

Full Length Research Article
Prevalence, Viral Load Dynamics, and Factors Influencing SARS-CoV-2 Infection: A Cross-sectional Study in Lahore, Pakistan
Ali Ahsan1&, Zahra Kalim2&, Muhammad Abdul Qadeer3, Muhammad Saif Ullah Khan3, Muhammad Imran3, Muhammad Anees Sharif3, Kiran Jalil1, Zoha Rubab4, and Chaudhry Ahmed Shabbir5*
Adv. life sci., vol. 12, no. 1, pp. 98-104, February 2025
*- Corresponding Author: Chaudhry Ahmed Shabbir (Email: ahmed.chaudhry@adelaide.edu.au)
Authors' Affiliations
2. Institute of Microbiology, Government College University Faisalabad – Pakistan
3. University Institute of Medical Laboratory Technology, Faculty of Allied Health Sciences, The University of Lahore, Lahore-54590 – Pakistan
4. Department of Physical Therapy, The Islamia University of Bahawalpur – Pakistan
5. Faculty of Health and Medical Science, Adelaide Medical School, The University of Adelaide – Australia
[Date Received: 12/08/2023; Date Revised: 07/06/2024; Date Published: 31/12/2024]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The pandemic caused by novel coronavirus has caused disaster worldwide and impacted the clinical settings with huge burden. The virus presented with diverse patterns of severity and the gold standard testing for corona virus was real-time PCR.
Methods: This study aimed to understand the impact of the coronavirus healthcare crisis by examining SARS-CoV-2 prevalence and viral load patterns. A substantial population sample from Lahore's diagnostic center was analyzed. A total of 17,260 samples were received out of which 1548 samples were meticulously analyzed to study the distribution of SARS-CoV-2 patients by age group and gender between October 2021 and December 2022. CT ranges in positive cases were examined across various age groups. Descriptive statistics for viral load, factoring in gender, age, and vaccination status, were reported. To comprehensively assess the influence of gender and age on viral load, a multivariate analysis employing two-way ANOVA was conducted, yielding valuable insights.
Results: Among the sampled individuals, the positive patients (n=1250, 80.7%) were predominantly male (mean age 36.08 years), while females (n=298, 19.3%) had a mean age of 37.69. The positivity prevalence was 8.96% with CT values spanning 12 to 35. Mainly, cases occurred in CT ranges 26-30 (29.97%) and 31-35 (28.43%). Males showed higher mean viral load (25.88 ± 5.75) than females (23.25 ± 4.94). Age groups didn't significantly alter viral load; vaccination showed no significant viral load association. Gender and age collectively influenced viral load dynamics per multiple logistic regression.
Conclusion: The study emphasizes the significant SARS-CoV-2 burden and the necessity for sustained surveillance and prevention. Gender and age impacted viral load dynamics, while vaccination's direct influence was inconclusive. Investigating the intricate relationship between gender, age, viral load, and outcomes is warranted for improved epidemiological comprehension and effective prevention strategies.
Keywords: SARS-CoV-2; Viral load; Prevalence; Vaccination; Public health; Infection dynamic
Introduction![]()
In late 2019, a viral pneumonia-like illness with an unknown cause emerged in the Huainan seafood wholesale market in Wuhan, China. The virus responsible for this illness was later identified as Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) [1,2]. The rapid global spread of the virus led to its declaration as a global pandemic by the World Health Organization (WHO) [3]. Coronaviruses, although not new to humanity, have caused significant epidemics in the past, including the severe acute respiratory syndrome (SARS) epidemic in China in 2002 and the Middle East Respiratory Syndrome Coronavirus (MERS-CoV) epidemic in Saudi Arabia in 2012 [1,4].
In Pakistan, the Ministry of National Health Services Regulations and Coordination, Government of Pakistan, confirmed the first two cases of COVID-19 on February 27, 2020, in Karachi and Islamabad, with a travel history to Iran [5]. According to the recent report by Dawn newspaper of Pakistan on 30th June 2024, Pakistan had reported 641 COVID-19-positive patients — the highest number of daily cases in over three months since 10th of March 2024, when the daily tally was 723. To date, the ministry of health reported the virus quickly spread nationwide, placing a substantial burden on healthcare providers and state governments. While a zero-tolerance vaccination policy was implemented, reinfection concerns arose due to mutations in the viral genome.
