

Review Article
Understanding the Role of Genetics in Tumour and Cancer Biology
Abdulaziz Asiri*, Amer Al Ali, Mohammed H. Abu-Alghayth
Adv. life sci., vol. 12, no. 1, pp. 35-48, February 2025
*- Corresponding Author: Abdulaziz Asiri (Email: amfasiri@ub.edu.sa)
Authors' Affiliations
[Date Received: 12/05/2024; Date Revised: 24/11/2024; Date Available Online: 31/12/2024]
Editorial Note: This manuscript has post-publication change in the acknowledgement section.
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
The interplay between genetics and cancer has been a focal point of research for decades, leading to profound understandings into the molecular mechanisms driving tumorigenesis. In this comprehensive review article, we explore the genetic basis of cancer, encompassing the diverse array of alterations that underline oncogenic transformation. From oncogenes to tumor suppressor genes, and from point mutations to chromosomal rearrangements, we delve into the molecular hallmarks of cancer and their implications for diagnosis, treatment, and prevention. Drawing on recent advancements in genomic technologies, we discuss the role of next-generation sequencing, single-cell sequencing, and computational modeling in unraveling the complexity of cancer genetics. Furthermore, we examine the clinical implications of genetic predisposition to cancer, highlighting the importance of genetic testing and counselling in cancer risk assessment and management. Through an exploration of tumor heterogeneity, clonal evolution, and therapeutic resistance, we underscore the challenges and opportunities in precision oncology. Finally, we discuss future directions in cancer genetics research, including precision prevention strategies and ethical considerations.
Keywords: Cancer Genetics; Oncogenes; Tumor Suppressor Genes; Genetic Alterations; Precision Oncology; Clonal Evolution
Introduction![]()
Cancer, considered by way of the uncontrolled growth & feast of abnormal cells, represents one of the most significant health challenges globally. It encompasses a diverse group of diseases that can affect virtually some part of the body, prominent to a range of symptoms & complications. Cancer arises from genetic mutations or alterations that disrupt the normal regulatory mechanisms governing cell growth, division, and death [1]. These aberrations enable cancer cells to proliferate uncontrollably, invade surrounding tissues, and metastasize to distant sites in the body. As a result, cancer can cause significant morbidity and mortality, impacting not only individuals but also families, communities, and entire healthcare systems.
The burden of cancer is substantial and continues to escalate worldwide, with increasing incidence rates observed across various populations and geographical regions [2]. Factors contributing to this rise include population aging, lifestyle changes, environmental exposures, and disparities in access to healthcare. Moreover, the socioeconomic impact of cancer is profound, encompassing direct medical costs, productivity losses, and psychological distress for patients and their caregivers [3]. Addressing the global burden of cancer requires a multifaceted approach that encompasses prevention, early detection, diagnosis, treatment, and palliative care, underscoring the urgent need for coordinated efforts at the national & international levels. At the core of cancer development lies an intricate interplay of genetic alterations that disrupt normal cellular functions and drive oncogenesis. Oncogenes, which encode proteins involved in promoting cell proliferation and survival, can become activated through various mechanisms such as point mutations, gene amplifications, or chromosomal rearrangements [4]. In contrast, tumor suppressor genes doing as carers of the genome, regulating cell cycle progression, DNA repair, & apoptosis. Inactivation or loss of tumor suppressor function, often resulting from genetic mutations or deletions, can unleash unchecked cell growth and contribute to tumorigenesis [5].
Furthermore, genomic instability, characterized by an increased propensity for genetic mutations or chromosomal aberrations, is a hallmark of cancer cells [6]. This instability can arise from defects in DNA repair pathways, exposure to genotoxic agents, or dysregulation of mitotic processes. Collectively, these genetic changes confer choosy growth leads to cancer cells, enabling them to evade normal regulatory mechanisms and proliferate uncontrollably. Understanding the genetic basis of cancer is crucial for elucidating the molecular mechanisms driving oncogenesis & informing the development of targeted therapies, diagnostic biomarkers, and preventive interventions tailored to individual patients.
Advances in cancer genetics have revolutionized our approach to cancer diagnosis, treatment, and prevention, offering unprecedented opportunities for personalized medicine. Genetic markers and molecular profiling techniques play a crucial role in stratifying patients based on their risk of developing cancer, guiding early detection efforts, and informing screening recommendations [7]. Moreover, genomic analyses can help identify hereditary cancer syndromes and high-risk individuals who may benefit from targeted surveillance or preventive interventions such as prophylactic surgeries or chemoprevention strategies. In the realm of cancer treatment, an in-depth understanding of cancer genetics is crucial for identifying actionable genetic alterations that can be targeted with precision therapies. Targeted therapies, with small molecule inhibitors, monoclonal antibodies, & immunotherapies, are designed to selectively target cancer-specific molecular vulnerabilities while minimizing systemic toxicity [8].
Additionally, molecular profiling can aid in predicting treatment responses, monitoring disease progression, and identifying mechanisms of therapeutic resistance, thereby facilitating more effective and personalized treatment strategies [9]. Furthermore, the insights gained from cancer genetics research hold immense promise for precision prevention strategies aimed at reducing the incidence and burden of cancer [10]. By identifying individuals at elevated risk based on their genetic predisposition, lifestyle factors, and environmental exposures, we can implement targeted interventions to mitigate risk factors, promote healthy behaviours, and facilitate early detection through screening and surveillance programs. Ultimately, integrating cancer genetics into clinical practice enables a proactive and personalized approach to cancer care, with the potential to improve patient outcomes, reduce healthcare costs, and alleviate the global burden of cancer.
One of the earliest milestones occurred in the 1970s with the discovery of the first oncogene, the RAS (Rat sarcoma) gene, in retroviruses causing sarcomas in rodents [11]. This discovery laid the foundation for elucidating the role of oncogenes in promoting uncontrolled cell growth and tumorigenesis. In the 1980s, the identification of tumor suppressor genes emerged as a pivotal milestone in cancer genetics research. The seminal discovery of the RB1 gene, implicated in retinoblastoma, provided compelling evidence for the existence of genes that function as brakes on cell proliferation [12]. Subsequent studies run to the empathy of other tumor suppressor genes, with TP53, (tumour protein 53) PTEN (Phosphatase and TENsin homolog), & APC (Adenomatous polyposis coli), which play critical roles in keeping genomic constancy & averting the development of cancer. The development of DNA sequencing technologies facilitated the cloning and characterization of cancer-associated genes, paving the way for the identification of mutations underlying familial cancer syndromes and sporadic tumors [13]. Furthermore, the mapping of the human genome in the early 2000s provided a comprehensive catalog of genetic variants associated with cancer susceptibility, laying the groundwork for genome-wide association studies (GWAS) to detect common genetic risk factors for cancer. In modern years, advances in high-throughput sequencing technologies have revolutionized cancer genetics research, enabling the comprehensive characterization of the cancer genome across diverse tumor types. Large-scale cancer genomics initiatives, such as The Cancer Genome Atlas (TCGA) & the International Cancer Genome Consortium (ICGC), have created vast quantities of genomic data, facilitating the discovery of novel cancer driver genes, mutational signatures, and therapeutic targets [14].
These efforts have transformed our appreciative of the molecular heterogeneity of cancer & provided valuable visions into the evolutionary dynamics of tumor progression and metastasis. Several key discoveries and advancements have contributed to our current thoughtful of the genetic basis of cancer and its clinical implications. One of the landmark discoveries was the identification of the BRCA1 & BRCA2 genes, which are allied with hereditary breast & ovarian cancer syndromes [15]. The identification of these genes not only provided critical insights into the genetic predisposition to cancer but also covered the way for the growth of genetic testing and risk-reduction strategies for individuals with familial cancer risk. Another key advancement was the elucidation of the PI3K/AKT/mTOR signalling pathway, which plays a vital role in regulating cell growth, survival, & metabolism [16]. Dysregulation of this pathway has been implicated in a wide range of cancers, principal to the expansion of targeted therapies such as mTOR inhibitors for the treatment of certain cancer types. The advent of next-generation sequencing (NGS) technologies has transformed cancer genomics study via enabling complete profiling of tumor genomes at unprecedented resolution [17]. NGS-based methods, including whole-genome sequencing, whole-exome sequencing, and targeted panel sequencing, have facilitated the identification of recurrent somatic mutations, copy number changes, & structural variants across diverse cancer types. These genomic insights have not only advanced our understanding of cancer biology but also concreted the way for the progress of precision oncology tactics, wherein treatment decisions are showed through the molecular profile of the tumor. Moreover, the emergence of immunotherapy as a paradigm-shifting approach to cancer treatment represents a major milestone in cancer research. Immune checkpoint inhibitors, such as PD-1 & PD-L1 inhibitors, have revealed extraordinary efficacy in a subset of cancer patients, leading to durable responses and long-term survival benefits [18]. The identification of predictive biomarkers, such as tumor mutational burden & microsatellite instability, has facilitated patient selection for immunotherapy and improved clinical outcomes [19]. Overall, these key discoveries and advancements have revolutionized our appreciative of cancer genetics & paved the way for precision medicine approaches that hold the promise of more effective and personalized cancer treatment strategies.
