

Full Length Research Article
Evaluating the Self-Care Efficacy and Needs of Cancer Patients Experiencing Chemotherapy Side Effects
Santhi Muttipoll Dharmarajlu1*, Anuratha M D2
Adv. life sci., vol. 12, no. 1, pp. 127-133, February 2025
*- Corresponding Author: Santhi Muttipoll Dharmarajlu (Email: srajalu@jazanu.edu.sa)
Authors' Affiliations
2. PSG Hospitals, Coimbatore(Affiliated with The Tamil Nadu Dr. MGR Medical University, Chennai) Tamil Nadu – India
[Date Received: 16/05/2024; Date Revised: 25/11/2024; Date Published: 31/12/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Chemotherapy involves the strategic use of chemotherapeutic agents to manage cancer. While effective, it can harm healthy cells, leading to adverse effects. Our study aims to identify the self-care gaps faced by cancer patients and provide them with the essential knowledge, skills, and support to manage their condition effectively.
Methods: A cross-sectional descriptive-analytic design was employed, involving a purposive sample of 100 patients with cancer experiencing side effects from chemotherapy. A predesigned questionnaire evaluated the history of chemotherapy and its side effects, Psychological, social, and religious needs, and Level of independence in basic self-care and daily living skills. Descriptive and inferential statistics organized, tallied, and examined the gathered data.
Results: The majority 88 percent of clients meet their needs moderately adequate, only 9 percent of clients meet their needs adequately and 3 percent of clients cannot meet their needs. The overall mean score was 20.99 (SD = 4.802) out of a maximum possible score of 24, indicating that most patients demonstrated autonomy in self-care effectiveness concerning daily activities. A significant correlation was observed between the levels of independence and the demographic variables of the patients. Additionally, there is a noteworthy positive correlation (r = 0.303) between mental health, social, and spiritual requirements and the degree of independence in essential self-care efficacy among cancer patients.
Conclusion: The health team's primary duty is to raise awareness of and provide an explanation of self-care management of the disease. This will help people adopt a positive mindset and teach them how to practice at standard levels.
Keywords: Self-care efficacy; Cancer; Chemotherapy; Side effects; Patient needs
Introduction![]()
Cancer poses a significant health challenge globally, ranking as a significant cause of worldwide fatalities. Data from 2018 indicate that there are approximately 18 million new cancer diagnoses each year, resulting in 9.6 million deaths attributed to the disease [1].
Chemotherapy serves as a systematic approach to cancer management through the use of anticancer drugs, which inhibit the rapid growth and division of cancer cells. Unfortunately, this treatment does not differentiate between malignant and normal cells, leading to adverse effects when healthy cells are harmed [2]. Self-care encompasses individuals’ actions to maintain their physical and mental health, prevent illness, and support recovery after illness or hospitalization [3]. It involves personal decisions and activities to address health concerns or enhance well-being [4].
For cancer patients on chemotherapy, adapting personal care practices to meet their physiological and emotional needs post-therapy is crucial. Thus, nurses play a pivotal in recognizing the extent and nature of self-care deficits among cancer patients, providing them with the necessary knowledge, expertise, and assistance to effectively manage their condition [5].
Malignant disease remains a prevalent health issue across communities worldwide and is a leading contributor to illness and mortality. According to GLOBOCAN (2012), there were 8.2 million deaths related to cancer and 14.1 million new diagnoses reported. This is expected to climb by at least 70% by 2030. In India [6], there are expected to be 14.5 lakh new instances of cancer and 7.36 lakh deaths from the disease, according to a study published in May 2016 by the Indian Council of Medical Study. Nevertheless, only 12.5% of patients receive treatment at hospitals when their illness is still in its early stages [7]. Estimates from the GLOBOCAN 2012 Cancer Report [8] show that The five most prevalent cancers in India, impacting both genders, were lung (6.9%), colorectal (6.3%), prostate (9.9%), cervical (12.1%), breast (14.3%), and colon (9.9%). These cancers account for 302,124 fatalities [9]. Cancer patients face a wide range of symptoms. The inability to handle symptoms well might make it difficult for a person to do daily responsibilities. It is anticipated that the overall cancer burden in Chennai will increase by 32% between 2002 and 2006; changes in cancer risk will account for 19% of this increase, while demographic changes will account for the remaining 13%. In Chennai, approximately 6,100 new cancer cases are diagnosed each year, contributing to a total of around 55,000 new cases across Tamil Nadu. To address the projected rise in the cancer burden in the state, it is essential to implement a comprehensive strategy aimed at evaluating and improving the cancer management and care infrastructure, as well as ensuring sufficient budget allocations [10]. Chemotherapy medications primarily attack tumor cells through a mechanism called genotoxicity, which involves the generation of reactive oxygen radicals. This mechanism inflicts damage on both cancerous and healthy cells, rather than exclusively targeting cancer cells [11].
