

Full Length Research Article
Immunohistochemical expression of Annexin A2 and Annexin A6 in a random sample group of Iraqi women with triple-negative breast cancer
Hadjir Saad Sulaiman*, Hiba Ahmed Gaidan, Raghad Hanoon Zamil
Adv. life sci., vol. 12, no. 1, pp. 250-254, February 2025
*- Corresponding Author: Hadjer Saad Sulayman (Email: haider.k.abaas@gmail.com)
Authors' Affiliations
[Date Received: 14/06/2023; Date Revised: 19/07/2024; Date Published: 31/12/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Breast cancer represents the most common and the first leading cause of cancer-associated deaths in Iraqi women. It is a heterogeneous disease with different subtypes; one of these subtypes is triple-negative (basal-like) breast cancer, which is characterized by a distinctive molecular profile, aggressive clinical behavior, and the absence of targeted therapies. Annexin A2 and Annexin A6 are part of the Annexin protein family; these proteins have a suggested role in the evolution and progression of many cancer types, including breast cancer. Evaluation of the immunohistochemical expression of Annexin A2 and Annexin A6 in triple-negative subtype) in a random sample group of Iraqi women patients and correlating the results with clinicopathological parameters, including tumor grade and stage.
Methods: The current study was conducted in Baghdad /Iraq, in which forty paraffin-embedded blocks of breast tissue from women patients diagnosed with breast cancer were collected and selected to be triple-negative breast cancer. Immunohistochemical staining of Annexin A2 and Annexin A6 markers was performed for this sample with a correlation of the results with clinicopathological parameters, including tumor grade and stage.
Results: The study demonstrates a significant association between Annexin A2 and Annexin A6 expression and a significant association between Annexin A2 expression and tumor grade and stage in triple-negative breast cancer in this group of Iraqi patients.
Conclusions: This study displays the role of Annexin A2 and Annexin A6 in triple-negative breast cancer and suggests the role of Annexin A2 in the progression, metastasis, and prognosis of this special type of breast cancer by its association with advanced tumor grade and stage.
Keywords: Annexin A2; Annexin A6; triple-negative; Breast cancer
Introduction![]()
Breast cancer represents the most common and leading cause of cancer-related deaths in Iraqi women [1]. Breast cancer is now regarded as a heterogeneous disease with different molecular subtypes. The advances in breast cancer molecular studies and classification result in the recognition of three main molecular markers: the estrogen receptor, the progesterone receptor, and the type 2 human epidermal growth factor receptor [2, 3]. This classification assorts breast cancer into the main three molecular subtypes: ER+ and/or PR+ (luminal), HER2+, and triple-negative (basal-like) breast cancer [4]. Triple-negative breast cancer is characterized by a distinctive molecular profile, special metastasis patterns, aggressive behavior, and the absence of targeted therapy [5]. According to these subtypes and other clinicopathological features like age, tumor size, grade, and stage, the decision for the type of treatment and prognosis of breast cancer will be determined [6]. The clinical outcome of breast cancer remains unsatisfactory despite the efforts made to improve therapy strategies due to the recurrence and metastasis of the disease So, there is a great need for the development and establishment of noninvasive biomarkers that can be detected easily and have significant importance in the treatment, follow up and prognosis of breast cancer. Annexin A2 and Annexin A6 were from these biomarkers. The Annexin family represents one of the largest groups of calcium and phospholipid-binding proteins in the human body, consisting of more than 160 members [7]. Annexins play important roles in different physiological and cellular processes, including the synthesis of the cell cytoskeleton and membranes, endocytosis, exocytosis, and the formation of calcium ion channel 7. Annexin A is a subtype of the Annexin family, consisting of 12 members. Recent reports have also proposed the association between the Annexin A family and autophagy by suggesting that Annexin A can help in the regulation of exocytosis, and endocytosis [8, 9]. Annexin A2 represents part of the Annexin protein family; it is found on chromosome 15q22.2 and is expressed in macrophages, endothelial cells, mononuclear cells, and