Methods
![]()
Literature search strategy and selection criteria
A methodical strategy is required while performing a literature review or choosing pertinent studies to ensure that the literature gathered is of the highest caliber and closely related to the research issue. This review paper gathered information from Scopus, Web of Science, PsycINFOGoogle Scholar, Pubmed, SciFinder, and Google Web. The necessary data was retrieved using various keywords from published research and review articles. The published works consulted for this evaluation were selected latest references up to 2024.
Discussion![]()
Genetic Basis of Cancer
Oncogenes, tumor suppressor genes, & DNA repair genes represent three key classes of genes that play critical roles in maintaining the balance between cell proliferation & cell death, and their dysregulation is central to the development of cancer. Oncogenes are genes that, when mutated or activated, promote cell growth & proliferation. These genes typically encode proteins involved in signalling pathways that regulate cell cycle progression, apoptosis, and differentiation. Oncogenes can become activated through various mechanisms, such as point mutations, gene amplifications, or chromosomal translocations. Examples of well-known oncogenes include RAS, MYC, and ERBB2, which are frequently implicated in a wide range of cancers [20, 21]. In contrast, tumor suppressor genes act as carers of the genome, inhibiting cell proliferation & preventing the development of cancer. Loss-of-function mutations or deletions in tumor suppressor genes can disrupt their normal regulatory functions, leading to uncontrolled cell growth and tumorigenesis. Tumor suppressor genes encode proteins that govern critical cellular processes, including DNA repair, cell cycle checkpoint control, & apoptosis. Examples of tumor suppressor genes include TP53, RB1, and PTEN, mutations in which are commonly associated with various cancer types [22]. DNA repair genes play a crucial role in maintaining genomic integrity by detecting and repairing DNA damage caused by endogenous & exogenous insults, such as reactive oxygen species, ultraviolet radiation, & chemical carcinogens [23]. Mutations in DNA repair genes can impair the cell’s ability to repair damaged DNA, leading to the accumulation of mutations and genomic instability, which are hallmarks of cancer. Defects in DNA repair pathways can predispose individuals to hereditary cancer syndromes, such as hereditary breast & ovarian cancer syndrome (caused by mutations in BRCA1 & BRCA2) and Lynch syndrome (caused by mutations in DNA mismatch repair genes). Cancer begins, progresses, & metastasizes mostly due to mutations in oncogenes, tumor suppressor genes, & DNA repair genes [24]. Oncogenic mutations confer selective growth advantages to cancer cells by activating signalling pathways that promote cell proliferation, survival, and angiogenesis. These mutations can arise done various mechanisms, with point mutations, gene amplifications, or chromosomal rearrangements, follow-on in the constitutive stimulation of oncogenic pathways. For example, activating mutations in the RAS oncogene leads to hyperactivation of downstream signalling cascades, such as the MAPK & PI3K/AKT pathways, driving cell proliferation and tumorigenesis [25]. Conversely, loss-of-function mutations or deletions in tumor suppressor genes remove critical constraints on cell growth and survival, allowing cancer cells to evade apoptotic signals and resist antiproliferative signals [26].
Tumor suppressor gene mutations can impair cell cycle checkpoint control, DNA repair mechanisms, and apoptotic pathways, leading to uncontrolled cell proliferation and genomic instability. For instance, mutations in the TP53 tumor suppressor gene disrupt its capability to induce cell cycle arrest or apoptosis in response to DNA damage, facilitating the survival & proliferation of genetically unstable cells [27]. Additionally, mutations in DNA repair genes cooperation the cell’s capacity to repair DNA damage, leading to the gathering of mutations & genomic changes that drive cancer development [28]. Defects in DNA repair pathways can result in an increased mutation rate and genomic instability, creating a favourable environment for the acquisition of additional oncogenic mutations and the progression of malignant phenotypes [29]. The cumulative effects of mutations in oncogenes, tumor suppressor genes, & DNA repair genes contribute to the multistep process of cancer development, from the initiation of tumorigenesis to the acquisition of metastatic potential.
Mechanisms of gene regulation and dysregulation in cancer
Gene regulation plays a critical part in controlling the expression of genes elaborate in essential cellular processes, including cell growth, differentiation, & survival. Dysregulation of gene expression is a hallmark of cancer and can occur done various mechanisms, with genetic mutations, epigenetic modifications, and alterations in signalling pathways. Aberrant gene expression in cancer cells can promote tumorigenesis by disrupting normal cellular functions and driving uncontrolled cell growth [30]. Genetic mutations can directly affect gene expression via mutable the DNA sequence within regulatory regions, such as promoters, enhancers, or transcription factor binding sites. Point mutations, insertions, or deletions in these regulatory elements can disrupt transcription factor binding or alter the affinity of transcriptional regulators, leading to aberrant gene expression patterns [31]. Additionally, mutations in coding regions of genes can impact mRNA stability, translation efficiency, or protein function, further contributing to dysregulated gene expression in cancer [32]. Histone alterations, DNA methylation, & noncoding RNA-mediated gene regulation are examples of epigenetic modifications; represent another mechanism of gene dysregulation in cancer [33]. Aberrant DNA methylation patterns, characterized by global hypomethylation and localized hypermethylation of CpG islands within gene promoters, can silence tumor suppressor genes or activate oncogenes, driving cancer progression [34]. Histone modifications, such as acetylation, methylation, or phosphorylation, can alter chromatin structure and accessibility, influencing gene expression patterns in cancer cells [35]. Furthermore, dysregulation of noncoding RNAs can interfere with the regulation of posttranscriptional genes and support carcinogenic signalling pathways in cancer. These noncoding RNAs include circular, long, and microRNAs [36]. Furthermore, dysregulated signaling pathways play a central role in driving aberrant gene expression patterns in cancer. Aberrant activation of growth factor signaling pathways, such as the MAPK, PI3K/AKT, & Wnt/β-catenin pathways, can promote cell proliferation, survival, and invasion by altering the expression of downstream target genes intricate in these processes. Additionally, dysregulation of cell cycle control, apoptosis, & DNA damage response pathways can further exacerbate gene expression abnormalities and contribute to cancer progression. Collectively, the dysregulation of gene expression through genetic, epigenetic, and signaling pathway alterations is a hallmark of cancer and underlies its pathogenesis and progression.
Types of Genetic Alterations in Cancer
Point mutations and chromosomal rearrangements are two distinct types of genetic alterations that play significant roles in driving cancer development and progression. Point mutations refer to changes in individual nucleotides within the DNA sequence, where a single nucleotide is substituted, inserted, or deleted. These mutations can occur randomly or as a result of exposure to environmental factors such as ultraviolet chemicals, radiation, or errors during DNA replication [37]. In cancer, point mutations can prime to the activation of oncogenes or the inactivation of tumor suppressor genes, thereby promoting uncontrolled cell growth and tumorigenesis. For example, point mutations in oncogenes such as RAS or BRAF can result in constitutive activation of downstream signaling pathways, leading to aberrant cell proliferation and tumor formation [38]. Similarly, point mutations in tumor suppressor genes such as TP53 or PTEN can disrupt their normal functions, allowing cancer cells to evade growth inhibitory signals and undergo unchecked proliferation [39]. The accumulation of point mutations over time can contribute to the genetic heterogeneity and evolution of tumors, leading to treatment resistance and disease progression. Chromosomal rearrangements, on the other hand, involve large-scale alterations in the structure of chromosomes, where segments of DNA are broken, rearranged, or exchanged between different chromosomes [40]. These rearrangements can result from errors during DNA replication, exposure to DNA-damaging agents, or defects in DNA repair mechanisms. Chromosomal rearrangements can chief to the fusion of genes, creating novel gene fusions or chimeric proteins with oncogenic properties. The BCR-ABL fusion gene, which is linked to chronic myeloid leukemia (CML) and is the product of a translocation between chromosomes 9 and 22, is one well-known example [41]. The BCR-ABL fusion protein has constitutive tyrosine kinase activity, leading to uncontrolled cell proliferation and leukemia development. Additionally, chromosomal rearrangements can lead to gene amplifications, where multiple copies of a gene or chromosomal region are duplicated, resulting in increased gene expression and oncogene activation [42]. Conversely, chromosomal deletions or loss of heterozygosity (LOH) can lead to the loss of tumor suppressor genes or critical regulatory regions, promoting tumorigenesis [43]. The identification of specific chromosomal rearrangements and their associated oncogenic drivers has delivered valued visions into the molecular mechanisms fundamental cancer development and has concreted the way for the development of targeted therapies & accuracy medicine approaches. Copy number variations (CNVs) and epigenetic modifications are two distinct but interconnected mechanisms that contribute to the regulation of gene expression & the development of cancer [44]. Copy number variations refer to changes in the number of copies of a particular DNA segment, ranging from small-scale insertions or deletions to large-scale amplifications or deletions of genomic regions. CNVs can arise through various mechanisms, including errors during DNA replication, unequal crossing over during meiosis, or exposure to genotoxic agents. In cancer, CNVs can have significant implications for gene dosage and expression, leading to alterations in cellular processes such as cell cycle regulation, DNA repair, & apoptosis [45].