Various factors have been identified to contribute to patient morbidity and mortality, including the virus' differential behavior based on gender and age group [6]. Severe infections have been observed in immunocompromised patients and individuals at extreme ages, such as adults over 60 years and children under 15 years [7]. Studies have also indicated that gender plays a role in disease spread, with males being more susceptible to virus infection and exhibiting higher mortality rates than females [8]. Vaccines such as the BNT162b2 mRNA vaccine developed by Pfizer-BioNTech, and the ChAdOx1 nCoV-19 viral vector vaccine developed by Oxford-AstraZeneca have effectively reduced infections. However, vaccination is associated with lower infectivity (reflected by higher CT values), and rare transmission cases can still occur. Examining the variation in viral dynamics, such as viral load, among different sexes, age groups, and vaccinated individuals can provide valuable insights into the role of these factors in disease severity. Understanding how viral dynamics relate to other factors influencing disease outcomes, including mortality rates, remains uncertain. Some studies have reported a significant association between viral load and disease severity, length of hospital stay, and disease transmission [9-11]. However, other studies have found no statistically significant relationship between viral load and disease prognosis [12]. While Pakistani scientists have conducted several studies investigating the role of viral load concerning gender and age, limited information exists regarding the impact of vaccination on reinfection. Therefore, the current study aimed to investigate viral dynamics concerning gender, age, and vaccination status.
This manuscript utilized various statistical analyses to explore the association between viral load and multiple factors. The t-test was employed to compare the mean viral load between different gender groups. One-way ANOVA assessed the mean viral load across various age groups and vaccination status. The univariate analysis examined the individual relationship between viral load and each factor. A multivariate analysis approach was utilized to examine the combined impact of age groups, gender, and vaccination status on viral load. Such statistical approaches helped to thoroughly investigate the viral dynamics and their relation to different clinical and demographic variables. T-tests and ANOVA were used to compare means among different groups because each variable in the study comprises two or more population sets. One-way ANOVA was examined to analyze whether group means of a specific dependent variable significantly differ after exposure to an independent variable. Furthermore, two-way ANOVA was used to analyze variance with multiple independent variables. [9]. Overall, understanding the dynamics of viral load and its association with various factors can contribute to better comprehending the disease severity. This knowledge can aid in developing effective strategies for managing the ongoing pandemic.
Methods![]()
Study Settings, Design, and Population
This manuscript reports the findings from a cross-sectional study conducted at a private health care laboratories center in Lahore, Pakistan. Lahore is an important metropolitan city, culturally and historically, with a population exceeding 13.5 million in Pakistan. It contains an economic center of Punjab, with the largest number of people coming to work here every year. This study examined 1548 positive samples that were collected from different locations for testing across the country between October 2021 and December 2022. Nasopharyngeal samples were collected from each suspected individual and swabs inserted in Virogene viral transport medium (VTM). The detection limit in polymerase chain reaction (PCR) was determined by the threshold cycle (CT), and it is the least number of cycles to be undertaken for reaching the detection limit. Analyses were considered positive when CT values were less than 35, following the manufacturer's instruction. The study included only those participants who were diagnosed positive for coronavirus PCR test within seven days, and they provided their consent to use their demographics for conducting this study. The patients denying consent or diagnosed for COVID-19 test more than a week were excluded from this study.
Sample Processing, RNA Extraction, and Amplification
RNA was extracted using the GF-1 Viral Nucleic Acid Extraction Kit by Vivantis Technologies, Malaysia, following the manufacturer's recommended protocol. Real-time RT-PCR amplification was done on the extracted RNA using commercially available Bosphore® Novel Coronavirus (2019-nCoV) detection kit v4, Turkey. The conventional primers of the diagnostic kit were designed targeting the viral genome-specific genes. These genes include the S-gene, N-gene, and ORF1ab-gene. RT-PCR was done in a Turkey-based Anatolia Geneworks Montania 4896 thermal cycler. The conditions were optimized based on the manufacturer's instructions. Graphical representation and CT values were noted after 40 amplification cycles.