One of the most important areas of the pharmaceutical industry is the development of novel anti-cancer drugs, as chemotherapy is a vital component of the treatment of many diseases [12]. However, the intrinsic properties of chemotherapy cause injury not only to healthy cells but also to cancer cells, leading to unfavourable outcomes [13]. A person’s emotional condition, quality of life, and physical health are all impacted by the adverse effects of chemotherapy [14,15]. Common temporary adverse effects associated with Conventional adjuvant chemotherapy protocols include oral mucositis, neutropenia, fatigue, nausea, and vomiting, listed here in order of their frequency and severity. This is one of the more common adverse effects of cancer chemotherapeutic management that has been identified in recent years [16-21].
Chemotherapy has several adverse effects on cancer patients, some of which can worsen and make it impossible for patients to lead regular lives. Increased symptom burden will significantly affect the patient's degree of psychological distress and quality of life. Numerous affordable and effective self-care strategies are available to alleviate these side effects. When provided to patients, these techniques can empower them to manage the adverse effects of chemotherapy successfully and maintain a fulfilling, healthy lifestyle. This study aims to Self-managing cancer patients experiencing side effects following chemotherapy.
Methods![]()
Research Design
A descriptive-analytic cross-sectional study was conducted at PSG Hospital, Oncology Unit, Coimbatore, Tamil Nadu.
Research Participants
Cancer patients receiving chemotherapy treatment between the ages of 20 and 60 years and experiencing side effects from the treatment were selected for the study. Patients who had undergone radiation therapy were excluded. A purposive non-random sampling method was applied. The sample size for this study was calculated using Cochran's formula, based on data from a prior study conducted by Nandakumar A in New Delhi. While the calculated sample size was n=118, the study included 100 participants.
Research Instrument
The research instrument was a structured questionnaire consisting of five parts:
- Part I: Captured sociodemographic details, including age, sex, marital status, education, occupation, monthly income, level of family support, and patient availability.
- Part II: Comprised seven questions assessing patients' understanding of cancer, its causes, chemotherapy administration, adverse effects, and when to seek medical attention.
- Part III: Included seven questions about chemotherapy and its side effects.
-
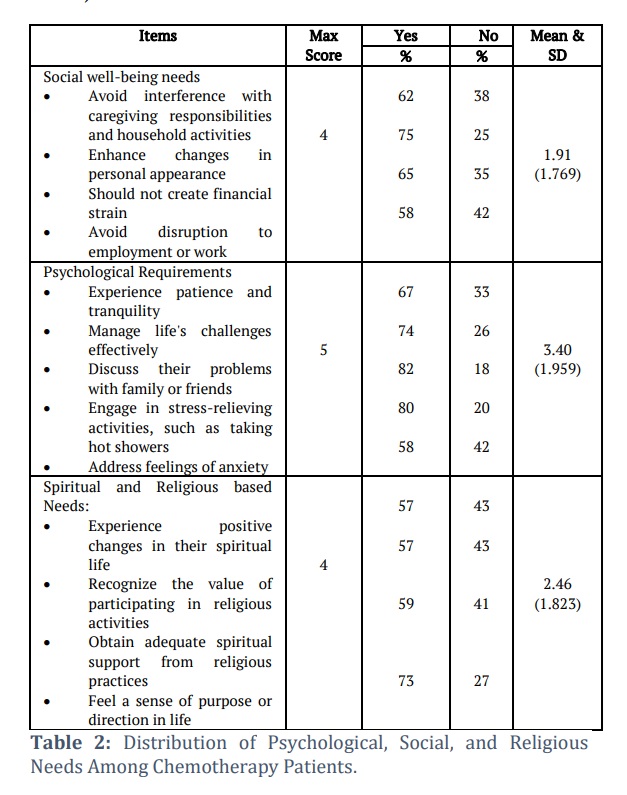
Part IV: Evaluated patient needs in psychological, social, and religious domains through 13 questions. The total score was categorized as:
- Adequate (11–13),
- Moderately Adequate (4–10),
- Inadequate (0–3).