Amplifications of oncogenes, resulting in increased gene dosage and overexpression, can promote uncontrolled cell proliferation and tumorigenesis. For example, amplification of the ERBB2 gene, encoding the HER2 receptor tyrosine kinase, is observed in a subset of breast cancers & is associated with aggressive tumor behaviour & poor prognosis [46]. The identification of CNVs through genomic profiling techniques such as array relative genomic hybridization (aCGH) or NGS (next-generation sequencing) has provided valuable insights into the genetic drivers of cancer and has facilitated the development of targeted therapies & precision medicine methodologies aimed at correcting gene dosage imbalances [47]. Epigenetic modifications, on the other hand, involve chemical modifications to DNA or histone proteins that alter the structure and accessibility of chromatin without changing the underlying DNA sequence. These modifications contain DNA methylation, histone acetylation, methylation, phosphorylation, & ubiquitination, among others. Epigenetic modifications play serious parts in regulating gene expression patterns through influencing chromatin structure, DNA accessibility, and the recruitment of transcriptional regulators. Dysregulation of epigenetic mechanisms can principal to aberrant gene expression patterns & contribute to cancer development and progression. In cancer, global hypomethylation of DNA and localized hypermethylation of CpG islands within gene promoters are commonly observed, leading to silencing of tumor suppressor genes or activation of oncogenes. For example, hypermethylation of the promoter region of the MLH1 gene, a DNA mismatch repair gene, is associated with the development of microsatellite instability and hereditary nonpolyposis colorectal cancer [48]. Similarly, alterations in histone modifications, such as loss of histone acetylation or gain of histone methylation, can disrupt chromatin structure and lead to transcriptional dysregulation in cancer cells. The development of epigenetic-targeted therapies, such as DNA methyltransferase inhibitors & histone deacetylase inhibitors, has emerged as an auspicious strategy for reprogramming aberrant epigenetic states and restoring normal gene expression patterns in cancer cells [49]. Overall, the interplay between CNVs and epigenetic modifications contributes to the complex landscape of cancer genetics and provides opportunities for the development of innovative diagnostic & therapeutic methods for cancer management.
Commonly Implicated Genes and Pathways
TP53
TP53, also known as the tumor protein p53, is a critical tumor suppressor gene that shows a central role in safeguarding the genome and preventing the development of cancer [50]. TP53 is a transcription factor found on the short arm of chromosome 17 that regulates the expression of genes involved in cell cycle arrest, DNA repair, apoptosis, and senescence in response to cellular stress signals such as DNA damage, oncogene activation, or hypoxia. The p53 protein works as a “guardian of the genome,” coordinating cellular responses to stress and maintaining genomic stability by encouraging DNA repair or causing apoptosis in irreversibly damaged cells [51]. Dysregulation or loss of TP53 function is one of the most common genetic alterations observed in human cancers, occurring in over half of all malignancies [52]. TP53 mutations can lead to the abrogation of its tumor suppressor functions, allowing cancer cells to evade growth inhibitory signals, resist apoptosis, and acquire genetic instability. Moreover, mutant p53 proteins can acquire oncogenic gain-of-function properties, promoting tumor progression, metastasis, and therapeutic resistance. The significance of TP53 in cancer biology is underscored by its pivotal role in driving tumorigenesis and it’s possible as a therapeutic target for cancer treatment.
BRCA1 & BRCA2
BRCA1 & BRCA2 are tumor suppressor genes that encode proteins involved in maintaining genomic integrity and preventing the development of breast, ovarian, & other cancers [53]. BRCA1 is positioned on chromosome 17, while BRCA2 is situated on chromosome 13. Both genes encode proteins that function in DNA repair pathways, particularly homologous recombination-mediated repair of DNA double-strand breaks. BRCA1 and BRCA2 proteins play critical roles in coordinating the repair of DNA damage, ensuring the fidelity of the genome, and suppressing the accumulation of mutations that can drive tumorigenesis. Mutations in BRCA1 or BRCA2 genes, inherited in an autosomal dominant way, are associated with hereditary breast & ovarian cancer syndrome (HBOC), characterized via an increased risk of developing breast, ovarian, and additional cancers at a young age [54]. BRCA1/2 mutations disrupt normal DNA repair mechanisms, leading to genomic instability and the accumulation of genetic alterations that predispose individuals to cancer progress [55]. Additionally, BRCA1/2 mutations are associated with an increased susceptibility to DNA-damaging agents, such as ionizing radiation or platinum-based chemotherapies, making affected individuals more prone to treatment-related toxicities. Genetic testing for BRCA1/2 mutations plays an essential part in recognising individuals at high risk of HBOC, enabling personalized risk assessment, early detection strategies, and targeted preventive interventions, such as risk-reducing surgeries or chemoprevention.
PTEN
PTEN, or phosphatase & tensin homolog, is a tumor suppressor gene positioned on chromosome 10q23.3 that encodes a lipid phosphatase protein with dual-specificity phosphatase activity. PTEN plays a perilous part in negatively regulating the phosphoinositide 3-kinase (PI3K)/AKT/mTOR signaling pathway, which is intricate in controlling cell proliferation, survival, metabolism, and migration [56]. PTEN functions as a lipid phosphatase, dephosphorylating phosphatidylinositol (3,4,5)-trisphosphate (PIP3) to phosphatidylinositol (4,5)-bisphosphate (PIP2), thereby antagonizing the activation of AKT signaling and suppressing downstream oncogenic pathways. Loss-of-function mutations, deletions, or epigenetic silencing of PTEN are commonly observed in various cancers, including prostate, breast, and endometrial cancers, important to constitutive activation of the PI3K/AKT/mTOR path & promoting tumorigenesis [57]. PTEN alterations are associated with increased cell proliferation, enhanced cell survival, metabolic reprogramming, and resistance to apoptosis, contributing to tumor growth, invasion, and metastasis. Furthermore, PTEN deficiency has implications for cancer therapy, as it confers resistance to targeted therapies and chemotherapy agents that rely on intact PTEN function for their efficacy [58]. The identification of PTEN alterations in cancer patients has implications for prognosis, treatment selection, and the development of targeted therapeutic strategies expected at restoring PTEN task or targeting alternative nodes in the PI3K/AKT/mTOR way.
RAS Pathway
The RAS Lane is a crucial signaling cascade intricate in regulating cell growth, proliferation, & survival. Activation of the RAS pathway occurs in response to extracellular signals such as growth factors, hormones, or cytokines binding to cell surface receptors, leading to the activation of RAS proteins. RAS proteins, including HRAS, KRAS, and NRAS, act as molecular switches that cycle between an inactive GDP-bound state & an active GTP-bound state [59]. Upon activation, GTP-bound RAS proteins stimulate downstream signaling cascades, with the MAPK & PI3K/AKT pathways, through interactions with effector proteins such as RAF kinases. The MAPK pathway, also known as the mitogen-activated protein kinase path, is a highly conserved signaling pathway complicated in transducing extracellular signals into intracellular responses such as cell proliferation, differentiation, & survival. Activation of the MAPK pathway occurs through a series of phosphorylation events involving a cascade of protein kinases, including RAF, MEK, and ERK [60]. Once activated, ERK translocates to the nucleus, where it phosphorylates transcription factors and other nuclear targets, leading to changes in gene expression that promote cell growth and survival. Dysregulation of the RAS-MAPK pathway, often through activating mutations in RAS or upstream receptor tyrosine kinases, is commonly observed in various cancers & pays to tumor initiation, progression, & metastasis [61].