some types of tumors [10]. Annexin A2 has three functional regions: the terminal region (N), the terminal region(C), and core region. The terminal region (N) carries tissue plasminogen activator (TPA); the core region of Annexin A2 holds phospholipid and calcium binding sites; and the terminal region(C) carries heparin, F- actin and plasminogen binding sites [11]. Annexin A2 is overexpressed in invasive ductal breast carcinoma and in situ ductal carcinoma, suggesting an important role of Annexin A2 in breast cancer development [12]. Annexin A6 represents one of the largest members of the Annexin protein family; it is located on chromosomes 5q32–q34 [13]. Many studies suggest that Annexin A6 participates in actin cytoskeleton remodeling [14]. As with most members of the Annexin family, the translocation of Annexin A6 to the cell membrane occurs as a response to increased intracellular Ca+ that contributes to membrane microdomain remodeling and maintains plasma membrane integrity [15, 16]. Other recent advanced research has shown that Annexin A6 plays a major role in tumor cell growth, motility, adhesion, and cell membrane repair [17]. In this study, we evaluate the immunohistochemical expression of Annexin and Annexin A6 in breast cancer tissues of a random sample of Iraqi women diagnosed with breast cancer with triple-negative hormonal status (ER, PR, and HER2) and analyzes this expression in correlation with tumor grade and stage in this group of breast cancer patients.
Methods![]()
Ethical agreement
This study obtained approval from the College of Medicine/Al-Mustansiriyah University (1 Jun 2021, no.21), and consent was taken from patients to use their paraffin block samples.
Study design and sample criteria
In this retrospective study, breast tissue in paraffin-embedded blocks of a group of Iraqi women patients diagnosed with breast cancer was collected between the periods of January 2021 and June 2022 from archived materials from Al Yarmouk Teaching Hospital, Baghdad, Iraq. These paraffin blocks represented 40 cases of breast cancer; all cases were selected to be specimens of mastectomies. Cases included in this study had patients aged between 46 and 65 years with a mean of 54.7± 5.61 (SD) years. All cases were diagnosed as invasive ductal carcinoma of the breast. Clinicopathological parameters, including the age of patients, grade, and stage of the tumor, were obtained from the histopathologic reports and were independently reviewed by two histopathologists. Regarding tumor grade (according to the Nottingham Histological Grading System), ten cases were in grade Ⅰ, and fifteen cases were in grades 11 and Ⅲ. Concerning the tumor stage (according to the American Joint Committee on Cancer), the cases were divided into: nine cases in stage Ⅰ, eleven cases in stage 11, and 10 cases in each stage Ⅲ and stage Ⅳ, as shown in Tables 2 and 3. All cases were selected to be triple-negative (basal-like) breast cancer subtypes according to estrogen, progesterone, and her 2-receptors status at the time of diagnosis. Samples of normal breast tissue were taken from adjacent tissue from 10 cases of the same mastectomy specimens as a negative control. The positive control used in this study included tissue of a normal human liver for Annexin A2 and tissue of a normal human tonsil for Annexin A6 (according to kit leaflets) with each run.
Immunohistochemical staining procedures
Selected paraffin blocks of breast tissue samples were sectioned into 4 µm. From each block, 3 sections were taken: one section for hematoxylin and eosin, and two sections were prepared on positively charged slides for immunohistochemical staining with Annexin A2 and Annexin A6. Immunohistochemical staining was achieved by using the following antibodies: Annexin A2 (dilution 1: 100, Abcam; Code: 178677, rabbit monoclonal antibody) and Annexin A6 (dilution 1: 2000, Abcam; Code: 201023, rabbit monoclonal antibody). An automated system from Leica was used for all staining steps. Specimens were deparaffinized, and then antigen retrieval was done by using a microwave for about 20 minutes. All slides were incubated for about 15 minutes with the primary antibody, then for 10 minutes with the post-primary polymer, and were blocked for 4 minutes by hydrogen peroxide 3% and with brown chromogen for 10 minutes, followed by staining with counterstain (hematoxylin) for 5 minutes. All these steps of incubation were achieved at room temperature. Slides were washed with buffered saline between these steps, and coverslipping by DPX was performed.