-
Part V: Assessed patients' independence in basic self-care and daily living efficacy using 12 items. Scores were classified as:
- Completely Dependent (0–4),
- Need Assistance (5–19),
- Independent (20–24).
Ethical Consideration
The study obtained formal approval from the Institutional Human Ethics Committee of the PSG Institute of Medical Sciences and Research, authorized by the Dean of PSG Hospital. Informed consent was acquired from all participants before inclusion. The ethics committee's decision was issued on April 14, 2023, with reference number PSG/IHEC/2023/Appr/Exp/157.
Data Collection Procedure
After ethical approval, each patient was informed about the study's purpose. Cancer patients undergoing chemotherapy were selected based on the inclusion criteria. The questionnaire was then administered, and data were collected within 20 minutes per participant.
Statistical Analysis
Data were entered into SPSS and analyzed using descriptive and inferential statistics. Descriptive statistics included frequency, mean, standard deviation, and mean percentage. Chi-square tests and correlation coefficients were applied for inferential analysis.
Results![]()
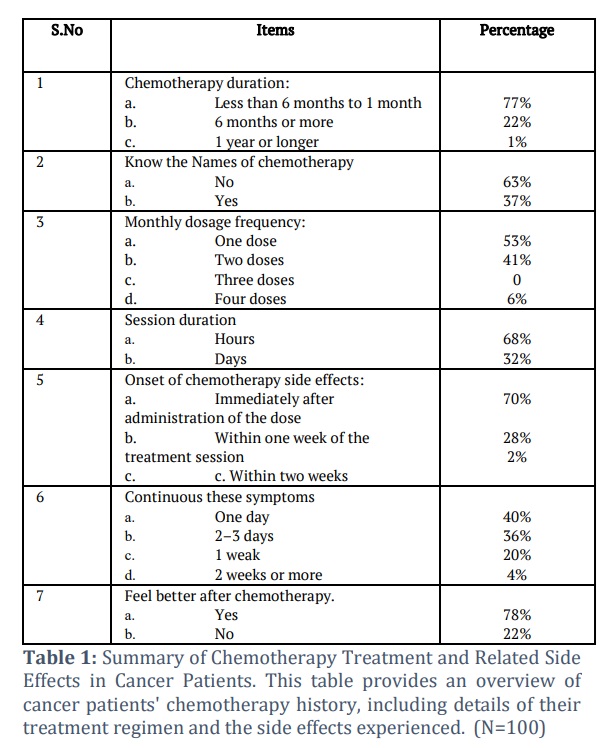
The largest group of individuals (50%) fell within the age range of 51 to 60 years. The majority (66%) of them were female. 86 percent of clients were married and completed their primary education (39%). 31 percent of clients were illiterate and the majority (69%) of clients were working still. Maximum (65%) of clients were in the monthly income range of Rs. 10,000 to Rs. 15,000. Three-fourths of the (76%) clients’ treatment was supported by Government health insurance. Nearly half (58%) of them were depending on their son/daughter to lead a life. 77 percent of clients were under chemotherapy for less than 6 months. More than 70 percent of clients were affected by the side effects from a week after the chemotherapy and felt better from the disease progress after the chemotherapy (78%). Only a small percentage (30%) of clients expressed chemotherapy side effects which lasted for a week.