PI3K/AKT/mTOR pathway
The PI3K/AKT/mTOR way is another critical signaling pathway convoluted in regulating cell growth, metabolism, & survival. Activation of the PI3K/AKT/mTOR pathway occurs in response to growth factors, insulin, or other stimuli binding to receptor tyrosine kinases, leading to the activation of PI3K [62]. PI3K phosphorylates phosphatidylinositol lipids, generating PIP3 which assists as a docking site for AKT. Once recruited to the plasma membrane, AKT is activated over phosphorylation via PDK1 (phosphoinositide-dependent kinase 1) & mammalian target of mTORC2 (rapamycin complex 2) Activated AKT phosphorylates various downstream targets complicated in cell survival, protein synthesis, & metabolism, including mTOR complex 1 (mTORC1), which controls protein translation and cell growth. Dysregulation of the PI3K/AKT/mTOR lane is commonly observed in cancer and contributes to oncogenesis and tumor progression [63]. Genetic alterations such as activating mutations in PIK3CA (encoding the catalytic subunit of PI3K), loss-of-function mutations in PTEN (a negative regulator of the pathway), or amplification of AKT or mTOR genes can lead to constitutive activation of the way. Hyperactivation of the PI3K/AKT/mTOR pathway promotes cell proliferation, survival, & resistance to apoptosis, making it an attractive target for cancer therapy. Inhibitors targeting various components of the pathway, such as PI3K inhibitors, AKT inhibitors, & mTOR inhibitors, have shown promise in preclinical & clinical studies for the treatment of a wide range of cancers [64].
Genetic Predisposition to Cancer
Hereditary cancer syndromes include a group of genetic disorders characterized via an improved susceptibility to certain types of cancer. These syndromes are caused via inherited mutations in specific genes that play critical roles in regulating cell growth, DNA repair, & tumor suppression. Examples of well-known hereditary cancer syndromes include hereditary breast & ovarian cancer syndrome (associated with mutations in the BRCA1 & BRCA2 genes), Lynch syndrome (associated with mutations in DNA mismatch repair genes such as MSH6, MLH1, PMS2 & MSH2), and hereditary adenomatous polyposis (associated with mutations in the APC gene) [65]. Inherited mutations in these genes predispose individuals to a significantly higher risk of developing specific cancers associated to the common population. Hereditary cancer syndromes often exhibit an autosomal dominant design of inheritance, meaning that individuals with a single copy of the mutated gene have an increased risk of developing cancer. The importance of family history in cancer risk assessment cannot be overstated, as it serves as a valuable tool for identifying individuals who might be at enlarged risk of hereditary cancer syndromes [66]. Family history information provides insights into the presence of cancer in multiple generations of a family, the types of cancer diagnosed, the age at diagnosis, and the number of affected relatives. A strong family history of certain cancers, particularly those associated with known hereditary cancer syndromes, may warrant further evaluation through genetic testing and counselling. In addition to genetic factors, family history may also provide clues about shared environmental exposures or lifestyle factors that contribute to cancer risk. Genetic testing and counselling play pivotal roles in the identification, management, and prevention of hereditary cancer syndromes [67]. Genetic testing contains analyzing an individual’s DNA to identify mutations in genes associated with hereditary cancer predisposition. This testing can help confirm a clinical diagnosis of a hereditary cancer syndrome, inform personalized cancer screening and prevention strategies, guide treatment decisions, and facilitate cascade testing of at-risk family members. Genetic counseling, provided by trained healthcare professionals such as genetic counsellors or medical geneticists, involves a comprehensive assessment of an individual’s personal & family medical history, education about genetic testing options and implications, interpretation of test results, and discussion of risk management and surveillance recommendations [68]. Genetic counselors play a critical role in empowering individuals to make informed decisions about genetic testing, addressing psychosocial concerns, and providing ongoing support and guidance throughout the testing process. Overall, hereditary cancer syndromes represent an important subset of cancer predisposition disorders with significant implications for cancer risk assessment, early detection, and prevention. By recognizing the importance of family history, facilitating access to genetic testing and counseling services, and implementing personalized risk management strategies, healthcare providers can show a proactive part in reducing the burden of hereditary cancers & educating outcomes for individuals and families affected by these conditions.
Tumor Heterogeneity and Evolution
Intratumoral heterogeneity mentions to the presence of diverse populations of cancer cells inside a single tumor, characterized via distinct genetic, epigenetic, & phenotypic profiles [69]. This heterogeneity arises from genetic mutations, chromosomal rearrangements, epigenetic modifications, and microenvironmental influences that drive clonal diversification and evolution over time. Intratumoral heterogeneity poses momentous challenges in cancer diagnosis, treatment, & prognosis, as altered subclones within a tumor may show varying responses to therapy and contribute to disease progression and metastasis [70]. Understanding intratumoral heterogeneity is critical for guiding treatment decisions and developing personalized therapeutic strategies that target the specific genetic alterations and molecular pathways driving tumor growth and survival. Clonal evolution and tumor progression describe the dynamic process by which cancer cells acquire genetic alterations and evolve over time to become increasingly aggressive and resistant to treatment [71]. Clonal evolution involves the sequential growth of mutations, chromosomal rearrangements, and epigenetic changes within tumor cells, leading to the appearance of genetically distinct subclones with selective growth advantages. This evolutionary process is driven by genomic instability, mutagenic insults, & selective pressures imposed by the tumor microenvironment & therapeutic interventions.
As tumors evolve, clonal subpopulations with genetic alterations conferring resistance to chemotherapy, targeted therapies, or immunotherapy may emerge, leading to treatment failure and disease relapse [72]. Understanding clonal evolution and tumor progression is essential for predicting treatment responses, identifying therapeutic vulnerabilities, and developing strategies to incredulous resistance mechanisms in cancer. The implications of intratumoral heterogeneity & clonal evolution for personalized medicine & treatment resistance are profound. Personalized medicine aims to tailor cancer treatments to the unique genetic & molecular characteristics of individual tumors, with the goal of maximizing therapeutic efficacy while minimizing toxicity [73]. However, intratumoral heterogeneity and clonal evolution present significant challenges to the success of personalized medicine, as treatment responses may vary widely among different clonal subpopulations within a tumor. Moreover, the emergence of treatment-resistant clones can limit the effectiveness of targeted therapies and immunotherapies, necessitating the development of alternative treatment strategies and combination approaches to overcome resistance [74]. Integrating genomic profiling, single-cell sequencing, and spatial transcriptomics technologies into clinical practice can provide insights into intratumoral heterogeneity, clonal evolution, and treatment resistance, enabling more precise and effective therapeutic interventions [75]. By comprehensively characterizing the genetic landscape of tumors and monitoring clonal dynamics over time, oncologists can optimize treatment selection, monitor disease progression, and adapt therapeutic strategies to address the evolving complexity of cancer.
Emerging Technologies and Approaches
Next-generation sequencing (NGS)
Next-generation sequencing represents a revolutionary approach to DNA sequencing that has dramatically transformed our ability to decipher the genetic code with unprecedented speed, accuracy, and cost-effectiveness [76]. Unlike traditional Sanger sequencing methods, which rely on labour-intensive and time-consuming gel electrophoresis techniques, NGS platforms utilize massively parallel sequencing technology to simultaneously sequence millions of DNA fragments in a high-throughput manner [77]. This parallelization enables the rapid generation of vast amounts of sequencing data, facilitating the comprehensive analysis of entire genomes, exomes, transcriptomes, and epigenomes. NGS has revolutionized genomics research and clinical diagnostics by enabling the identification of genetic variants, structural rearrangements, and epigenetic modifications associated with human diseases, with cancer, inherited disorders, & infectious diseases. The scalability, flexibility, and affordability of NGS platforms have democratized access to genomic technologies, making large-scale sequencing projects and personalized medicine initiatives feasible on a global scale. NGS continues to drive innovations in biomedical research, drug discovery, and precision medicine, unlocking new insights into the genetic basis of health & disease. For instance, the utilization of NGS in identifying genomic alterations has significantly transformed the treatment strategies for lung cancer patients, spanning from perioperative care to advanced stages [78]. Simultaneously, recent findings highlight the promising roles of NGS in early screening, detection, and Minimal Residual Disease (MRD) assessment. Another recent study examined the impact of NGS panels on the clinical progress of cancer patients [79]. It found that while NGS testing performed within clinical judgement significantly improves progression-free survival (PFS), it does not significantly influence PFS when based on drug-based criteria or having favourable molecular targets. The outcomes suggest that clinical judgement plays a crucial role in guiding therapy decisions for certain patient populations, such as those with advanced cancers needing multiple genetic markers or those screened for molecular clinical trials. However, NGS testing may not be beneficial for patients with poor performance status, rapidly progressing cancer, short life expectancy, or lack of standard therapeutic options. Nevertheless, obstacles persist, notably the absence of uniform protocols across various platforms and bioinformatics analysis methods, as well as the intricacies involved in interpreting and utilizing the multitude of genomic mutations for treatment decisions. Future endeavours should focus on surmounting these challenges and broadening the scope of NGS applications, including its integration with immunotherapy approaches.
