

Full Length Research Article
Bone marrow-derived mesenchymal stem cells: a potential therapy in an autoimmune hepatitis rat model
Nagia Sultan1, Wafaa Saadeldin Ramadhan*2, 3 Saleh Alkarim1,3
Adv. life sci., vol. 12, no. 1, pp. 105-113, February 2025
*– Corresponding Author: Wafaa Saadeldin Ramadhan (Email: wramadhan@kau.edu.sa)
Authors' Affiliations
2. Department of Clinical Anatomy, Faculty of Medicine, King Abdulaziz University Jeddah – Saudi Arabia
3. Stem Cell Research Unit, King Fahd Medical Research Center, King Abdulaziz University, Jeddah, – Saudi Arabia
[Date Received: 05/02/2024; Date Revised: 28/09/2024; Date Published: 31/12/2024]
Editorial Note on Version of Record
28 May 2025: This article has been corrected. See https://doi.org/10.62940/als.v13i0.4251 for more information.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Autoimmune hepatitis (AIH) is becoming more common worldwide. The therapy choices for AIH are still limited, with unfavorable side effects resulting in patients with a low quality of life. This study aims to study the therapeutic role of bone marrow-derived mesenchymal stem cells (MSCs) on AIH in the rat model.
Methods: Twenty-nine white Wistar rats were used for a total of 53 days. Four groups were set up; Group I (5 rats) was used as the negative control (CON). Group II (24 rats) was administered Concanavalin A (Con A) 20 mg/kg ip once a week for five consecutive weeks. Sixteen rats from group II were divided among groups III and IV after stoppage of Con A and injected with 2 x106 BM-MSCs via tail vein. Group III (TTT-12) rats were sacrificed after 12 days and Group IV (TTT-18) after 18 days. Morphological, biochemical, histopathological, and immunohistochemical studies were conducted.
Results: The administration of BM-MSCs lowered elevated serum levels of AST by 47% after 12 days and 19% after 18 days whereas the level of ALT decreased by 13% and 20.8%in group Con A. Serum inflammatory cytokines IL-10 and tumor necrosis factor alpha (TNF-α) increased in the Con A group were decreased in treated groups by 27% and 23% in TTT-12 and 22.8% and 1.8% in TTT-18. In group TTT-12, the area of Kupffer cells immunostained with CD68 was significantly reduced by 72%, whereas the BM-MSCs immunostained with CD44 were more intense by increasing by 257%. The therapeutic effect of BM-MSCs in group TTT-12 exceeded that in TTT-18 decreasing liver enzymes, inflammation and fibrosis, and restoring liver structure.
Conclusions: BM-MSCs achieved a considerable short-term improvement in the AIH model; however, repeated injections were necessary to achieve a sustained therapeutic effect.
Keywords: Liver; Autoimmunity; MSCs; Inflammatory cytokines; CD68; CD44; Histopathology
Introduction![]()
Autoimmune hepatitis (AIH) is a sustained inflammatory disease among various age groups worldwide. Although autoimmunity diseases are infrequent, it is increasingly identified globally [1]. AIH incident rate strikingly increased in the period (2014-2016), relative to the preceding years (2008-2010) [2]. AIH has a wide clinical spectrum, ranging from symptom -free presentation [3] to an acute severe disease [4]. The progression of AIH can pass unnoticed and consequently untreated resulting in chronic hepatitis in 70%-80% of the cases and 33% with cirrhosis by the time it is recognized [5, 6] Portal hypertension, liver failure, and hepatocellular carcinoma are common consequences of cirrhosis of the liver [7]. The underlying causes of AIH are still obscure; however, environmental factors, epigenetic changes, and gut microbiome have been correlated with its development [8].
In genetically predisposed individuals, AIH is mostly triggered by infections [9]. Viral infections reveal a process of molecular pathogenesis simulation. This occurs when the immune response is directed towards self-antigens rather than the real pathogen due to structure similarity initiating AIH. Proteins of the hepatitis C virus have shared amino acid sequences with autoantigen CYP2D6 resulting in AIH-2 [10,11]. AIH typically exhibits pathological picture of fierce hepatitis, evident by the presence of lymphocytes, macrophages, and plasma cells [12]. AIH is essentially known as a T-cell-driven disorder, with B-cell activation dependent on T-cell involvement [13]. Immunosuppressive drugs are the common therapeutic measure for AIH. Still, liver cell failure results when patients do not respond to such drugs [14].
The marked side effects accompanied with the corticosteroids therapy can be accompanied by impaired quality of life [15]. Clinically, the complications developing from AIH often hinder its improvement, increasing the mortality rate [16].The global spread of AIH focuses attention on the prompt need for new therapeutic strategies [17]. Recent research revealed significant advancements in stem cell therapy [18]. MSCs, pluripotent stem cells, can migrate to injured areas and apply their therapeutic effect [19]. The source of MSCs markedly affects its potential role in differentiation and proliferation [20]. This was related to the various microenvironments in which the MSCs are present [21]. The sources of MSCs have been previously documented to include bone marrow, fetal membranes such as placenta, umbilical cord, and amnion [22], as well as adipose tissue [23]. Clinically, the bone marrow-derived MSCs are the most considered [24]. MSC-based therapy is becoming a prominent measure in treating a wide range of liver pathology due to its capabilities in immunomodulation, anti-fibrotic effects, and differentiation into hepatocyte [25]. Not long past, the therapeutic advantages of MSCs were investigated clinically in cases of stroke, multi-system atrophy, multiple sclerosis, Parkinson’s disease, Alzheimer’s disease, chronic spinal cord injury, and cardiovascular disease [26]. It is established that preclinical studies in animal models proved successful, especially when studying the development of new therapeutic measures. The AIH animal model proved a good simulation for the pathology of AIH in humans [27]. Administration of Concanavalin A (Con A) to animals induced liver injury associated with a marked increase of interleukin 2 (IL-2), IL-4, and interferon-gamma (IFN-γ) preceded with T helper cells activation [28].
Hence the present work aimed to assess the early and late therapeutic role of BM-MSCs in AIH rat model induced by Con A.