Assessment of immunohistochemical results
In Annexin A2 and Annexin A6, the location of cellular staining is cytoplasmic, and membranous or only cytoplasmic brown staining was regarded as a positive result. The two markers are also expressed in stromal cells, but this expression was not included in the evaluation. The assessment of the intensity of staining was as follows: 0 as none; 1 as mild (0% to 5% of epithelial cells); 2 as moderate (more than 5% to 50%); and 3 as strong (more than 50% staining) [18].
Statistical analysis
The Statistical Package of Social Sciences (SPSS version 25) program was used in the statistical analysis of the results. The student test (t-test) was used for handling the quantitative data: Annexin A2+, Annexin A2–, Annexin A6+, Annexin A6‑, and controls. If required, absolute variables were evaluated by a Pearson Chi-squared analysis test with an ANOVA test. The p-value was considered to be significant if it was less than (0.05).
Results![]()
We investigate the immunohistochemical expression of Annexin A2 and Annexin A6 in 40 cases of triple-negative (basal-like) breast cancer in a random sample group of Iraqi patients and correlate the expression with tumor grade and stage. For both types of Annexin A, most cases show moderate to strong expression according to the selected scoring system (18).
Immunohistochemical expression of Annexin and Annexin A6
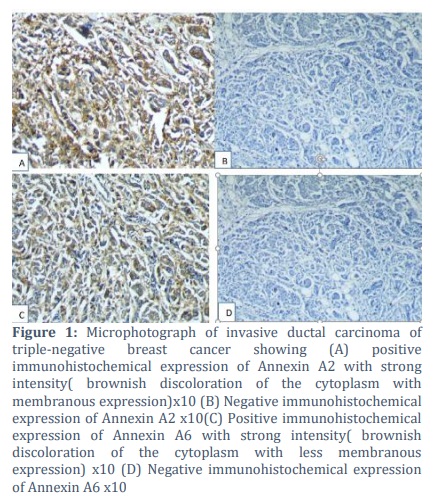
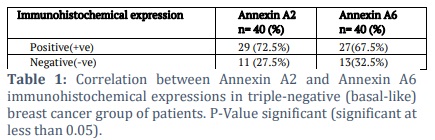
Regarding Annexin A2, there was a positive expression in 29 (72.5%) of cases, while 11 (27.5%) of cases show a negative expression (table 1, figures 1A, B). Annexin A6 shows positive expression in 27 (67.5%) of cases, while 13 (32.5%) of cases show negative expression (table 1, figures 1C, and D). There was a strong significant correlation between Annexin A2 and Annexin A6 expression in triple-negative breast cancer in this group of patients (P-value was highly significant at 0.005, regard significant if less than 0.05) (table 1).
Correlation between Annexin A2 expression and tumor grade and stage
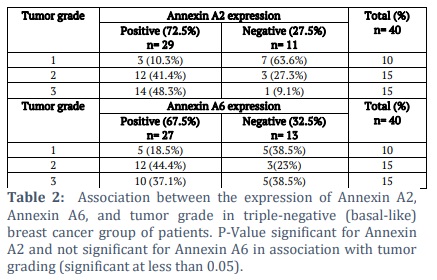
The correlation between Annexin A2 expression and the tumor histological grade was significant (P-value 0.008). Fourteen cases (48.3%) with positive expression were in grade Ⅲ of triple-negative breast cancer, twelve cases (41.4%) were in grade Ⅱ, and three cases (10.3%) were in grade I (table 2). The correlation between Annexin A2 expression and the tumor clinical stage was significant (P-value 0.007). The percentage of positive expression with Annexin A2 increased with more advanced stages (10.35% of positive cases were in stage Ⅰ, 24.15% of cases were in stage Ⅱ, 31% of cases were in stage Ⅲ, while 34.5% of cases were in stage Ⅳ), as shown in Table 3.