Single-cell sequencing
Single-cell sequencing represents a cutting-edge technology that permits academics to analyze the genetic & molecular profiles of individual cells using unprecedented resolution & sensitivity [80]. Traditional bulk sequencing approaches rely on the averaging of signals from millions of cells, masking the heterogeneity present within complex cellular populations. Single-cell sequencing overcomes this limitation by isolating and sequencing individual cells, enabling the characterization of cell-to-cell variability in gene expression, chromatin accessibility, and epigenetic modifications. This technology has revolutionized our understanding of cellular diversity, development, and disease pathogenesis by revealing rare cell populations, identifying transitional states, and dissecting cellular hierarchies within tissues and tumors. Single-cell sequencing has broad applications across diverse fields, including cancer biology, immunology, neurobiology, and developmental biology. In cancer research, single-cell sequencing has delivered insights into tumor heterogeneity, clonal evolution, & treatment resistance, enabling the identification of rare subpopulations of cells with stem-like properties or metastatic potential [81]. Moreover, single-cell sequencing holds promise for guiding precision medicine approaches by identifying actionable genetic alterations and biomarkers at the single-cell level [82]. Despite technical challenges such as sample preparation, data analysis, and cost, single-cell sequencing continues to advance rapidly, fueled by innovations in microfluidics, droplet-based technologies, and computational biology. As single-cell sequencing technologies become more accessible and scalable, they are poised to revolutionize biomedical research and clinical diagnostics, paving the way for personalized approaches to disease prevention, diagnosis, and therapy [83].
Functional genomics
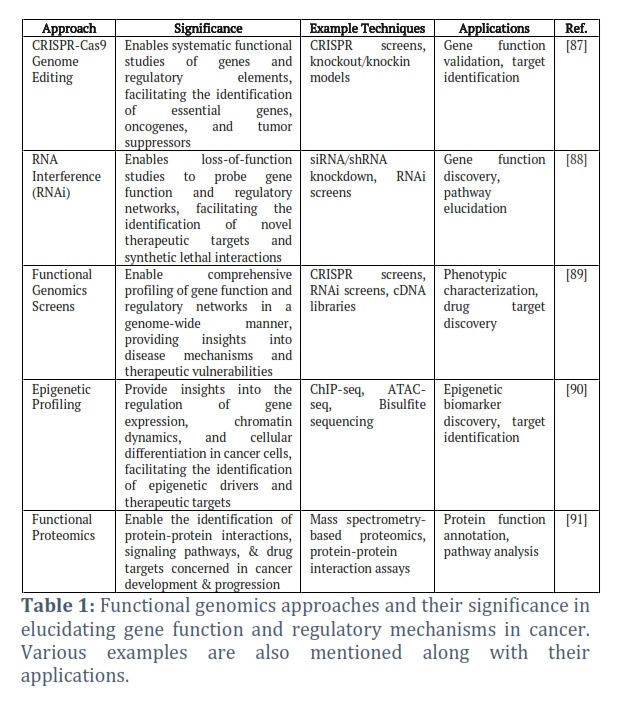
Functional genomics is a multidisciplinary field that aims to elucidate the function and regulation of genes on a genome-wide scale, providing insights into the complex biological processes underlying health and disease [84]. Unlike traditional genomics approaches that focus on cataloging genetic variants or gene expression patterns, functional genomics integrates experimental techniques such as genome editing, RNA interference, and high-throughput screening to systematically interrogate the functions of genes and noncoding elements within the genome (Table 1). By perturbing gene function and observing phenotypic changes at the cellular or organismal level, functional genomics enables the identification of genes involved in specific biological pathways, cellular processes, or disease states. Functional genomics approaches have been instrumental in uncovering novel gene functions, dissecting gene regulatory networks, and elucidating the molecular mechanisms underlying cancer. In cancer research, functional genomics has been used to identify driver genes, tumor suppressors, and oncogenic pathways, facilitating the progress of targeted therapies & accuracy medicine methods [85]. Moreover, functional genomics provides a powerful framework for prioritizing candidate genes and therapeutic targets from large-scale genomic datasets, enabling the translation of genomic discoveries into clinically relevant insights and interventions [86].
Artificial intelligence (AI) in combination with computational modelling
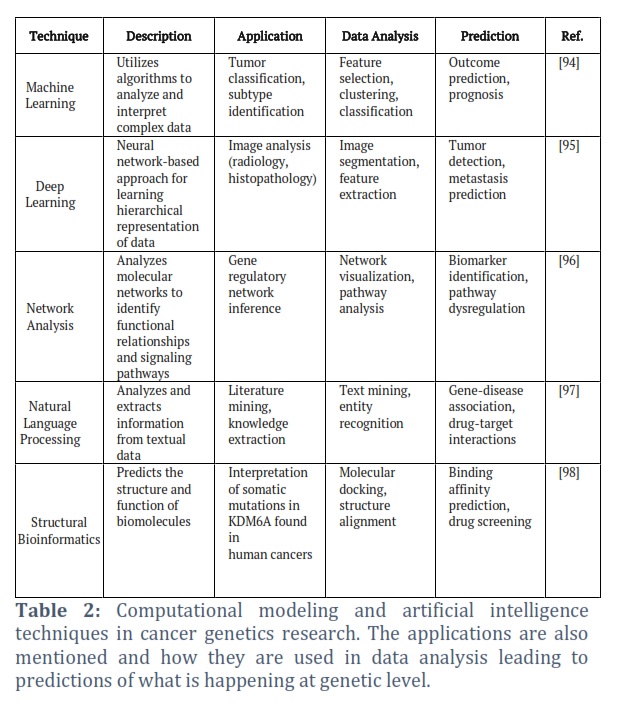
Computational modeling and artificial intelligence (AI) have emerged as indispensable tools in cancer genetics research, offering powerful methods for analyzing complex biological data, predicting disease outcomes, and guiding therapeutic strategies. Computational modeling encompasses a diverse range of mathematical, statistical, and computational techniques for simulating biological systems, modeling molecular interactions, and predicting cellular behaviours [92]. By integrating multiomic data, network analysis, and machine learning algorithms, computational models can elucidate the molecular mechanisms underlying cancer progression, metastasis, and treatment response. Artificial intelligence techniques, containing deep learning, neural networks, & natural language processing, have revolutionized cancer genetics research by enabling the analysis of large-scale genomic datasets, electronic health records, and biomedical literature with unprecedented speed and accuracy [88] (Table 2). AI-driven approaches have been applied to various aspects of cancer genetics, including tumor classification, biomarker discovery, drug repurposing, and patient stratification, leading to the identification of novel therapeutic targets & personalized treatment regimens. Moreover, computational models and AI algorithms can integrate diverse data modalities, such as genomics, imaging, and clinical data, to provide holistic insights into tumor biology and patient outcomes. As computational capabilities continue to advance and genomic datasets grow in complexity and scale, computational modeling and AI-driven approaches are poised to play increasingly prominent roles in cancer genetics research, transforming our indulgent of cancer biology & guiding the development of precision oncology strategies [93].