Methods![]()
Drug and chemicals
Concanavalin A (ConA) was purchased from (Nanjing duly biotech Co. Ltd (Xinjiang, China). CD44 antibody was obtained from (Solarbio Science & Technology Co., Ltd., Beijing, China). Dulbecco & 39;s modified eagle medium low glucose (DMEM-LG), with 10% fetal calf serum,1%glutamine (Gibco, USA) and 1% penicillin/streptomycin (Sigma-Aldrich, USA ).
Animals
29 male Wister albino rats 10-12 weeks old, weighing 192-215g, were obtained from the animal house in the Faculty of Pharmacy, Jeddah, Saudi Arabia. 5 male mice 8-10 weeks, weighing 25-27g, were used for isolation of MSCs. All animals were housed in plastic cages following guidelines of the National Institutes of Health for the care and use of Laboratory animals (NIH Publications No. 8023, revised 1978). Their environment was pathogen-free, maintained at a constant temperature of 22 °C, and on a 12:12 h light–dark cycle. Rats were provided with unrestricted standard food and water. All experimental procedures were performed according to the animal ethical regulation of the Faculty of Pharmacy and approved by the Ethics Committee (No “PH-1443-19”), following the NIH guidelines.
Experimental plan
Rats were randomly organized into four distinct groups:
– Group I (CON): (N= Five) served as negative control. Animals were given physiological saline at the same dose of Con A ip for the same period.
– Group II (Con A): (N= Twenty four) served as an AIH model. Rats were administered with Con A (20 mg/kg) ip once every seven days for five successive weeks [29, 30]. Sixteen rats from group Con A were separated and equally divided into the following groups for treatment.
– Group III (TTT-12): Consisted of 8 rats that received Con A in group II. After Con A was discontinued, 0.2 ml of DMEM solution containing BM-MSCs 2 x106 was injected into the rat tail vein. Animals in this group were sacrificed 12 days after the administration of BM-MSCs [31, 32, 33].
– Group IV (TTT-18): Eight rats from group II, received Con A, were administered BM-MSCs suspension (2 x106 in 0.2 ml of DMEM) via the same route after the stoppage of Con A. Animals in this group were sacrificed 18 days after the administration of BM-MSCs [34].
The injection into the rat tail vein was done using a 26-gauge Kovax syringe (Koreavaccine, Gyeonggi,
Isolation and expansion of MSCs
Five male SWR/J mice, 8-10 weeks old, were used to extract MSCs from bone marrow following a previous established protocol [35]. After sacrification by cervical dislocation, femurs and tibiae were extracted, cleaned and tip removed before centrifugation at 10,000 x g for 15s. The bone marrow cells were filtered through a 70-mm nylon mesh filter (BD,Falcon, USA). Cells were harvested into a 6-well plastic culture plate with (DMEM-LG), 10% fetal calf serum, 1%glutamine, and 1% penicillin/streptomycin. Trypsinization was done, after the primary culture reached 90% confluence. The collected cells were cultured and the medium refreshed every three days. The cells from the third passage were used after checking their viability and counting them using a hemocytometer. [36]. The cells became attached, long, spindle shaped with thin cell body as typically described previously [37].
Biochemical analysis
Blood was drawn from the retro-orbital plexus of veins under light ether anaesthesia, 24 hours after the last Con A dosage, and at the time of sacrifice [38]. The serum was separated by centrifugation at 1300 rpm for 10 minutes. Serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels were measured both before and after MSC transplantation [39]. Tumor Necrosis Factor Alpha (TNF-α) levels and Interleukin 10 (IL-10) were measured using an ELISA kit. (My BioSource, San Diego, California, USA).
ELISA testing was performed using a DSX system (Dynex Technologies-Technogenetics-Germany) in accordance with the manufacturer’s instructions.
Histological and immunohistochemical analyses
Histopathological Study
The rats were anesthetized by sodium pentobarbital diluted in saline (80 mg/kg /ip) [40] followed by cervical dislocation. The abdomen was dissected, and the livers were removed, washed and fixed in10% buffered formalin, dehydrated in graded alcohol and embedded in paraffin. Sections 4-μm thick were cut and processed for staining with hematoxylin and eosin to assess the general structure of the liver and Masson’s trichrome stain to evaluate liver collagen [41]. Sections were examined under light microscope (Olympus BX51TF) and photographed by camera DP72 color.
Immunohistochemical Study
4-μm-thick cut sections from previously prepared paraffin blocks were deparaffinized, rehydrated, subjected to antigen retrieval in a microwave and had endogenous peroxidase blocked with 3% hydrogen peroxide. The slides were treated with CD44 and CD68 antibodies (Solarbio Science & Technology Co., Ltd.) (Beijing, China), at 4°C overnight. The horseradish peroxidase/Fab polymer conjugate was used after a wash with PBS. Diaminobenzidine 1:20 dilution; Zymed Laboratories was utilized for cell identification [42].
Image analysis
Immunohistochemically and Masson’s trichrome stained slides were examined and photographed. Five non overlapping images for each slide were examined and analyzed for area percent of cells immunohistochemically stained with CD44 and CD68, or blue colored stained collagen in Masson’s trichrome- stained slides using image Pro software, version 7.
Statistical analysis
The sample size was calculated following the equation
E = (number of animals in each group × number of groups) − number of groups. The sample size was then corrected following the equation:
Corrected sample size = Sample size/ (1− [% attrition/100]) [43].
In this experiment, the attrition percent was 20%. Statistical analyses were carried out using SPSS (version: 20). The mean ± SD was employed to represent the results. The comparison between groups was illustrated using the One-way ANOVA. In all analyses, statistical significance was stated at p ≤ 0.05.