Correlation between Annexin A6 expression and tumor grade and stage
The correlation between Annexin A6 expression and tumor grade was not significant (P-value 0.09). Five cases (18.5%) showing positive expression were in grade Ⅰ, twelve cases (44.4%) were in grade Ⅱ, and ten cases (37.1%) were in grade Ⅲ (table 2). The association between Annexin A6 expression and stage was not significant (P-value 0.08). The percentage of positive expression with Annexin A6 was not associated with tumor stage (7.4% of positive cases were in stage Ⅰ, 33.3% of cases were in stage Ⅱ, 29.65% of cases were in stage Ⅲ, while 29.65% of cases were in stage Ⅳ), as shown in Table 3.
Figures & Tables
Breast cancer represents the most frequent cancer in Iraqi women, and it is the first leading cause of cancer deaths among them. We investigate Annexin A2 and Annexin A6 due to their studied rules in the evolution and progression of different types of tumors, including breast cancer, selecting triple-negative (basal-like) breast cancer because of its aggressive behavior. The current study shows a positive expression of Annexin A2 in 72.5% of cases, the percentage of expression in the current study was higher in comparison with a previous study (positive in 54.54% of cases) by Lee, Kelsey M., Sayantan, et al. (2021) [19] and Lee and Jamboor (2017) [20].
Regarding Annexin A6 expression, this study shows positive expression in 67.5% of cases; this result agrees with a past study by Amos, Rainelli, Bobby, et al. (2010) [21]. The correlation between Annexin A2 and Annexin A6 expression in triple-negative breast cancer was significant in the investigated group of patients, suggesting the importance of these two markers in the development of this type of cancer. There was no previous study showing the correlation between these two markers in triple-negative breast cancer. There is a significant correlation between Annexin A2 expression and the tumor histological grade; we found that increases in expression were associated with a higher grade, while the correlation between Annexin A6 expression and the tumor histological grade was not significant, as shown in Table 2. There is a significant correlation between Annexin A2 expression and tumor stage; a positive expression is associated with advanced tumor stage, while no significant association was found between Annexin A6 expression and tumor stage, as shown in Table 3.
The results of the current study show that Annexin A2 expression in triple-negative breast cancer significantly correlates with progression, metastasis, and the poor clinical outcome and prognosis of the tumor, while Annexin A6 expression does not correlate with tumor grade or stage. This finding suggests that the investigation of Annexin A2 immunohistochemical expression may be a useful non-invasive biomarker that correlates with aggressive tumor behavior and poor prognosis and may introduce Annexin A2 as a possible new therapeutic target in this type of aggressive cancer. The limitation of this study is that we need a larger sample size and investigation of these two markers on other molecular types of breast cancer with follow-up of patients.
This study investigates the role of Annexin A2 and Annexin A6 in one of the most clinically aggressive subtypes of breast cancer, triple-negative breast cancer, and demonstrates the significant association of Annexin A2 and Annexin A6 expression in this type of cancer, and the significant association of Annexin A2 expression with tumor grade and stage. The expression is higher in the higher grade and advanced stage, which suggests the important role of Annexin A2 in the progression, metastasis, and prognosis of triple-negative breast cancer.
Author Contributions
Study design: Hadjir S.Sulaiman, Hiba A. Gaidan
Performing IHC procedures: Hadjir S.Sulaiman, Hiba A. Gaidan, Raghad H. Zamil
Acquisition, analysis and interpretation: Hadjir S.Sulaiman, Hiba A. Gaidan, Raghad H. Zamil
Writing and original draft preparation: Hadjir S.Sulaiman, Hiba A. Gaidan, Raghad H. Zamil
Reviewing and editing: Hiba A. Gaidan
The authors declare that there is no conflict of interestregarding the publication of this paper.
![]() References
References
- World Health Organization. International Agency for Research on Cancer. The Global Cancer Observatory , March (2021).
- Toss A, Cristofanilli M. Molecular characterization and targeted therapeutic approaches in breast cancer. Breast Cancer Research, (2015); 17:60.