Variables
CT, being the marker of viral load, was categorized into four groups:<15, 16-20, 21-25, 26-30, and 31-35. Age details of the patients were taken from their demographic proforma and put into the following groups: <15, 15-30, 31-45, 46-60, and 61-75 years.
Statistical Analysis and Data Arrangement
Tables were created through Microsoft Excel 2018.Descriptive statistics were applied to evaluate the proportion of CT values, while cross-tabulation was performed to determine the frequency distribution between CT and age groups. The data were presented as frequency (N), percentage (%), mean (x̄), standard deviation (SD), 95% confidence intervals (CI), p-value 0.001 (P), degree of freedom (df), Mean Square, and F value (F). T-test was applied to compare the mean of viral load between both genders. One-way Analysis of Variance (ANOVA) were conducted to determine statistically significant mean differences between three or more independent groups. Multivariable analysis using two-way ANOVA assessed the statistically significant difference between the means of the dependent variable (CT value) and independent variables (gender, age, and vaccination status). The statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) V.20.
Ethical Approval
Before the commencement of the study, ethical approval was obtained from the research laboratory (Ethical Approval Number IDC/HR/RR/09-36).
Results![]()
Distribution of SARS-CoV-2 Patients by Age Groups and Gender
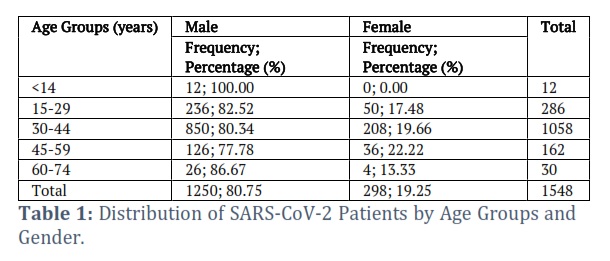
A total of 17,260 samples were received throughout the study period; 1548 (8.96%) were detected positive. The CT values of the positive samples ranged from 12 to 35. Most positive cases (29.97%, n=464) were diagnosed in the CT range of 26-30, followed by the CT range of 31-35 (28.43%, n=440), 21-25 (24.10%, n=373), 16-20 (12.39%, n=192), and <15 (5.11%, n=79). The data showed that, out of the total, in the age group <14, all 12 patients were males, with no female cases reported. In the age group 15-29, there were 236 male cases (82.52%) and 50 female cases (17.48%), totaling 286 cases. Among patients aged 30-44, 850 were male cases (80.34%) and 208 female cases (19.66%), amounting to 1058 cases. In the age group 45-59, 126 patients were male (77.78%), and 36 were female (22.22%), totaling 162 cases. For patients aged 60-74, there were 26 male cases (86.67%) and four female cases (13.33%), totaling 30 cases. Across all age groups, there were 1250 male cases (80.75%) and 298 female cases (19.25%), amounting to 1548 cases (Table 1).
Frequency Distribution of CT Ranges across Age Groups in SARS-CoV-2 Positive Individuals
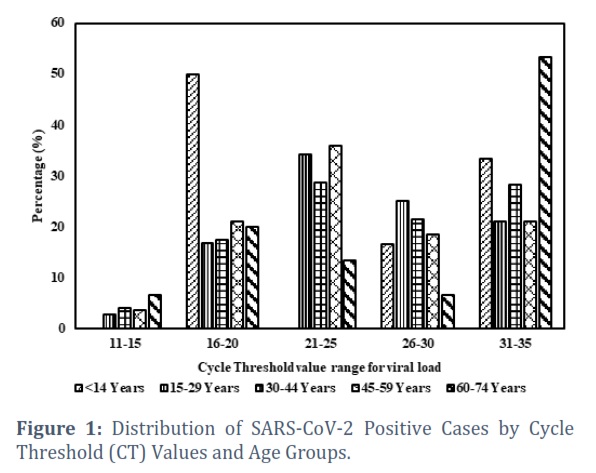
Figure 1 provides insights into the distribution of CT ranges across different age groups, highlighting the varying frequencies of individuals with different CT ranges within each age group. The results can be a valuable reference to understand the relationship between age and CT values in the studied population. The mean CT value for all positive cases was 25.42 (SD ± 5.68). The mean CT values for different age groups are presented in Figure 1. The cross-tabulation statistics between age groups and CT ranges are presented in the table 2. The age groups were categorized as <14, 15-29, 30-44, 45-59, and 60-74, while the CT ranges were categorized as 11-15, 16-20, 21-25, 26-30, and 31-35. The highest frequency of individuals with CT range 16-20 is found in the age group 30-44, followed by the age group 45-59. The age group 15-29 also shows a considerable frequency in this CT range. For the CT range 21-25, the highest frequency is observed in the age group 30-44, followed by the age group 45-59. Similarly, for the CT range 26-30, the highest frequency is found in the age group 30-44. (Figure 1).