Results![]()
Morphological results
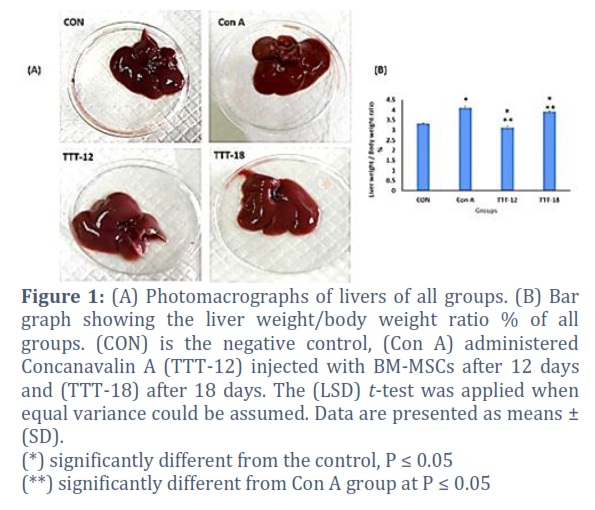
The general condition of rats was traced. Rats of the AIH group did not show any abnormal behavior or alteration in the amount of food and water consumed, yet on dissection, bleeding on the surface of the liver was detected in 2 rats. The administration of Con A did not precipitate any mortality among the rats. Three out of the 16 rats administered BM-MSCs had diarrhea for 10 days, but no mortality cases were encountered. The gross morphology of the livers of the four groups did not show any difference. However, the ratio of liver weight to body weight % of rats revealed a significant difference. As the liver weight in the Con A group increased, the resulting ratio also increased compared to other groups.
Following the administration of MCSs in groups TTT-12 and TTT-18, the relative liver-to-body weight was decreased compared to that of the Con A group due to a decrease in liver weight (Figure 1 A& B). This may be attributed to the marked congestion accompanying the inflammatory process in the livers of the Con A group, which decreased during treatment with MCSs.
Biochemical results
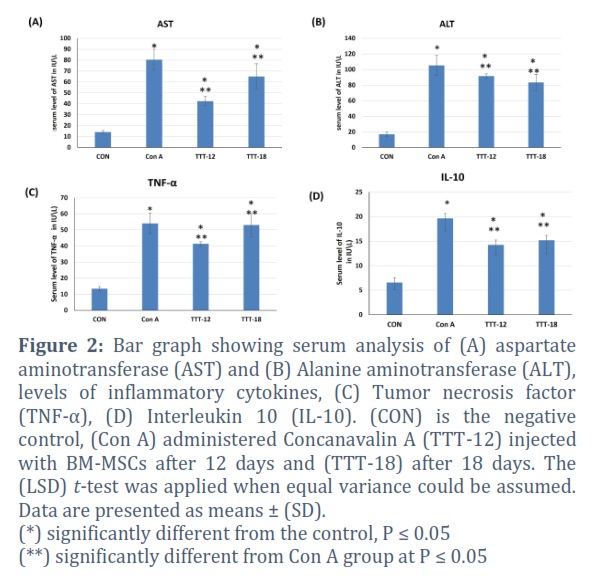
The liver function tests revealed a marked increase of AST and ALT (triple upper limit of normal) in the sera of the AIH model group (CON A). Groups III and IV treated with MSCs revealed a significant decrease in the liver AST and ALT compared to group II; AST dropped by 47% after 12 days and 19% after 18 days. ALT decreased by 13% in group (TTT-12) and 20.8% (TTT-18) (Figure 2 A& B). There was a significant increase of serum inflammatory cytokine (TNF-alpha) in rats of group CON A, but administration of BM-MSC decreased level by 23% in Group III and by 1.8% in Group IV.
Similarly, the sera level of Interleukin-10 (IL-10) revealed marked increase in the AIH model compared to treated rats in groups III and IV. The decrease in IL-10 levels was 26.3% and 22.8% in rats of groups III and IV, respectively (Figure 2 C& D).
Histological study
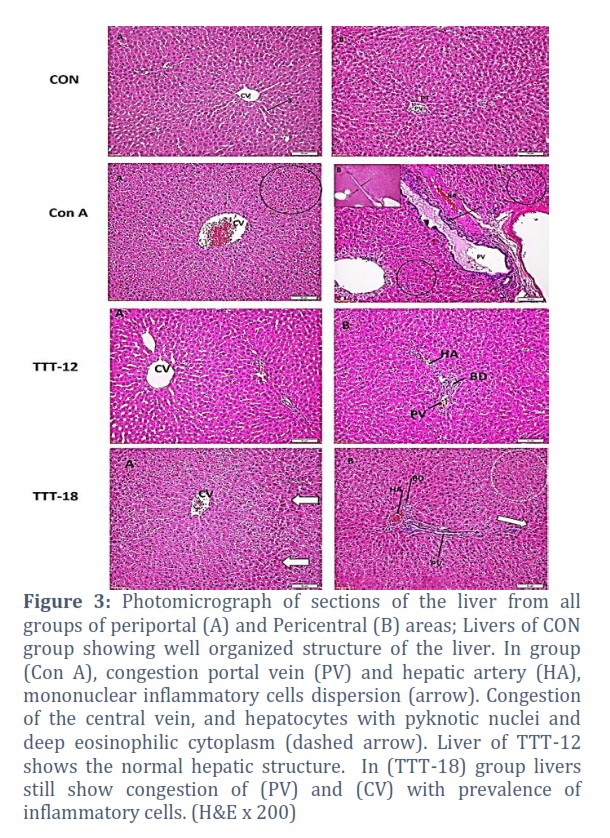
Liver sections stained with H&E revealed normal structured framework of pericentral and periportal areas of livers of the CON group. In (Con A) group, the livers manifested a distorted structure with apoptotic hepatocytes having deep eosinophilic cytoplasm and pyknotic nuclei around a congested central vein. In the periportal area, the mononuclear inflammatory cells embraced the congested portal vein and hepatic arteries. Numerous hepatocytes had pyknotic nuclei.