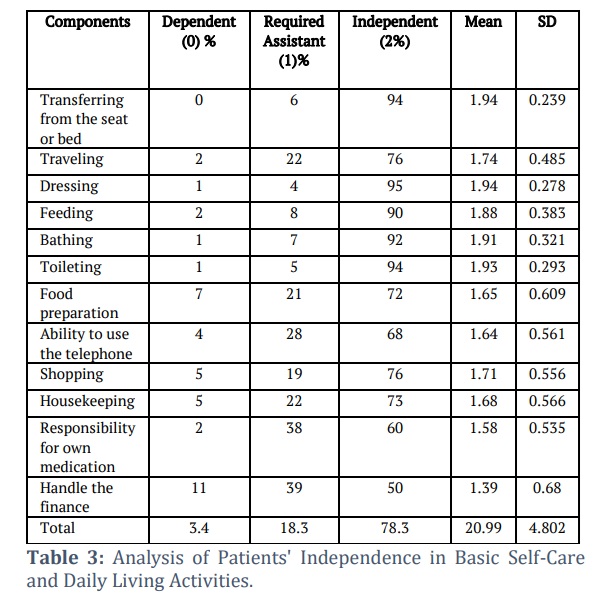
Distribution of clients based on history and side effects of chemotherapy shows that 77 percent of clients started chemotherapy less than 6 months history and 63 percent of clients know their chemotherapy name. 70 percent of clients were affected with the side effects within a few days of chemotherapy and it lasted for more than a week for 24 percent of clients. 78 percent of clients felt better from the disease progress after the chemotherapy (Table 1). The analysis of patients' independence in basic self-care and daily living activities reveals that the majority exhibit high levels of independence across various domains. For transferring from a seat or bed, 94% were independent, with significant influences observed from factors such as age (χ² = 64.26, p = .031), financial support (χ² = 148.69, p = .000), and adequacy of income for treatment (χ² = 96.46, p = .002). In contrast, other variables like marital status and education showed no significant impact. For activities like traveling, dressing, feeding, bathing, toileting, and food preparation, over 70% of patients were independent, and specific activities like responsibility for own medication and handling finances showed lower levels of independence, with 60% and 50% managing independently, respectively. Across all activities, the overall distribution highlights that 3.4% of patients were completely dependent, 18.3% required assistance, and 78.3% were fully independent, with an overall mean independence score of 20.99 (SD = 4.802).
Hence it reveals that patients show high levels of independence in basic self-care and daily living activities, with significant factors like age, financial support, and adequacy of income influencing their independence in certain areas, especially transferring and handling finances. However, other variables like occupation and marital status had less impact across most activities (Table 3).
Evaluation of the correlation coefficient according to Karl Pearson between the psychological, social, and spiritual needs and degree of independence in fundamental self-care abilities for daily living on cancer shows a significant positive relationship (r= 0.303).
Figures & Tables
Cancer and its management represent a significant and fatal challenge. Chemotherapy is a crucial treatment option for cancer patients; however, it comes with numerous adverse effects and serious issues that impact the biological, mental, social, and spiritual dimensions of personal life, often affecting their normal functioning for months or even years. As a result, Individuals receiving chemotherapy treatment require comprehensive information regarding their treatment plans, including possible adverse reactions, self-care strategies, and the impact on job and personal connections, all of which are vital for effective intervention outcomes [22].
The outcomes of this research reveal that nearly half of the participants fall within the 51–60 age range, suggesting that cancer is more prevalent among older individuals. Additionally, over three-quarters of these patients were female. This aligns with findings from a study of Asian Americans [23], which noted a mean age range of 21 to 86 years, with a predominance of females. This observation is further supported by research conducted by Jung et al., which highlights that cancer is predominantly a pathological condition affecting older adults, with incidence rates escalating significantly after the age of 50 and hitting its highest levels in the oldest demographics for many cancer types [24].