The x-axis in Figure 1 represents the cycle threshold (CT) value ranges, which are categorized into intervals of 5, spanning from <15 to 35 (e.g., 16-20, 21-25, 26-30). The y-axis denotes the number of positive SARS-CoV-2 cases within each CT value category. Each CT value group is further stratified by age groups, with intervals of 15 years, ranging from <14 to 64 years old (e.g., 15-29, 30-44). This stratification allows for an analysis of the distribution of viral loads across different age cohorts, facilitating the assessment of potential correlations between age and viral load dynamics.
Descriptive Statistics of Viral Load by Gender, Age Groups, and Vaccination Status
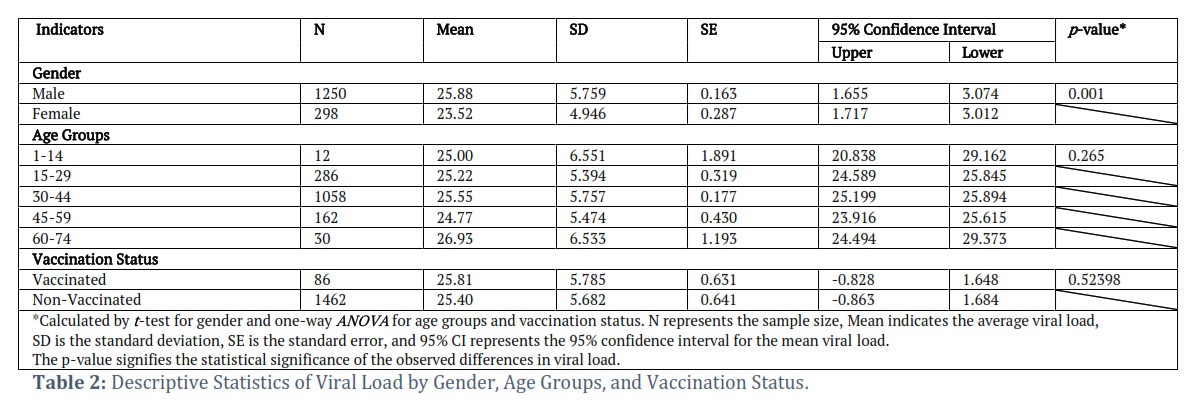
Table 2 presents the descriptive statistics for viral load across different variables in the study, including gender, age groups, and vaccination status. For gender, the mean viral load for males is 25.88 ±5.759), which is significantly higher than that of females (mean=23.52 ± 4.946; p < 0.001). Among the different age groups, no significant differences in viral load were observed (p > 0.05). The mean viral load for each age group ranged from 24.77 to 26.93, with standard deviations varying from 5.474 to 6.533. Regarding vaccination status, no significant difference in viral load was found between vaccinated and non-vaccinated individuals (p = 0.52398). The mean viral load for vaccinated individuals was 25.81 ±5.785, while for non-vaccinated individuals, it was 25.40 ±5.682.
The statistical tests used were t-tests for gender comparisons and one-way ANOVA for age group and vaccination status comparisons. The p-values indicate the level of significance and were used to determine whether the observed differences in viral load are statistically significant. These findings provide insights into the gender distribution among SARS-CoV-2 patients across different age groups, highlighting variations in the prevalence of infection among males and females. In the case of descriptive statistics of viral load by gender, age groups, and vaccination status, the multivariable analysis using two-way ANOVA indicated no statistically significant interaction effects between age and vaccination status on CT values (F=0.067, p=0.935, df=8). No statistically significant differences in mean CT values were observed among age groups (F=0.697, p=0.596, df=4). Furthermore, the study examined the relationship between vaccination status and CT values. Among the positive cases, 63.48% (n=982) were unvaccinated, 25.65% (n=397) had received one dose of a COVID-19 vaccine, and 10.87% (n=169) had received two doses.