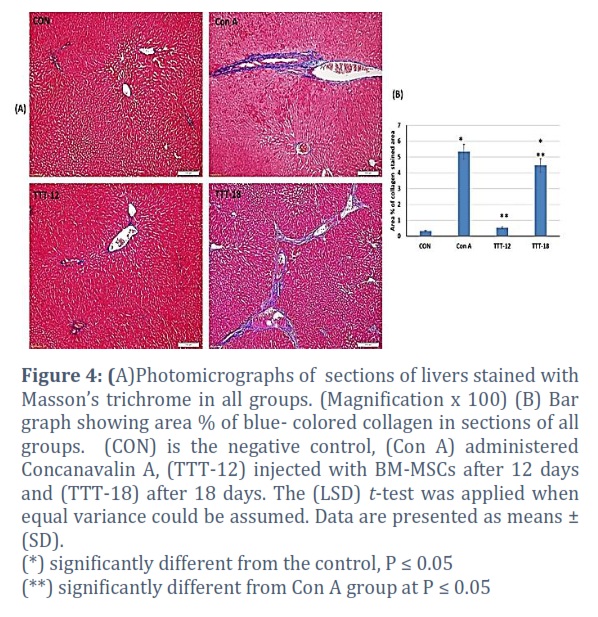
In animals administered BM-MSCs, the livers of group (TTT-12) showed repaired hepatic structure with minimal pericentral and periportal mononuclear inflammatory cell infiltration. In group (TTT-18), the pericentral area showed a congested central vein and hepatocytes with profoundly eosinophilic cytoplasm and pyknotic nuclei. Persistent pathological hepatic changes were still evident with the portal tract showing distorted structure and congested hepatic artery. Masson’s trichrome -stained liver sections of the (Con A) group showed profound fibrosis in periportal field than in the pericentral zone. Livers of rats in group (TTT-12) revealed a significant decrease in the mean area per cent of Masson trichrome-stained collagen fibers as compared to AIH model (Con A) and group (TTT-18) (P ≤ 0.05). The potential therapeutic efficacy of BM-MSCs was found to be more effective when administered early rather than late. (Figure 4 A & B).
Immunohistochemistry
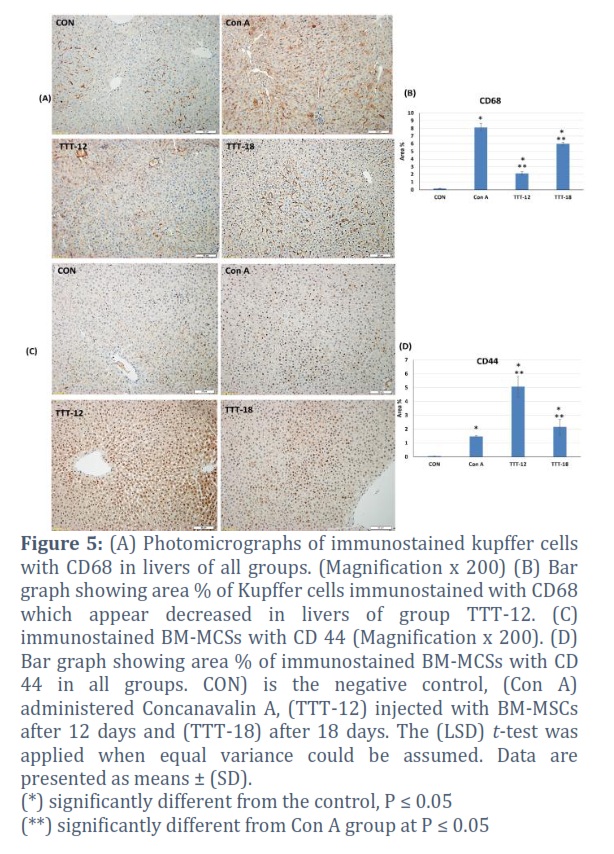
The CD68 immunostained Kupffer cells illustrated the inflammatory areas in liver sections and were quantified as area percent. Sections of the (Con A) group revealed an immense increase (8.11. ±0.48) which was markedly reduced by 73.6% in the group (TTT-12) and by 26% in the group (TTT-18) (Figure 5 A&B). The area percent of BM-MSC immunostained with CD44 was extensive in sections of livers of the group (TTT-12), which was higher by 46% than in the group (TTT-18). On the other hand, the untreated (Con A) group revealed a significant decrease compared to the groups administered BM-MSCs (Figure 5 C&D).
Figures & Tables
The liver has a distinguished immune pattern to actively avoid needless immune responses to food antigens and toxins of the alimentary tract reaching the liver [44]. However, in AIH, abundant inflammatory responses to self-antigens are not competently dominated by the liver’s tolerogenic mediators [45]. Thus, AIH is regarded as an immune-mediated inflammatory liver disease with a rising incidence and fatality rate [46].
In the present study, Con A was adopted to induce immune-mediated hepatitis in a rat model of liver injury due to its similarity to AIH in humans [47].
The challenges in managing AIH are significant. Corticosteroids are the primary choice in treating AIH, and in cases of remission, which occurs in 80% of patients, immunosuppressive therapy is added [48]. Hazards of immunosuppressive drugs include increased risk for some malignancies. Moreover, predominant infections are revealed both early after transplantation (bacterial and fungal) or later as viral fulminating in the long term [49].
The present study aimed to evaluate the therapeutic effect of bone marrow-derived MSCs in cases of AIH. MSCs were selected because they can be sorted from various types of tissues, including tonsils, amniotic fluid, and placenta [50, 51]. From a therapeutic standpoint, the preference for MSCs over other types of stem cells, such as embryonic and induced pluripotent stem cells, is due to their therapeutic privileges. MSCs modulate immune function, move to the injured site, withstand immunological reactivity, and have no ethical violations [52]. In the present work, MSCs derived from mice bone marrow were administered into the AIH rat model. Other researchers have recorded this interspecies transfer of cells previously [53]. The authors successfully transplanted islet cells from mice pancreas into rats genetically deficient in the pancreas. This was followed by the isolation of islets from rat pancreas, which initially developed from mice, and their transplantation into diabetic mice induced by streptozotocin. Interestingly, the blood sugar of diabetic mice was regulated. Similarly, BM-MSCs from Pcrx2K-lacZ transgenic mice were subretinally transplanted in rats to investigate if MSCs can enhance the existence of photoreceptor cells in vivo. The results revealed MSC culture-induced proliferation of photoreceptor cells [54]. MSC proved its potential therapeutic effect in other hepatic lesions. MSCs-exosomes proved to have an inhibitory effect on the Diethylnitrosamine-induced HCC rat model [55]. In a clinical trial, autologous MSC proved an effective short-term therapy for hepatitis B virus-induced liver failure [56]. Moreover, BM-MSC enhanced liver regeneration in alcoholic liver disease mainly by interfering with the inflammatory response [57].