Most patients were still employed, a finding that contrasts with Couzin-Frankel's report, which indicated that most cancer patients are either not employed or jobless [25]. Additionally, our research indicated that roughly one-third of the patients were illiterate. Despite this, most participants recognized their diagnosis, echoing the results of Üstündağ and Zencirci, who found that just ten percent of cancer patients in their study were illiterate [26].
Our research also revealed that chemotherapy-related adverse effects generally emerge soon after administration, within a few days to a week. This finding partially aligns with Wilkes and Barton-Burke's observations, which suggested that side effects from chemotherapeutic agents can emerge anywhere from a few days to several weeks post-treatment [27]. The timing of these side effects may vary depending on their physiological nature, with some appearing sooner than others.
Conversely, regarding patient satisfaction after chemotherapy, two-thirds of those studied reported feeling better. This is in agreement with Adenipekun and Soyannwo's findings, which indicated that the majority of their participants successfully handled the reactions to chemotherapy and reported satisfaction with the care provided [28].
In our research, we discovered that over fifty percent of clients had an overall low extent of understanding. This may be attributed to the generally limited educational attainment of the participants or the absence of ongoing educational programs aimed at increasing patient awareness. Similar findings were reported by Aziz, who noted a low overall knowledge level among patients regarding their illness and treatment, with significant differences in patients' knowledge levels [29].
The analysis of biological conditions among the participants in this study revealed that the most prevalent issue was related to the gastrointestinal tract, which included loss of appetite, nausea, vomiting, and alterations in taste. This finding aligns with the report from the American Cancer Association, which stated that antineoplastic agents can provocate the stomach coating and the duodenum, stimulating nerves that communicate with the emesis center in the brain, leading to feeling sick and expulsion of stomach contents [30].
Additionally, our study revealed that most patients experienced severe tiredness and overall weakness, which impacted their everyday activities. This observation is consistent with Mahoney et al., who noted musculoskeletal changes in patients being treated with chemotherapy [31].
Supporting this finding, Piamjariyakul et al. emphasized the importance of assisting cancer patients in managing the adverse reactions of chemotherapy and equipping them with training and resources about their care [32]. At the same time, the studied patients were mostly self-sufficient in essential daily activities like walking, dressing, eating, and toileting, over half required assistance with bathing, and a quarter needed help with food preparation and housekeeping tasks.
This finding aligns with the study undertaken by Alptekin et al., which indicated that the majority of caregivers resided in the same household as the patient and confirmed that patients required assistance with one or more essential daily tasks [33]. This requirement for support could be due to the participants in the study having an average age of 48 years. As is well-known, the body’s functional performance tends to decline with age, resulting in diminished self-care capabilities that can impact patients' levels of independence and increase their need for help in effectively managing daily tasks.
Most cancer patients reported low levels of Physical, emotional, and social wellness. This may stem from limited knowledge regarding the complications from chemotherapy and their intervention, as well as diminished interaction with healthcare providers—patients often spend minimal time in the outpatient clinic due to high caseloads. This observation is supported by Janelsins et al., who proposed that intellectual challenges in cancer-affected patients undergoing chemotherapy result from the impact of therapy on their demands. Consequently, the contributors emphasize the crucial nursing contribution to our study, particularly in addressing and enhancing the biological, psychosocial, and religious needs of patients who are administered cancer therapy [34].
With the connection between patients' overall knowledge level and their sociodemographic information, this study found statistically significant associations between patients' mental health, social, and religious necessities, their level of independence, and various demographic variables. However, factors such as sex, education, occupation, monthly income, marital status, and financial treatment support did not show significant relationships. This finding aligns with Aziz’s research, which indicated statistically significant relationships between age and sex and overall insight into the disease and its treatment strategies [29]. Additionally, a strong correlation existed between education attainment and cumulative knowledge scores.
Conversely, Kandasamy, Chaturvedi, and others recommended that spiritual fulfilment is a vital aspect of wellness enhancement and resilience for cancer patients, closely linked to the bodily and emotional indicators of discomfort. They emphasized the importance of addressing this component appropriately in palliative care settings [35].