Multivariate analysis
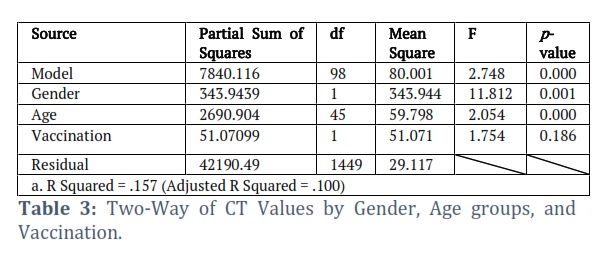
The two-way ANOVA analysis examined the relationship between viral load (measured by CT values) and two independent variables: gender and age groups. The analysis results revealed a significant overall effect of the model (p < 0.001), indicating that the combined factors of gender and age groups have a statistically significant impact on viral load. Specifically, the partial sum of squares for the gender variable was 343.9439, with 1 degree of freedom (df), resulting in a mean square value of 343.944. The associated F-value was 11.812, indicating a significant effect of gender on viral load (p = 0.001). Similarly, the partial sum of squares for the age variable was 2690.904, with 45 degrees of freedom, resulting in a mean square value of 59.798. The associated F-value was 2.054, indicating a significant effect of age groups on viral load (p < 0.001).
On the other hand, the variable of vaccination status did not show a significant effect on viral load. The partial sum of squares for vaccination was 51.07099, with 1 degree of freedom, resulting in a mean square value of 51.071. The associated F-value was 1.754, suggesting no statistically significant association between vaccination status and viral load (p = 0.186). The analysis also provided information on the model's goodness-of-fit, with an R-squared value of 0.157, indicating that approximately 15.7% of the variance in viral load can be explained by the combined factors of gender and age groups. The adjusted R-squared value, considering the degrees of freedom, was 0.100. Overall, the results of the two-way ANOVA analysis suggest that both gender and age groups have a significant influence on viral load. At the same time, vaccination status does not show a significant association. These results support the relevance of considering gender and age to understand the viral load dynamics of infection with SARS-CoV-2. (Table 3).
Figures & Tables
The aim of the present study is to investigate the prevalence and viral load dynamics of SARS-CoV-2 among a large population sample collected at a private healthcare center in Lahore, Pakistan. The findings yielded interesting insights into the distribution of SARS-CoV-2 among different age groups, genders, and the potential impact of vaccination on viral load dynamics. A prevalence positivity rate of 8.96% among the 17,260 collected samples highlights the substantial SARS-CoV-2 infection burden in the study population. The quoted results show the continuous process of viral infection in the community and underscore the need for rigorous surveillance and preventive measures to control the spread. Numerous studies have already reported on viral shedding and transmission rates, and SARS-CoV-2 appears to follow the same pattern of transmission and spread. [13; 14].
CT value analysis as a measure of viral load revealed variation in viral load distribution among different CT ranges. Most positive cases fell within the Ct ranges of 26-30 (29.97%) and 31-35 (28.43%). These findings suggest that many infected individuals had a moderate to low viral load, as indicated by higher CT values. It is worth noting that the CT values provide an indirect measure of viral load, and caution should be exercised in interpreting these results as a direct indication of infectiousness. In 2021 Mahallawi et al. conducted a study on 3006 SARS-CoV-2 positive patients and revealed no statistically significant difference in CT distribution among the age groups [15].
The younger age group also indicated no significant difference in viral load between age groups below 18 years [16]. In 2020 Kleiboeker et al. stated the same results; no noticeable variation in mean and median values between age groups was seen in their study [17]. Despite similar results to previous studies, a study by Jones et al. revealed a conflict regarding the association between Ct value and age group. The study of 3303 COVID-19-positive patients indicated a minor difference in viral load distribution between young and old age groups; this variation in viral load between different age groups is due to differences in PCR systems used [18]. In 2020 Kim et al. also showed a significant association between viral load in elderly patients (above 80 years old) [19].