In the present study, there were no mortality cases among rats of all groups. Actually, the detailed amount of food and water intake was not measured, as the focus was not on the metabolic activity of the rats, and the general condition was stable. This could also explain why the morphologic changes of livers in the present study revealed that the relative liver weight to body weight was consistent with previous findings, showing a significant increase in the Con A group [58]. The present results revealed a marked increase in the levels of ALT and AST of the Con A group compared to the control group. This was in agreement with the previous results [59]. Similarly, administration of MSCs in patients diagnosed with alcoholic hepatitis restored levels of ALT and AST to normal [60]. Administration of MSCs dramatically improved overall liver function. The results exhibited a significant decrease in AST and ALT on the 12th and 18th days, exhibiting therapeutic efficacy on MSCs.
Moreover, the deformed histological structure of livers of the Con A group elucidates a fall in liver function. These results are in line with earlier research [61, 62]. In rats of the Con A group, the marked congestion of portal and central veins with infiltration of mononuclear inflammatory cells was alleviated by the administration of BM-MSCs. The improvement of liver structure after 18 days was less evident than in the 12-day treatment group. Other researchers observed liver fibrosis was alleviated after MSCs treatment in rats and humans. They claimed that MSCs inactivated stellate cells for 14 days after the transplantation [63]. The process by which Con A-induced liver damage was induced by the activated Kupffer cells to secrete a variety of proinflammatory cytokines and induced liver tissue inflammation were critical factors in developing Con A liver injury [64]. The area percent of the hepatic Kupffer cells immunostained with CD68 in the livers of the Con A group was significantly higher than in the CON group. However, following BM-MSCs administration, a significant reduction of 73.6% after 12 days (TTT-12) and 26% after 18 days (TTT-18) was documented, demonstrating an anti-inflammatory effect of the MSCs therapy. Moreover, the inflamed intrahepatic microenvironment is fortified with proinflammatory cytokines, such as IL-6, IL-12, IFNγ, and TNFα [65]. They play a significant role in immune cells’ mobilization, differentiation, existence, and proliferation. The subjection to proinflammatory signals leads to a decrease in the effectiveness of regulatory T cells (Treg) or resistance of T effector cells to Treg cell suppression [66]. Such findings explain the increase in IL-10 and TNF-α in the rats of the Con A group in the present study. Previous research confirms that serum TNF-α and IL-10 are major factors in initiating and establishing AIH [65,67].
The present results revealed the diminution of sera IL-10 and TNF-α in Con A under the effect of MSC. This could be verified by the immune regulation exerted by the MSCs in the liver, which was found to be via cell-cell interaction or secretion of anti-inflammatory elements. They also decrease the proinflammatory cytokines by hindering the activation of the natural killer cells [68, 69]. The active substances secreted by MSCs have angiogenic and antiapoptotic properties that ameliorate the injury of tissues at the affected sites and restore blood supply [70]. The mechanisms by which MSCs participate in liver regeneration were attributed to enhancing liver cell recovery by secreting cytokines, sustaining the stellate cell function, and inducing the proliferation of the primary liver stem cells [68].
The segregated BM-MSCs successfully expressed recognized MSCs surface markers, CD44, consistent with a prior study [70]. In group TTT-12, the BM-MSCs immunostained with CD 44 area was more intense than in group TTT-18. Previous research claimed that MSCs have low engraftment due to their short life [71]. MSCs have been characterized before by positive cell surface markers, CD90, CD105, CD44, CD73, CD166, and CD140b, and being negative to CD45, CD34, CD31, and the macrophage marker CD11b as there are no standard phenotypic markers to cover the MSC [70]. The delivery method is vital to MSC transplantation and its therapeutic effect. A successful delivery method will achieve safe arrival at the intended damaged area and high regenerative power with minor ill undesirable effects. The most convenient mode of MSC transplantation is the intravenous route. This route has proved the efficient distribution of MSCs, mainly in various body organs [72]. Previous experiments have proved the accumulation of MSC in injured organs such as myocardial infarction and injured lung tissue [73, 74]. This migration was described as the active phase following the passive phase in which MSC resided in the lung first, a phenomenon described as homing [75]. It is assumed that the injured liver may produce cytokines to enroll BM-MSCs in the affected areas [76]. This explains the migration of MSCs from the injection site to distant regions of injury. In the present study, the area percent of CD44 immunostained MSCs was significantly higher in sections of rats in group TTT-12 than in group TTT-18.
In the present study, although tracing of the intravenously injected BM-MSC was lacking, detailed recognition of the cells in the target organ, the liver, was achieved. Further research is also needed to elucidate the secretory function of BM-MSC in the target organ and to study the long-term efficacy of BM-MSC in vivo. The results of this study assist the therapeutic potential of BM-MSCs in AIH. Biochemical analysis and histopathological study of livers revealed that BM-MSC administration ameliorated liver function, lowered liver enzymes, decreased inflammatory process in the liver, and restored its structure. The administration of 2×106 MSCs efficiently lowered Con A-induced hepatitis after 12 days, but the effect was insignificant after18 days. This may be attributed to either the need for higher cell counts or administration of a second dose of BM-MSCs.
Author Contributions
Najiah Sultan performed the experiment, processed all staining techniques, and wrote the manuscript. Wafaa S. Ramadan performed the statistics, analyzed the figures, revised the manuscript, and followed up on publication. Saleh Alkarim contributed to the final version and supervised the whole project.
The authors declare no conflict of interest.
![]() References
References
- Grønbæk L, Vilstrup H, Jepsen P. Autoimmune hepatitis in Denmark: Incidence, prevalence, prognosis, and causes of death. A nationwide registry-based Cohort Study. Journal of Hepatology, (2014); 60(3): 612–617.
