl H. Post collection synthesis of ethyl glucuronide by bacteria in urine may cause false identification of alcohol consumption. Clinical Chemistry, (2007); 53(10): 1855-7.
- Winek CL, Esposito FM. Blood alcohol concentrations: factors affecting predictions. Legal Medicine, (1985): 34-61.
- Dentin R, Liu Y, Koo S, Hedrick S. Insulin modulates gluconeogenesis by inhibition of the coactivator TORC2. Nature, (2007); 449(7160): 366-369.
- Plougmann S, Hejlesen O, Turner B, Kerr D, Cavan D. The effect of alcohol on blood glucose in type 1 diabetes—metabolic modelling and integration in a decision support system. International Journal of Medical Information, (2003); 70(2-3): 337-344.
- Edenberg HJ. The genetic of alcohol metabolism. Role of alcohol dehydrogenase and aldehyde dehydrogenase variants. Alcohol Research and Health, (2007); 30(1): 5-13.
- Honey D, Caylor C, Luthi R, Kerrigan S. Comparative alcohol concentrations in blood and vitreous fluid with illustrative case studies. Journal of Analytical Toxicology, (2005); 29(5): 365-9.
- Lidén H, Vijayakumar AR, Gorton L, Marko-Varga G. Rapid alcohol determination in plasma and urine by column liquid chromatography with biosensor detection. Journal of Pharmacy and Biomedical Analysis, (1998); 17(6-7): 1111-28.
- Sulkowski HA, Wu AH, McCarter YS. In-vitro production of ethanol in urine by fermentation. Journal of Forensic Science, (1995); 40(6): 990-3.
- Passariello N, Sepe J, Marrazzo G, De Cicco A, Peluso A, et al. Effect of Aldose Reductase Inhibitor (Tolrestat) on Urinary Albumin Excretion Rate and Glomerular Filtration Rate in IDDM Subjects With Nephropathy. Diabetes Care, (1993); 16(5): 789-95.
- Gruszecki AC, Robinson CA, Kloda S, Brissie RM. High urine ethanol and negative blood and vitreous ethanol in a diabetic woman: a case report, retrospective case survey, and review of the literature. American Journal of Forensic Medicine and Pathology, (2005); 26(1): 96-8.