Gender differences in viral load were observed in the present study. Males exhibited a significantly higher mean viral load; 25.88 ± 5.75 than the females; 23.25 ± 4.94). This finding aligns with previous studies that reported a higher susceptibility to SARS-CoV-2 infection and more severe disease outcomes in males than females [20]. The underlying reasons for this gender disparity in viral load and disease severity require further investigation. Potential factors contributing to this difference may include hormonal, immunological, and behavioral factors such as sleep wake cycle disruption, poor dietary habits and family history of any sickness.
Age groups were also found to influence viral load dynamics. However, contrary to expectations, no significant differences in viral load were observed among the different age groups from both extremities of the age either younger or older. Previous studies have suggested that older individuals may have higher viral loads and are more likely to experience severe disease [21]. However, this study did not find significant variations in viral load across age groups. The age distribution of the study population and the inclusion of only symptomatic individuals in the sample may have influenced these results. Further studies with larger sample sizes and a more comprehensive age range are needed to elucidate the relationship between age and viral load in SARS-CoV-2 infection [22-24].
One crucial aspect explored in this study was the potential impact of vaccination status on viral load dynamics. Interestingly, no significant association was found between vaccination status and viral load. The partial sum of squares for vaccination was 51.07099, with 1 degree of freedom, resulting in a mean square value of 51.071. The associated F-value was 1.754, suggesting no statistically significant association between vaccination status and viral load (p = 0.186). This finding suggests that vaccination may not directly impact viral load in infected individuals. However, it is crucial to note that vaccination has been shown to significantly reduce the risk of severe disease, hospitalization, and mortality. Vaccination remains a critical tool in controlling the spread of SARS-CoV-2 and mitigating the impact of the virus at the population level. The current study indicated no association between viral load and vaccination status. In 2021 Kissler et al. conducted a study including 37 vaccinated and 136 non-vaccinated patients, revealing no significant difference in mean viral load between vaccinated and non-vaccinated individuals [21]. A similar study to assess the viral load between vaccinated and non-vaccinated patients also showed the same results [22-26]. These results were consistent with our studies; however, vaccinated individuals' booster dose decreased viral load. The reduced viral load after a successful booster dose hints toward lowered infectiousness and the effectiveness of the booster dose.
The multivariate two-way ANOVA analysis demonstrated that gender and age groups collectively influenced viral load dynamics. The significant effect of gender on viral load, with males having a higher mean viral load than females, highlights the need to explore further the underlying factors contributing to this disparity. The significant effect of age groups suggests that age influences the severity of infection, although the lack of significant differences in viral load among age groups warrants additional investigation.
The findings of this study contribute to our understanding of the epidemiology of SARS-CoV-2 in the study population and provide insights into factors that may influence viral load dynamics. The importance of the current study can be vested in its good sample size, two-way ANOVA multivariate analysis, from real-world data reported, while investigating the possible important factors taken under consideration, those being gender, age groups, vaccination status, etc. There are several limitations, however, consensus emerged that these results would have important implications for health: these results further support the importance of vaccination, guide gender/age-specific health strategies, promote strategies regarding the management of disease severity, and support research and surveillance programs that incrementally increase the public's trust in health authorities due to evidence of reduced viral loads attributable to vaccination. One of the limitations of our study are its cross-sectional design, which really restricts the establishing of causal relationships and the determination of the chronological sequence of events. The study participants belonged to specific populations at one point. A major limitation is the lack of ability to trace changes in viral load over time that captures the dynamic nature of the SARS-CoV-2 infection process; this could have been dealt with by a longitudinal study design. Further, this kind of study is sample-dependent in that it relied on samples from one health center in Lahore, Pakistan, which may have introduced some form of selection bias, whereby the sample may not be representative of the full population, making it difficult to generalize these findings to any other region or its population. It is also significant to remark that the study population comprises those who present for screening likely because they suspect they are infected; hence, there may be no account of asymptomatic or mildly symptomatic cases. Such exclusion might bear a consequence for understanding the overall rates and dynamics of SARS-CoV-2 infection, as these cases could have different patterns of viral load.