- Lamba M, Ngu J, Stedman C. Trends in Incidence of Autoimmune Liver Diseases and Increasing Incidence of Autoimmune Hepatitis. Clinical Gastroenterology and Hepatology, (2021); 19(3): 573-579.
- Vuerich M, Wang N, Kalbasi A, Graham J, Longhi MS. Dysfunctional Immune Regulation in Autoimmune Hepatitis: From Pathogenesis to Novel Therapies. Frontiers in Immunology, (2021); 12: 76436
- Kumar BG, Sethy PC, Gupta RA. Rare etiology of persistent jaundice in type 1 autoimmune hepatitis. Archive of Clinical Cases, (2021); 8(3): 37–41.
- Manns MP, Czaja AJ, Gorham JD, Krawitt EL, Mieli-Vergani G, Vergani D, et al. Diagnosis and management of autoimmune hepatitis. Hepatology, (2010); 51(6): 2193–2213.
- Czaja AJ, Freese DK. Diagnosis and treatment of autoimmune hepatitis, Hepatology, (2002); 36(2): 479–497.
- Vierling JM. Autoimmune hepatitis and overlap syndromes: Diagnosis and management, Clinical Gastroenterology and Hepatology, (2015); 13(12): 2088–2108.
- Liwinski T, Heinemann M, Schramm C. Semin The intestinal and biliary microbiome in autoimmune liver disease-current evidence and concepts. Immunopathology. (2022); 44(4): 485–507.
- Gatselis NK, Zachou K, Koukoulis GK, Dalekos GN. Autoimmune hepatitis, one disease with many faces: etiopathogenetic, clinico-laboratory and histological characteristics. World journal of gastroenterology, (2015); 21(1): 60.
- Mieli-Vergani G, Vergani D, Czaja AJ, Manns MP, Krawitt EL, et al. Montano-Loza AJ. Autoimmune hepatitis. Nature Reviews Disease Primers, (2018); 4(1): 1-21.
- Ferri S, Muratori L, Lenzi M, Granito A, Bianchi FB, Vergani D. HCV and autoimmunity. Current pharmaceutical design, (2008); 14(17): 1678-1685.
- Löhr H, Treichel U, Poralla T, Manns M, zum Büschenfelde KM, Fleischer B. Liver-infiltrating T helper cells in autoimmune chronic active hepatitis stimulate the production of autoantibodies against the human asialoglycoprotein receptor in vitro. Clinical & Experimental Immunology, (1992); 88(1): 45-9.
- Ichiki Y, Aoki CA, Bowlus CL, Shimoda S, Ishibashi H, Gershwin ME. T cell immunity in autoimmune hepatitis Autoimmunity Reviews, (2005); 4(5): 315–321.
- Galderisi U, Peluso G, Di Bernardo G. Clinical trials based on mesenchymal stromal cells are exponentially increasing: where are we in recent years? Stem cell reviews and reports, (2022); 18(1): 23-36.
- Liberal R, Diego V, Giorgina M. Update on Autoimmune Hepatitis. Journal of Clinical and Translational Hepatology, (2015); 3(1): 42–52.
- Wong LL, Fisher HF, Stocken DD, Rice S, Khanna A, Heneghan MA, et al. The Impact of Autoimmune Hepatitis and Its Treatment on Health Utility. Hepatology, (2018); 68(4): 1487–1497.
- De Luca-Johnson J, Wangensteen K J, Hanson J, Krawitt E, Wilcox R. Natural History of Patients Presenting with Autoimmune Hepatitis and Coincident Nonalcoholic Fatty Liver Disease. Digestive Diseases and Sciences, (2016); 61(9): 2710–2720.
- Zhou YK, Zhu LS, Huang HM, Cui SJ, Zhang T, et al. Stem cells from human exfoliated deciduous teeth ameliorate concanavalin A-induced autoimmune hepatitis by protecting hepatocytes from apoptosis. World Journal of Stem Cells, (2020); 12(12): 1623.
- Hoang DM, Pham PT, Bach TQ, Ngo AT, Nguyen QT, et al. Stem cell-based therapy for human diseases. Signal Transduction and Targeted Therapy; Springer Nature, (2022); 7(1):1-41.
- Yang X, Meng Y, Han Z, Ye F, Wei L, Zong C. Mesenchymal stem cell therapy for liver disease: full of chances and challenges. Cell & Bioscience, (2020); 10(10):1-8.
- Maleki M, Ghanbarvand F, Behvarz M R, Ejtemaei M, Ghadirkhomi E. Comparison of Mesenchymal Stem Cell Markers in Multiple Human Adult Stem Cells. International Journal of Stem Cells, (2014); 7(2): 118–126.
- Kolf CM, Cho E, Tuan RS. Mesenchymal stromal cells. Biology of adult mesenchymal stem cells: regulation of niche, selfrenewal, and differentiation. Arthritis Research and Therapy, (2007); 9: 1-10.
- de Souza Fernandez T, de Souza Fernandez C. Mesenchymal stem cells: biological characteristics and potential clinical applications for haematopoietic stem cell transplantation. IntechOpen, (2016) Jul 20.Transplantation. InTech eBooks, 2016; URL: https://doi.org/10.5772/63772
- Ramos LT, Sánchez-Abarca L I, Muntión S, Preciado S, Puig N, et al. MSC surface markers (CD44, CD73, and CD90) can identify human MSC-derived extracellular vesicles by conventional flow cytometry. Cell Communication and Signaling, (2016); 14(14): 1-4
- Szabo´ GV, Ko¨vesd Z, Cserepes J, Daro´czy J, Belkin M, Acsa´dy G. Peripheral blood-derived autologous stem cell therapy for the treatment of patients with late-stage peripheral artery disease-results of the short- and long-term follow-up. Cytotherapy, (2013); 15(10):1245–1252.
- Wang LT, Ting CH, Yen ML, Liu KJ, Sytwu HK, Wu KK, Yen BL. Human mesenchymal stem cells (MSCs) for treatment towards immune- and inflammation-mediated diseases: review of current clinical trias. J Biomed Sci, (2016); 23(1):76–89.