Tables and Figures
Looking ahead, the field of cancer genetics is poised for exciting advancements that hold the promise of reshaping our approach to cancer prevention, diagnosis, and treatment. As genomic technologies continue to evolve, we anticipate a deeper understanding of the genetic drivers of cancer, including rare & understudied variants. The integration of multi-omics data, such as genomics, transcriptomics, proteomics, & metabolomics, will afford a more complete opinion of the molecular landscape of cancer, paving the way for novel therapeutic strategies and biomarker discovery. For instance, a recent study expected to develop a DNA methylation biomarker for predicting the prognosis of colorectal cancer (CRC). Using data from Illumina EPIC methylation arrays, hypermethylated genes in CRC tissue were identified. A cohort of 30 pairs of tumor & nearby normal tissue was used to correlate the methylation status of the identified marker with its expression. Another cohort of 254 CRC patients' formalin-fixed paraffin-embedded (FFPE) tumor tissue was used for prognosis analysis. The study found that regulating synaptic membrane exocytosis 2 (RIMS2) was hypermethylated & expressed at low levels in CRC likened to contiguous normal tissue. Hypermethylation of RIMS2 correlated with less frequent KRAS mutation & higher differentiation. RIMS2 promoter methylation independently predicted survival outcomes, with an arrangement of RIMS2 methylation & KRAS status improving prognosis prediction. The findings suggest that RIMS2 hypermethylation is a novel biomarker for expecting CRC prognosis [99, 100].
Furthermore, the era of precision medicine holds tremendous potential for personalized cancer care, with the identification of actionable genetic alterations guiding targeted therapies and immunotherapies. As we move towards a more patient-centric model of cancer treatment, efforts to overcome therapeutic resistance and enhance treatment efficacy will be paramount. Combination therapies targeting multiple pathways and exploiting synthetic lethal interactions offer promise in overcoming resistance mechanisms and improving patient outcomes. In parallel, advances in computational biology and artificial intelligence are poised to revolutionize cancer genetics research and clinical practice. Machine learning algorithms can analyze vast amounts of genomic data to find patterns, predict treatment responses, and stratify patients based on their molecular profiles. Additionally, the application of AI-driven drug discovery platforms holds potential for the rapid identification of innovative therapeutic targets & the development of more actual anticancer agents.
Moreover, as our understanding of cancer genetics continues to deepen, there will be a growing emphasis on precision prevention strategies aimed at identifying individuals at high risk of developing cancer and implementing targeted interventions to reduce their risk. This includes lifestyle modifications, chemoprevention strategies, and early detection modalities tailored to an individual's genetic predisposition. Ethical considerations neighbouring genetic testing, data privacy & equitable access to genomic technologies will remain critical as the field progresses. Ensuring that the benefits of genomic medicine are accessible to all populations, regardless of socioeconomic status or geographic location will be essential to addressing health disparities and achieving global cancer control.
In conclusion, the future of cancer genetics holds immense promise for revolutionizing cancer care and improving patient outcomes. By leveraging the power of genomics, computational biology, and precision medicine, we can unravel the complications of cancer biology, develop more effective treatments, & ultimately, transform the landscape of cancer prevention and management. As we continue to push the boundaries of scientific discovery, collaboration across disciplines and international borders will be key to realizing the full potential of genomic medicine in the fight against cancer.
In conclusion, our review has illuminated the complex genetic landscape of cancer, showcasing the pivotal role of genetic alterations in driving tumorigenesis. Through decades of research, we have gained profound understandings into the molecular mechanisms fundamental oncogenic transformation, from the dysregulation of oncogenes & tumor suppressor genes to the intricate interplay of signaling pathways. The advent of genomic technologies has revolutionized our understanding of cancer genetics, enabling unprecedented insights into tumor heterogeneity, clonal evolution, and therapeutic resistance. Moving forward, the assimilation of genomic data into clinical exercise holds tremendous promise for precision oncology, facilitating the development of customized targeted therapy to the unique genetic profiles of individual tumors. Furthermore, advances in genetic testing and counseling offer opportunities for early detection and personalized risk assessment, enhancing cancer prevention and management strategies. However, challenges such as therapeutic resistance and ethical considerations persist, underscoring the need for continued research and interdisciplinary collaboration.
Acnowledgement
The authors extend their appreciation to the Deanship of Graduate Studies and Scientific Research at University of Bisha for funding this research through the general research project under grant number (UB-GRP- 39 -1444).
Author Contributions
A A: Prepare the first draft and data analysis; AAA: Revised and editing of the manuscript; MHA: revision and language editing of the manuscript.
The authors are thankful to the Deanship of Graduate Studies and Scientific Research at the University of Bisha for supporting this work through the Fast-Track Research Support Program.
![]() References
References
- Labi V, Erlacher M. How cell death shapes cancer. Cell death & disease, (2015); 6(3): e1675-e1675.
- Torre LA, Siegel RL, Ward EM, Jemal A. Global cancer incidence and mortality rates and trends-an update. Cancer epidemiology, biomarkers & prevention, (2016); 25(1): 16-27.
- Więckiewicz G, Weber S, Florczyk I, Gorczyca P. Socioeconomic Burden of Psychiatric Cancer Patients: A Narrative Review. Cancers, (2024); 16(6): 1108.
- Botezatu A, Iancu IV, Popa O, Plesa A, Manda D, Huica I, et al. Mechanisms of oncogene activation. New aspects in molecular and cellular mechanisms of human carcinogenesis, (2016); 9(1).
- Joyce C, Rayi A, Kasi A. Tumor-suppressor genes. (2018).
- Chen X, Agustinus AS, Li J, DiBona M, Bakhoum SF. Chromosomal instability as a driver of cancer progression. Nature Reviews Genetics, (2024); 1-16.
- Reis AH, Vargas FR, Lemos B. Biomarkers of genome instability and cancer epigenetics. Tumor Biology, (2016); 37(10): 13029-13038.
- Bashraheel SS, Domling A, Goda SK. Update on targeted cancer therapies, single or in combination, and their fine tuning for precision medicine. Biomedicine & Pharmacotherapy, (2020); 125: 110009.
- Wade CA, Kyprianou N. Profiling prostate cancer therapeutic resistance. International journal of molecular sciences, (2018); 19(3): 904.
- Kensler TW, Spira A, Garber JE, Szabo E, Lee JJ, Dong Z, et al. Transforming cancer prevention through precision medicine and immune-oncology. Cancer Prevention Research, (2016); 9(1): 2-10.
- Weiss RA. A perspective on the early days of RAS research. Cancer and Metastasis Reviews, (2020); 39(4): 1023-1028.
- Ostlund A. The Translocation t (7; 12) (q36; p13) in Childhood Acute Myeloid Leukemia. (2024).
- Ellsworth DL, Blackburn HL, Shriver CD, Rabizadeh S, Soon-Shiong P, Ellsworth R E. Single-cell sequencing and tumorigenesis: improved understanding of tumor evolution and metastasis. Clinical and translational medicine, (2017); 6(1): 15.
- Cooper LA, Demicco EG, Saltz JH, Powell RT, Rao A, Lazar AJ. Pan Cancer insights from The Cancer Genome Atlas: the pathologist's perspective. The Journal of pathology, (2018); 244(5): 512-524.
- Jarhelle E, Riise Stensland HMF, Hansen GAM, Skarsfjord S, Jonsrud C, Ingebrigtsen M, et al. Identifying sequence variants contributing to hereditary breast and ovarian cancer in BRCA1 and BRCA2 negative breast and ovarian cancer patients. Scientific reports, (2019); 9(1): 19986.
- Sun K, Luo J, Guo J, Yao X, Jing X, Guo F. The PI3K/AKT/mTOR signaling pathway in osteoarthritis: a narrative review. Osteoarthritis and cartilage, (2020); 28(4): 400-409.
- Morganti S, Tarantino P, Ferraro E, D’Amico P, Viale G, et al. Complexity of genome sequencing and reporting: Next generation sequencing (NGS) technologies and implementation of precision medicine in real life. Critical reviews in oncology/hematology, (2019); 133, 171-182.
- Goleva E, Lyubchenko T, Kraehenbuehl L, Lacouture ME, Leung DY, Kern JA. Our current understanding of checkpoint inhibitor therapy in cancer immunotherapy. Annals of Allergy, Asthma & Immunology, (2021); 126(6): 630-638.
- Klempner SJ, Fabrizio D, Bane S, Reinhart M, Peoples T, Ali SM, et al. Tumor mutational burden as a predictive biomarker for response to immune checkpoint inhibitors: a review of current evidence. The oncologist, (2020); 25(1): e147-e159.
- Sanchez-Vega F, Mina M, Armenia J, Chatila WK, Luna A, La KC, et al. Oncogenic signaling pathways in the cancer genome atlas. Cell, (2018); 173(2): 321-337.
- Cicirò Y, Sala A. MYB oncoproteins: emerging players and potential therapeutic targets in human cancer. Oncogenesis, (2021); 10(2): 19.