Patient instruction and guidance can significantly alleviate stress, enhance adaptive skills, and improve overall health, particularly for those with metastatic conditions. However, challenges such as limited health literacy, nonadherence, and lack of compliance present constraints to effective patient education [35].
The primary role of the healthcare team is to raise awareness and provide guidance on self-management strategies for diseases, fostering a positive attitude and encouraging adherence to established standards. To promote wellness and sustain both physiological and emotional well-being, individuals along with their families and communities, engage in self-care activities to prevent illness and support recovery after a hospital discharge. Self-care encompasses the choices and actions individuals take to address health issues or improve their overall health.
Acknowledgements
The authors would like to acknowledge the Institutional Human Ethics Committee at PSG Institute of Medical Sciences and Research for granting permission to carry out this study. They also express their appreciation to all participants for their significant contributions to the success of this research.
Author Contributions
Dr. M D Anuratha, Ph.D. – Conceptualization, study design, definition of intellectual content, literature synthesis, data gathering, data interpretation, statistical assessment, and manuscript drafting.
Dr. Santhi Muttipoll Dharmarajlu, Ph.D. – Concept development, Research design, statistical analysis, manuscript formulation, editing, and comprehensive review.
The authors affirm that there are no conflicts of interest concerning the publication of this paper.
![]() References
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians, (2018); 68(6): 394–424.
- PDQ Supportive and Palliative Care Editorial Board. Family Caregivers in Cancer: Roles and Challenges (PDQ®). (2010); National Cancer Institute, USA. https://www.ncbi.nlm.nih.gov/books/NBK65845.2/
- Williams PA. Fundamental Concepts and Skills for Nursing. (2028); Elsevier Health Sciences, London: 5th edition.
- Godfrey CM, Harrison MB, Lysaght R, Lamb M, Graham ID, et al. Care of self–care by other–care of other: the meaning of self-care from research, practice, policy, and industry perspectives. International Journal of Evidence-Based Healthcare, (2011); 9(1): 3–24.
- Smeltzer SC, Cheever KH, Bare B, Hinkle JL. Textbook of Medical-Surgical Nursing, Vol. 2. Wolters Kluwer Health, Philadelphia. (2011); PA, USA, 12th edition.
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. International Journal of Cancer, (2015); 136: E359‑86.
- Nandakumar A. Over 17 Lakh New Cancer Cases in India by 2020: ICMR. New Delhi, India: ICMR; 19 May, 2016. Available from: http://www.mid‑day.com/articles/Over 17lakhnewcancercasesinIndiaby2020‑icmr/17248152. [Last accessed on 2016 Oct 20].
- Stewart BW, Wild CP. World Cancer Report 2014. London: IARC; 2014.
- Saranath D, Khanna A. Current status of cancer burden: Global and Indian Scenario. Biomedical Research Journal, (2014); 1: 1‑5.
- Conklin KA. Chemotherapy-associated oxidative stress: impact on chemotherapeutic effectiveness. Integrative Cancer Therapies, (2004); 3(4): 294-300.
- Lee C, Longo VD. Fasting vs dietary restriction in cellular protection and cancer treatment: from model organisms to patients. Oncogene, (2011); 30(30): 3305-16.
- Chabner BA, Roberts TG Jr. Timeline: chemotherapy and the war on cancer. Nature Reviews Cancer, (2005); 5(1): 65-72.
- Liu B, Ezeogu L, Zellmer L, Yu B, Xu N, et al. Protecting the normal to better kill the cancer. Cancer Medicine, (2015); 4(9): 1394-403.
- Carelle N, Piotto E, Bellanger A, Germanaud J, Thuillier A, et al. Changing patient perceptions of the side effects of cancer chemotherapy. Cancer, (2002); 95(1): 155-63.
- Coates A, Abraham S, Kaye SB, Sowerbutts T, Frewin C, et al. On the receiving end–patient perception of the side-effects of cancer chemotherapy. European Journal of Cancer and Clinical Oncology, (1983); 19(2): 203-8.