- He C, Yang Y, Zheng K, Chen Y, Liu S, et al. Mesenchymal stem cell-based treatment in autoimmune liver diseases: underlying roles, advantages and challenges. Therapeutic Advances in Chronic Disease, (2021); 12: 1-18.
- Wang HX, Liu M, Weng SY, Li JJ, Xie C, et al. Immune mechanisms of Concanavalin A model of autoimmune hepatitis. World journal of gastroenterology, (2012); 18(2): 119.
- Zhang X, Wei HX, Rui S, Wei H, Tian Z. Opposite effects of high and low doses of interleukin-2 on T cell-mediated hepatitis in mice (interleukin-2 on hepatitis). Hepatology International, (2010); 4: 641-648
- Ye, T, Wang T, Yang X, Fan X, Wen M, Shen Y, Xi X, Men R, Yang L. Comparison of Concanavalin a-Induced Murine Autoimmune Hepatitis Models. Cellular Physiology and Biochemistry, (2018); 46(3): 1241-1251.
- Louis H, Le Moine A, Quertinmont E, Peny MO, Geerts A, Goldman M, Le Moine O, Devière J. Repeated concanavalin a challenge in mice induces an interleukin 10-producing phenotype and liver fibrosis. Hepatology, (2000); 31(2): 381–390.
- Bos C, Delmas Y, Desmoulière A, Solanilla A, Hauger O, et al. In Vivo MR Imaging of Intravascularly Injected Magnetically Labeled Mesenchymal Stem Cells in Rat Kidney and Liver. Radiology, (2004); 233(3): 781–789.
- Kim M D, Kim SS, Cha HY, Jang SH, Chang DY, et al. Therapeutic effect of hepatocyte growth factor-secreting mesenchymal stem cells in a rat model of liver fibrosis. Experimental & Molecular Medicine, (2014); 46(8): e110.
- Cho K, Woo S, Seoh J, Han H, Ryu K. ‘Mesenchymal stem cells restore CCL4-induced liver injury by an antioxidative process’, Cell Biology International, (2012); 36(12): 1267–1274.
- Soleimani M, Nadri S. A protocol for isolation and culture of mesenchymal stem cells from mouse bone marrow, Nature Protocols. (2009); 4(1): 102–106,
- Kocabiyik B, Gumus E, Abas BI, Anik A, Cevik O. Human wharton-jelly mesenchymal stromal cells reversed apoptosis and prevented multi-organ damage in a newborn model of experimental asphyxia. Journal of Obstetrics and Gynaecology, (2022); 42(8):3568-3576.
- Maridas DE, Rendina-Ruedy E, Le PT, Rosen CJ. Isolation, culture, and differentiation of bone marrow stromal cells and osteoclast progenitors from mice. Journal of Visualized Experiments, (2018); 131: e56750.
- Handke M, Rakow A, Singer D, Miebach L, Schulze F, et al. Bone marrow from periacetabular osteotomies as a novel source for human mesenchymal stromal cells. Stem Cell Research & Therapy, (2023); 14(1): 315.
- Itoh A, Isoda K, Kondoh M, Kawase M, Kobayashi M, et al. Hepatoprotective Effect of Syringic Acid and Vanillic Acid on Concanavalin A-Induced Liver Injury. Biological and Pharmaceutical Bulletin, (2009); 32(7): 1215–1219.
- Chen Y, Chen S, Liu LY, Zou ZL, Cai YJ, et al. Mesenchymal stem cells ameliorate experimental autoimmune hepatitis by activation of the programmed death 1 pathway. Immunology Letters, (2014); 162(12): 222–228.
- Zatroch KK, Knight CG, Reimer JN, Pang DSJ. Refinement of intraperitoneal injection of sodium pentobarbital for euthanasia in laboratory rats (Rattus norvegicus). BMC Veterinary Research, (2016); 13:1-7.
- Chu T, Chan H, Hu T, Wang E, Ma Y, et al. Celecoxib enhances the therapeutic efficacy of epirubicin for Novikoff hepatoma in rats. Cancer Medicine, (2018); 7(6): 2567–2580.
- Charan J, Kantharia N. How to calculate sample size in animal studies? Journal of Pharmacology and Pharmacotherapeutics, (2013); 4(4): 303-6.
- Bozward AG, Ronca V, Osei-Bordom D, Oo YH. Gut-liver immune traffic: deciphering immune-pathogenesis to underpin translational therapy. Front Immunol, (2021); 12: 1–12
- Richardson N, Wootton GE, Bozward AG, Oo YH. Challenges and opportunities in achieving effective regulatory T cell therapy in autoimmune liver disease. Seminars in Immunopathology, (2022); 44(4): 461–474.
- Sirbe C, Simu G, Szabo I, Grama A, Pop TL. Pathogenesis of Autoimmune Hepatitis—Cellular and Molecular Mechanisms. International Journal of Molecular Sciences, (2021); 22(24): 13578.
- Balitzer D, Shafizadeh N, Peters MG, Ferrell LD, Alshak N, Kakar S. Autoimmune hepatitis: review of histologic features included in the simplified criteria proposed by the international autoimmune hepatitis group and proposal for new histologic criteria. Modern Pathology, (2017); 30(5): 773–783.
- Heneghan MA, McFarlane IG. Current and novel immunosuppressive therapy for autoimmune hepatitis. Hepatology, (2002); 35(1): 7–13.
- Ruiz, R, Kirk, AD. Long-Term Toxicity of Immunosuppressive Therapy. Transplantation of the liver 3rd ed. (2105); 1354-1363. Elsevier eBooks. URL: https://doi.org/10.1016/b978-1-4557-0268-8.00097-x
- Salehinejad P, Moshrefi M, Eslaminejad T. An overview on mesenchymal stem cells derived from extraembryonic tissues: Supplement sources and isolation methods. Stem Cells and Cloning: Advances and Applications, (2020); 13: 57–65.
- Oh SY, Choi YM, Kim HY, Park YS, Jung SC, et al. Application of Tonsil-Derived Mesenchymal Stem Cells in Tissue Regeneration: Concise Review. Stem Cells, (2019); 37(10): 1252–1260.