- Hamid AA, Gray KP, Shaw G, MacConaill LE, Evan C, Bernard B, et al. Compound genomic alterations of TP53, PTEN, and RB1 tumor suppressors in localized and metastatic prostate cancer. European urology, (2019); 76(1): 89-97.
- Alhmoud JF, Woolley JF, Al Moustafa AE, Mallei MI. DNA damage/repair management in cancers. Advances in Medical Biochemistry, Genomics, Physiology, and Pathology, (2021); 309-339.
- Kontomanolis EN, Koutras A, Syllaios A, Schizas D, Mastoraki A, Garmpis N, et al. Role of oncogenes and tumor-suppressor genes in carcinogenesis: a review. Anticancer research, (2020); 40(11): 6009-6015.
- Cuesta C, Arévalo-Alameda C, Castellano E. The importance of being PI3K in the RAS signaling network. Genes, (2021); 12(7): 1094.
- Pertesi M, Ekdahl L, Palm A, Johnsson E, Jarvstrat L, Wihlborg A-K, et al. Essential genes shape cancer genomes through linear limitation of homozygous deletions. Communications Biology, (2019); 2(1): 262.
- Lipsick J. A history of cancer research: tumor suppressor genes. Cold Spring Harbor Perspectives in Biology, (2020); 12(2): a035907.
- Volkova NV, Meier B, González-Huici V, Bertolini S, Gonzalez S, Vohringer H, et al. Mutational signatures are jointly shaped by DNA damage and repair. Nature communications, (2020); 11(1): 2169.
- Yoshioka KI, Kusumoto-Matsuo R, Matsuno Y, Ishiai M. Genomic instability and cancer risk associated with erroneous DNA repair. International journal of molecular sciences, (2021); 22(22): 12254.
- Jiang Z, Gu Z, Lu X, Wen W. The role of dysregulated metabolism and associated genes in gastric cancer initiation and development. Translational Cancer Research, (2024); 13(7): 3854.
- Fueyo R, Judd J, Feschotte C, Wysocka J. Roles of transposable elements in the regulation of mammalian transcription. Nature reviews Molecular cell biology, (2022); 23(7): 481-497.
- Diederichs S, Bartsch L, Berkmann JC, Frose K, Heitmann J, Hoppe C, et al. The dark matter of the cancer genome: aberrations in regulatory elements, untranslated regions, splice sites, non‐coding RNA and synonymous mutations. EMBO molecular medicine, (2016); 8(5): 442-457.
- Yang Z, Xu F, Wang H, Teschendorff AE, Xie F, He Y. Pan-cancer characterization of long non-coding RNA and DNA methylation mediated transcriptional dysregulation. EBioMedicine, (2021); 68.
- Meier K, Recillas-Targa F. New insights on the role of DNA methylation from a global view. Front Biosci (Landmark Ed), (2017); 22(4): 644-668.
- Zaib S, Rana N, Khan I. Histone modifications and their role in epigenetics of cancer. Current medicinal chemistry, (2022); 29(14): 2399-2411.
- Liu X, Liu H. Changing expression profiles of messenger RNA, microRNA, long non-coding RNA, and circular RNA reveal the key regulators and interaction networks of competing endogenous RNA in pulmonary fibrosis. Frontiers in Genetics, (2020); 11: 558095.
- Ackerman S, Horton W. Effects of environmental factors on DNA: damage and mutations. In Green Chemistry (2018); (109-128). Elsevier.
- Khan AQ, Kuttikrishnan S, Siveen KS, Prabhu KS, Shanmugakonar M, Al-Naemi HA, et al. RAS-mediated oncogenic signaling pathways in human malignancies. In Seminars in cancer biology, (2019); 54,1-13.
- Wang LH, Wu CF, Rajasekaran N, Shin YK. Loss of tumor suppressor gene function in human cancer: an overview. Cellular Physiology and Biochemistry, (2019); 51(6): 2647-2693.
- Ray A. DNA Mutation, Repair, and Recombination. In Genetics Fundamentals Notes (2022); 433-490. Singapore: Springer Nature Singapore.
- Luatti S, Baldazzi C, Marzocchi G, Ameli G, Bochicchio MT, Soverini S, et al. Cryptic BCR-ABL fusion gene as variant rearrangement in chronic myeloid leukemia: molecular cytogenetic characterization and influence on TKIs therapy. Oncotarget, (2017); 8(18): 29906.
- Glenfield C, Innan H. Gene duplication and gene fusion are important drivers of tumourigenesis during cancer evolution. Genes, (2021); 12(9): 1376.
- Zhang X, Sjoblom T. Targeting loss of heterozygosity: a novel paradigm for cancer therapy. Pharmaceuticals, (2021); 14(1): 57.
- Postwala H, Shah Y, Parekh PS, Chorawala MR. Unveiling the genetic and epigenetic landscape of colorectal cancer: New insights into pathogenic pathways. Medical Oncology, (2023); 40(11): 334.
- Pathak GA, Polimanti R, Silzer TK, Wendt FR, Chakraborty R, Phillips NR. Genetically-regulated transcriptomics & copy number variation of proctitis points to altered mitochondrial and DNA repair mechanisms in individuals of European ancestry. BMC cancer, (2020); 20: 1-13.
- Asgari-Karchekani S, Aryannejad A, Mousavi SA, Shahsavarhaghighi S, Tavangar S M. The role of HER2 alterations in clinicopathological and molecular characteristics of breast cancer and HER2-targeted therapies: a comprehensive review. Medical Oncology, (2022); 39(12): 210.
- Nabavi S, Zare F. Identification of copy number alterations from next-generation sequencing data. Computational Methods for Precision Oncology, (2022); 55-74.
- Bhattacharya P, Patel TN. Microsatellite instability and promoter hypermethylation of DNA repair genes in hematologic malignancies: a forthcoming direction toward diagnostics. Hematology, (2018); 23(2): 77-82.
- Zhang J, Yang C, Wu C, Cui W, Wang L. DNA methyltransferases in cancer: biology, paradox, aberrations, and targeted therapy. Cancers, (2020); 12(8): 2123.
- Aubrey BJ, Strasser A, Kelly GL. Tumor-suppressor functions of the TP53 pathway. Cold Spring Harbor perspectives in medicine, (2016); 6(5): a026062.
- Capuozzo M, Santorsola M, Bocchetti M, Perri F, Cascella M, Granata V, et al. p53: from fundamental biology to clinical applications in cancer. Biology, (2022); 11(9): 1325.
- Alvarado-Ortiz E, de la Cruz-López KG, Becerril-Rico J, Sarabia-Sánchez MA, Ortiz-Sánchez E, García-Carrancá A. Mutant p53 gain-of-function: role in cancer development, progression, and therapeutic approaches. Frontiers in cell and developmental biology, (2021); 8: 607670.
- Li Q, Engebrecht J. BRCA1 and BRCA2 tumor suppressor function in meiosis. Frontiers in Cell and Developmental Biology, (2021); 9: 668309.
- Petrucelli N, Daly MB, Pal T. BRCA1-and BRCA2-associated hereditary breast and ovarian cancer. (2022); (5): 245-59.
- Fanale D, Pivetti A, Cancelliere D, Spera A, Bono M, Fiorino A, et al. BRCA1/2 variants of unknown significance in hereditary breast and ovarian cancer (HBOC) syndrome: looking for the hidden meaning. Critical Reviews in Oncology/Hematology, (2022); 172: 103626.
- Papa A, Pandolfi PP. The PTEN–PI3K axis in cancer. Biomolecules, (2019); 9(4): 153.
- Chang H, Cai Z, Roberts TM. The mechanisms underlying PTEN loss in human tumors suggest potential therapeutic opportunities. Biomolecules, (2019); 9(11): 713.
- Vidotto T, Melo CM, Castelli E, Koti M, Dos Reis RB, Squire JA. Emerging role of PTEN loss in evasion of the immune response to tumours. British journal of cancer, (2020); 122(12): 1732-1743.
- Kolch W, Berta D, & Rosta E. Dynamic regulation of RAS and RAS signaling. Biochemical Journal, (2023); 480(1): 1-23.
- Ullah R, Yin Q, Snell AH, Wan L. RAF-MEK-ERK pathway in cancer evolution and treatment. Seminars in cancer biology, (2022); 85: 123-154.
- Dillon M, Lopez A, Lin E, Sales D, Perets R, Jain P. Progress on Ras/MAPK signaling research and targeting in blood and solid cancers. Cancers, (2021); 13(20): 5059.