- Millis Z, Gatalica Z, Winkler J, Vranic S, Kimbrough J, Reddy S, et al. Predictive biomarker profiling of> over 6,000 breast cancer patients shows heterogeneity in TNBC, with treatment implications. Clinical breast cancer, (2015); 15(6):473–481.
- Russo J. Molecular Classification of Breast Cancer. Breast Cancer Essentials, (2021); 33–38.
- Ensenyat-Mendez M, Llinàs-Arias P, Orozco J, Íñiguez-Muñoz S, Salomon M, Sesé B, et al. Current Triple-Negative Breast Cancer Subtypes: Dissecting the Most Aggressive Form of Breast Cancer. Frontiers in oncology, (2021); 16:11:681476.
- Tsang J, Tse G. Molecular classification of breast cancer. Advances in anatomic pathology, (2020); 27(1):27–35.
- Xi Y, Ju R, Wang Y. Roles of Annexin A protein family in autophagy regulation and therapy. Biomedicine and pharmacotherapy, (2020); 130(8):110591.
- Moreau K,Ghislat G ,Hochfeld W, Renna M ,Zavodszky E, Runwal G, et al. Transcriptional regulation of Annexin A2 promotes starvation-induced autophagy. Nature communication, (2015); 6(1): 1–12.
- Chen Y, Fang Y, Cheng Y, Lin C, Hsu L, Wang S, et al. Exophagy of Annexin A2 via RAB11, RAB8A, and RAB27A in IFN-gamma-stimulated lung epithelial cells. Scientific reports, (2017); 7(1):5676.
- Wang C, Lin C. Annexin A2: Its Molecular Regulation and Cellular Expression in Cancer Development. Disease markers, (2014); 4: 308976.
- Sharma M. Annexin A2 (ANX A2): An emerging biomarker and potential therapeutic target for aggressive cancers. International Journal of Cancer, (2019); 1; 144(9):2074-2081.
- Mussunoor S, Murray G. The role of annexins in tumor development and progression. Journal of Pathology, (2008); 216:131–140.
- Enrich C, Rentero C, Grewal T. Annexin A6 in the liver: from the endocytic compartment to cellular physiology. Biochimica et Biophysica Acta (BBA): Molecular Cell Research, (2017); 1864 (6): 933–946.
- Koese M, Rentero C, Kota B, Hoque M, Cairns R, Wood P, et al. Annexin A6 is a scaffold for PKC alpha to promote EGFR inactivation. Oncogene, (2013); 32: 2858–2872.
- Creutz C, Hira J, Gee V, Eaton J. Protection of the membrane permeability barrier by Annexins. Biochemistry, (2012); 51:9966-9983.
- Alvarez-Guaita A, Vilà de Muga S, Owen D, Williamson D, Magenau A, García-Melero A, et al. Evidence for Annexin A6 dependent plasma membrane remodeling of lipid domains. British Journal of Pharmacology, (2015); 172:1677-1690.
- Boye T, Maeda K, Pezeshkian W, Sønder S, Haeger S, Gerke V, et al. Annexin A4 and A6 induce membrane curvature and constriction during cell membrane repair. Nature Communication, (2017); 8:1623.
- Chand P, Garg A, Singla V, Rani N. Evaluation of the Immunohistochemical Profile of Breast Cancer for Prognostics and Therapeutic Use. Nigerian Journal of Surgery, (2018); 24(2): 100–106.
- Gibbs L, Mansheim K, Maji S, Nandy R, Lewis C, Vishwanatha J, et al. Clinical Significance of Annexin A2 Expression in Breast Cancer Patients. Cancers, (2021); 13(1): 2.
- Gibbs L, Vishwanatha J. Prognostic impact of AnxA1 and AnxA2 gene expression in triple-negative breast cancer, (2018); 9:2697-2704.
- Sakwe A, Koumangoye R, Guillory B, Ochieng J. Annexin A6 contributes to the invasiveness of breast carcinoma cells by influencing the organization and localization of functional focal adhesions. Excremental cell research, (2001); 317(6): 823–837.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0![]()