- Gopalarethinam J, Nair AP, Iyer M, Vellingiri B, Subramaniam MD. Advantages of mesenchymal stem cell over the other stem cells. Acta Histochemica, (2023); 125(4): 52041.
- Yamaguchi T, Sato H, Kato-Itoh M, Goto T, Hara H, et al. Interspecies organogenesis generates autologous functional islets. Nature, (2017); 542(7640): 191–196.
- Inoue Y, Iriyama A, Ueno S, Takahashi H, Kondo M, et al. Subretinal transplantation of bone marrow mesenchymal stem cells delays retinal degeneration in the RCS rat model of retinal degeneration. Experimental Eye Research, (2007); 85(2): 234–241.
- Alzahrani FA, El-Magd MA, Abdelfattah-Hassan A, Saleh AA, Saadeldin IM, et al. Potential Effect of Exosomes Derived from Cancer Stem Cells and MSCs on Progression of DEN-Induced HCC in Rats. Stem Cells Int. (2018 ); 27; 8058979.
- Peng L, Xie DY, Lin BL, Liu J, Zhu HP, et al. Autologous bone marrow mesenchymal stem cell transplantation in liver failure patients caused by hepatitis B: short-term and long-term outcomes. Hepatology, (2011); 54 (3): 820-828.
- Lanthier N, Lin-Marq N, Rubbia-Brandt L, Clement S, Goossens N, Spahr L. Autologous bone marrow derived cell transplantation in decompensated alcoholic liver disease: What is the impact on liver histology and gene expression patterns? Stem Cell Research & Therapy, (2017); 8(1): 1-10.
- Cao Q, Batey R, Pang G, Russell A, Clancy R. IL‐6, IFN‐γ and TNF‐α production by liver‐associated T cells and acute liver injury in rats administered concanavalin A. Immunology and cell biology, (1998); 76(6): 542-549.
- Cho K, Woo S, Seoh J, Han H, Ryu K. Mesenchymal stem cells restore CCl4‐induced liver injury by antioxidative process. Cell Biology International, (2012); 36(12): 1267–1274.
- Suk KT, Yoon JH, Kim MY, Kim CW, Kim JK, et al. Transplantation with autologous bone marrow‐derived mesenchymal stem cells for alcoholic cirrhosis: Phase 2 trial. Hepatology, (2016); 64(6): 2185-2197.
- Rani R, Tandon A, Wang J, Kumar S, Gandhi CR. Stellate Cells Orchestrate Concanavalin A–Induced Acute Liver Damage. The American Journal of Pathology, (2017); 187(9): 2008–2019.
- khaleel A, El-Sheakh AR, Suddek GM. Celecoxib abrogates concanavalin a-induced hepatitis in mice: Possible involvement of Nrf2/HO-1, JNK signaling pathways and COX-2 expression. International Immunopharmacology, (2023); 121: 110442.
- Chen L, Zhang C, Chen L, Wang X, Xiang B, et al. Human Menstrual Blood-Derived Stem Cells Ameliorate Liver Fibrosis in Mice by Targeting Hepatic Stellate Cells via Paracrine Mediators. Stem Cells Translational Medicine, (2016); 6(1): 272–284.
- Chi G, Pei J, Li X. The imbalance of liver resident macrophages polarization promotes chronic autoimmune hepatitis development in mice. PeerJ, (2023); 11:e14871.
- Kato M. Involvement of IL-10, an anti-inflammatory cytokine in murine liver injury induced by concanavalin a. Hepatology Research, (2001);20(2): 232–243.
- Chen L, Xie XJ, Ye YF, Zhou L, Xie HY, et al. Kupffer cells contribute to concanavalin A-induced hepatic injury through a Th1 but not Th17 type response-dependent pathway in mice. Hepatobiliary & Pancreatic Diseases International, (2011); 10(12): 171–178.
- Chen Y, Jeffery HC, Hunter S, Bhogal R, Birtwistle J, et al. Human intrahepatic regulatory T cells are functional, require IL‐2 from effector cells for survival, and are susceptible to Fas ligand‐mediated apoptosis. Hepatology, (2016); 64(1): 138–150.
- Qu M, Yuan X, Liu D, Ma Y, Zhu J, et al. Bone Marrow-Derived Mesenchymal Stem Cells Attenuate Immune-Mediated Liver Injury and Compromise Virus Control During Acute Hepatitis B Virus Infection in Mice. Stem cells and development, (2017); 26(11):818–827.
- Wang H, Zhang H, Huang B, Miao G, Yan X, et al. Mesenchymal stem cells reverse high‑fat diet‑induced non‑alcoholic fatty liver disease through suppression of CD4+ T lymphocytes in mice. Molecular Medicine Reports, (2018); 17(3): 3769-3774.
- Caplan AI, Dennis JE. Mesenchymal stem cells as trophic mediators. Journal of Cellular Biochemistry, (2006); 98(5): 1076–1084.
- Reger R L, Tucker A, Wolfe MR. Differentiation and characterization of human MSCs. Humana Press eBooks, (2008); 93-107
- Kurtz A. Mesenchymal Stem Cell Delivery Routes and Fate. International Journal of Stem Cells, (2008); 1(11): 1–7.
- Barbash IM, Chouraqui P, Baron J, Feinberg MS, Etzion S, et al. Systemic Delivery of Bone Marrow–Derived Mesenchymal Stem Cells to the Infarcted Myocardium. Circulation, (2003); 108 (7): 863–868.
- Ortiz LA, Gambelli F, McBride C, Gaupp D, Baddoo M, et al. Mesenchymal stem cell engraftment in lung is enhanced in response to bleomycin exposure and ameliorates its fibrotic effects. Proceedings of the National Academy of Sciences, (2003); 100 (14): 8407–8411.
- Laird DJ, von Andrian UH, Wagers AJ. Stem cell trafficking in tissue development, growth, and disease. Cell, (2008); 132(4): 612-630.
- Chen Y, Xiang LX, Shao JZ, Pan RL, Wang YX, et al. Recruitment of endogenous bone marrow mesenchymal stem cells towards injured liver. Journal of Cellular and Molecular Medicine, (2009); 14(6b): 1494–1508.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0![]()