- Stefani C, Miricescu D, Stanescu-Spinu II, Nica RI, Greabu M, Totan AR, Jinga M. Growth factors, PI3K/AKT/mTOR and MAPK signaling pathways in colorectal cancer pathogenesis: where are we now? International Journal of Molecular Sciences, (2021); 22(19): 10260.
- Peng Y, Wang Y, Zhou C, Mei W, Zeng C. PI3K/Akt/mTOR pathway and its role in cancer therapeutics: are we making headway? Frontiers in oncology, (2022); 12: 819128.
- M Sokolowski K, Koprowski S, Kunnimalaiyaan S, Balamurugan M, Clark Gamblin T, Kunnimalaiyaan M. Potential molecular targeted therapeutics: role of PI3-K/Akt/mTOR inhibition in cancer. Anti-Cancer Agents in Medicinal Chemistry (Formerly Current Medicinal Chemistry-Anti-Cancer Agents), (2016); 16(1): 29-37.
- Piombino C, Cortesi L, Lambertini M, Punie K, Grandi G, Toss A. Secondary prevention in hereditary breast and/or ovarian cancer syndromes other than BRCA. Journal of Oncology, (2020); 2020: 6384190.
- Jackson L, Weedon MN, Green HD, Mallabar-Rimmer B, Harrison JW, Wood AR, Wright CF. Influence of family history on penetrance of hereditary cancers in a population setting. EClinicalMedicine, (2023); 64: 102159.
- Schneider KA, Chittenden A, Shannon KM. Counseling about cancer: strategies for genetic counseling. John Wiley & Sons. (2023).
- Samadder NJ, Riegert-Johnson D, Boardman L, Rhodes D, Wick M, Okuno S, et al. Comparison of universal genetic testing vs guideline-directed targeted testing for patients with hereditary cancer syndrome. JAMA oncology, (2021); 7(2): 230-237.
- Assenov Y, Brocks D, Gerhäuser C. Intratumor heterogeneity in epigenetic patterns. In Seminars in cancer biology, (2018); 51: 12-21.
- Turnquist C, Watson RA, Protheroe A, Verrill C, Sivakumar S. Tumor heterogeneity: does it matter? Expert Review of Anticancer Therapy, (2019); 19(10): 857-867.
- Apostoli AJ, Ailles L. Clonal evolution and tumor-initiating cells: new dimensions in cancer patient treatment. Critical reviews in clinical laboratory sciences, (2016); 53(1): 40-51.
- Anupriya S, Chakraborty A, Patnaik S. Clonal evolution and expansion associated with therapy resistance and relapse of colorectal cancer. Mutation Research/Reviews in Mutation Research, (2022); 790: 108445.
- Malone ER, Oliva M, Sabatini PJ, Stockley TL, Siu LL. Molecular profiling for precision cancer therapies. Genome medicine, (2020); 12: 1-19.
- Vlachostergios PJ, Faltas BM. Treatment resistance in urothelial carcinoma: an evolutionary perspective. Nature reviews Clinical oncology, (2018); 15(8): 495-509.
- Proietto M, Crippa M, Damiani C, Pasquale V, Sacco E, Vanoni M, et al. Tumor heterogeneity: preclinical models, emerging technologies, and future applications. Frontiers in Oncology, (2023); 13: 1164535.
- Sabour L, Sabour M, Ghorbian S. Clinical applications of next-generation sequencing in cancer diagnosis. Pathology & Oncology Research, (2017); 23: 225-234.
- Dhanjal DS, Chopra C, Chopra RS. Metagenomic DNA sequencing: technological advances and applications. Metagenomics: Techniques, Applications, Challenges and Opportunities, (2020); 37-53.
- Qiu T, Zhi X, Ren S. Recent advance of next-generation sequencing in patients with lung cancer. Expert Review of Molecular Diagnostics, (2023); 23(11): 959-970.
- Colomer R, Miranda J, Romero-Laorden N, Hornedo J, González-Cortijo L, Mouron S, et al. Usefulness and real-world outcomes of next generation sequencing testing in patients with cancer: an observational study on the impact of selection based on clinical judgement. EClinicalMedicine, (2023); 60: 102029. 60.
- Ren X, Kang B, Zhang Z. Understanding tumor ecosystems by single-cell sequencing: promises and limitations. Genome biology, (2018); 19(1): 211
- Lei Y, Tang R, Xu J, Wang W, Zhang B, Liu J, et al. Applications of single-cell sequencing in cancer research: progress and perspectives. Journal of hematology & oncology, (2021); 14(1): 91.
- Dutta AK, Alberge JB, Sklavenitis-Pistofidis R, Lightbody ED, Getz G, Ghobrial IM. Single-cell profiling of tumour evolution in multiple myeloma-opportunities for precision medicine. Nature Reviews Clinical Oncology, (2022); 19(4): 223-236.
- Lim J, Chin V, Fairfax K, Moutinho C, Suan D, Ji H, et al. Transitioning single-cell genomics into the clinic. Nature Reviews Genetics, (2023); 24(8): 573-584.
- Joshi A, Kumar A, Kaushik V. Functional Genomics and Network Biology. In Advances in Bioinformatics (2024); 71-96).
- Wang C, Cao Y, Yang C, Bernards R. Exploring liver cancer biology through functional genetic screens. Nature reviews Gastroenterology & hepatology, (2021); 18(10): 690-704.
- Salvati A, Gigantino V, Nassa G, Mirici Cappa V, Ventola GM, Cracas DGC, et al. Global view of candidate therapeutic target genes in hormone-responsive breast cancer. International journal of molecular sciences, (2020); 21(11): 4068.
- Jiang C, Meng L, Yang B, Luo X. Application of CRISPR/Cas9 gene editing technique in the study of cancer treatment. Clinical genetics, (2020); 97(1): 73-88.
- Zhang G, Wang Z, Qian F, Zhao C, Sun C. Silencing of the ABCC4 gene by RNA interference reverses multidrug resistance in human gastric cancer. Oncology reports, (2015); 33(3): 1147-1154.
- Przybyla L, Gilbert LA. A new era in functional genomics screens. Nature Reviews Genetics, (2022); 23(2): 89-103.
- Corces MR, Granja JM, Shams S, Louie BH, Seoane JA, Zhou W, et al. The chromatin accessibility landscape of primary human cancers. Science, (2018); 362(6413): eaav1898.
- Bludau I, Aebersold R. Proteomic and interactomic insights into the molecular basis of cell functional diversity. Nature Reviews Molecular Cell Biology, (2020); 21(6): 327-340.
- Patil VM, Gupta SP, Masand N, Balasubramanian K. Experimental and computational models to understand protein-ligand, metal-ligand and metal-DNA interactions pertinent to targeted cancer and other therapies. European Journal of Medicinal Chemistry Reports, (2024); 100133.
- Xu J, Yang P, Xue S, Sharma B, Sanchez-Martin M, Wang F, Parikh B. Translating cancer genomics into precision medicine with artificial intelligence: applications, challenges and future perspectives. Human genetics, (2019); 138(2): 109-124.
- Sebastian AM, Peter D. Artificial intelligence in cancer research: trends, challenges and future directions. Life, (2022); 12(12): 1991.
- Xie T, Wang Z, Zhao Q, Bai Q, Zhou X, Gu Y, Wang H. Machine learning-based analysis of MR multiparametric radiomics for the subtype classification of breast cancer. Frontiers in oncology, (2019); 9: 505.
- Chen R, Yang L, Goodison S, Sun Y. Deep-learning approach to identifying cancer subtypes using high-dimensional genomic data. Bioinformatics, (2020); 36(5): 1476-1483.
- Tong YF, He QE, Zhu JX, Ding EC, Song K. Multi‐omics differential gene regulatory network inference for lung adenocarcinoma tumor progression biomarker discovery. AIChE Journal, (2022); 68(4): e17574.
- Ding P, Pan Y, Wang Q, Xu R. Prediction and evaluation of combination pharmacotherapy using natural language processing, machine learning and patient electronic health records. Journal of Biomedical Informatics, (2022); 133: 104164.
- Chi YI, Stodola TJ, De Assuncao TM, Leverence EN, Smith BC, Volkman BF, et al. Structural bioinformatics enhances the interpretation of somatic mutations in KDM6A found in human cancers. Computational and Structural Biotechnology Journal, (2022); 20: 2200-2211.
- Li X, Cai D, Huang Y, Xie Y, Shen D, Yuan Z, Wang X. Aberrant methylation in neurofunctional gene serves as a hallmark of tumorigenesis and progression in colorectal cancer. BMC cancer, (2023); 23(1): 315.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