- Broeckel JA, Jacobsen PB, Horton J, Balducci L, Lyman GH. Characteristics and correlates of fatigue after adjuvant chemotherapy for breast cancer. Journal of Clinical Oncology, (1998); 16(5): 1689-96.
- Berger AM. Patterns of fatigue and activity and rest during adjuvant breast cancer chemotherapy. Oncology Nursing Forum, (1998); 25(1): 51-62.
- Sitzia J, Huggins L. Side effects of cyclophosphamide, methotrexate, and 5-fluorouracil (CMF) chemotherapy for breast cancer. Cancer Practice, (1998); 6(1): 13-21.
- Jacobsen PB, Hann DM, Azzarello LM, Horton J, Balducci L, et al. Fatigue in women receiving adjuvant chemotherapy for breast cancer: characteristics, course, and correlates. Journal of Pain and Symptom Management, (1999); 18(4): 233-42.
- Bower JE, Ganz PA, Desmond KA, Rowland JH, Meyerowitz BE, et al. Fatigue in breast cancer survivors: occurrence, correlates, and impact on quality of life. Journal of Clinical Oncology, (2000); 18(4): 743-53.
- Jacobsen PB, Stein K. Is fatigue a long-term side effect of breast cancer treatment?. Cancer Control, (1999); 6(3): 256-63.
- Siddiqi A, Given CW, Given B, Sikorskii A. Quality of life among patients with primary, metastatic, and recurrent cancer. European Journal of Cancer Care, (2009); 18(1): 84–96.
- Im EO, Lee B, Chee W. Shielded from the real world. Cancer Nursing, (2010); 33(3): E10–E20.
- Jung KW, Won YJ, Kong HJ, Oh CM, Lee DH, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2011. Cancer Research and Treatment, (2014); 46(2): 109–123.
- Couzin-Frankel J. Dizzying Journey to a New Cancer Arsenal, American Association for the Advancement of Science, (2013); Washington, DC, USA.
- Ust¨unda˘g S, Zencirci AD. Factors affecting the quality¨ of life of cancer patients undergoing chemotherapy: a questionnaire study. Asia-Pacific Journal of Oncology Nursing, (2015); 2(1): 17.
- Wilkes G, Barton-Burke M. Oncology Nursing Drug Handbook. 2009.
- Adenipekun A, Kupoluyi T, Soyannwo O. Knowledge and experience of cancer patients receiving chemotherapy in a teaching hospital in Nigeria. Internet Journal of Pain, Symptom Control and Palliative Care, (2012); 9(1): 1–5.
- Aziz AW. Patient education: it’s the effect on the quality of life of a patient with cancer on chemotherapy. Journal of American Science, (2011); 7(8): 541-542.
- Alteri R. Breast Cancer Facts & Figures, 2013. 2014, American Cancer Society, Atlanta, (2013); GA, USA.
- Mahoney SE, Davis JM, Murphy EA, McClellan JL, Pena MM. Dietary quercetin reduces chemotherapy-induced fatigue in mice. Integrative Cancer Therapies, (2014); 13(5): 417–424.
- Piamjariyakul U, Williams PD, Prapakorn S, Kim M, Park L, et.al. Cancer therapy-related symptoms and self-care in Thailand. European Journal of Oncology Nursing, (2010); 14(5): 387–394.
- Alptekin S, G¨on¨ull¨u G, Y¨ucel I, Yarıs F. Characteristics and quality of life analysis of caregivers of cancer patients. Medical Oncology, (2010); 27(3): 607–617.
- Janelsins MC, Devine KA, Mustian K, Mohile SG. Cognitive difficulties among patients with cancer receiving chemotherapy affect the quality of life: a University of Rochester Clinical Community Oncology Program study of 439 patients. Journal of Clinical Oncology, (2011); 29(15): 9119.
- Gampenrieder SP, R. Bartsch, P. Matzneller, Pluschnig U, Dubsky P, et al. Capecitabine and vinorelbine as all-oral chemotherapy in HER2-negative locally advanced and metastatic breast cancer. Breast Care, (2010); 5(3): 158–162.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0![]()