The study provides interesting insights into the prevalence and viral load dynamics of SARS-CoV-2 in a population setting. The results indicate that gender and age group play crucial roles in determining viral load, whereas vaccination does not appear to have any direct impact. This information is important for understanding the behavior of the infection and will help public health practitioners to develop innovative strategies and interventions to control the spread of SARS-CoV-2. To better understand the epidemiology of SARS-CoV-2 and to gain a solid grasp of its behavior, future research should continue to explore the complex relationships between age, gender, and viral load. Another future approach for new researchers could be understanding the molecular insights of viral load or threshold cycle associated with patients, molecular role of vaccination and their role in reducing CT values.
Acknowledgement
This study highlights our research team's dedication and self-reliance, accomplished without financial support. We thank our exceptional laboratory personnel and all those who inspired and supported our pursuit of scientific excellence in advancing COVID-19 diagnostics.
Author Contributions
AA and ASC designed the study, AQ, SU, MI, MAS and ZR collected and analyzed the data, ZK drafted the manuscript. ASC supervised and dealt with the review process. All authors discussed and approved the manuscript and submitted with mutual consent.
The authors declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- Peeri NC, Shrestha N, Rahman MS, Zaki R, Tan Z, et.al., The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: what lessons have we learned?. International Journal of Epidemiology, (2020); 49(3): 717-26.
- Wang L, Wang Y, Ye D, Liu Q. Review of the 2019 novel coronavirus (SARS-CoV-2) based on current evidence. International Journal of Antimicrobial Agents, (2020); 55(6): 105948.
- Kordzadeh-Kermani E, Khalili H, Karimzadeh I. Pathogenesis, clinical manifestations and complications of COVID-19. Future Microbiology, (2020); 15(13): 1287-305.
- Yan X, Zou Y. Optimal and sub-optimal quarantine and isolation control in SARS epidemics. Mathematical and Computer Modelling, (2008); 47(1-2): 235-45.
- Ullah R, Rana MS, Qadir M, Muhammad U. First COVID-19 related death in Pakistan in a patient with a travel history in Saudi Arabia. Asian Pacific Journal of Tropical Medicine, (2020); 13(8): 375-377.
- Peckham H, de Gruijter NM, Raine C, Radziszewska A, Ciurtin C, et al., Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nature Communications, (2020); 11(1): 6317.
- Naja M, Wedderburn L, Ciurtin C. COVID-19 infection in children and adolescents. British Journal of Hospital Medicine, (2020); 81(8): 1-0.
- Jin JM, Bai P, He W, Wu F, Liu XF, et al., Gender differences in patients with COVID-19: focus on severity and mortality. Frontiers in Public Health, (2020); 8: 545030.
- Magleby R, Westblade LF, Trzebucki A, Simon MS, Rajan M, et al., Impact of severe acute respiratory syndrome coronavirus 2 viral load on risk of intubation and mortality among hospitalized patients with coronavirus disease 2019. Clinical Infectious Diseases, (2021); 73(11): e4197–e4205.
- Shrestha NK, Marco Canosa F, Nowacki AS, Procop GW, Vogel S, et al., Distribution of transmission potential during no severe COVID-19 illness. Clinical Infectious Diseases, (2020); 71(11): 2927-32.
- Walsh KA, Jordan K, Clyne B, Rohde D, Drummond L, et al., SARS-CoV-2 detection, viral load and infectivity over the course of an infection. Journal of Infection, (2020); 81(3): 357-371.
- Mahallawi WH, Alsamiri AD, Dabbour AF, Alsaeedi H, Al-Zalabani AH. Association of viral load in SARS-CoV-2 patients with age and gender. Frontiers in Medicine, (2021); 8: 608215.
- Maltezou HC, Magaziotou I, Dedoukou X, Eleftheriou E, Raftopoulos V, et al., Children and adolescents with SARS-CoV-2 infection: epidemiology, clinical course and viral loads. The Pediatric Infectious Disease Journal, (2020); 39(12): e388-92.
- Kleiboeker S, Cowden S, Grantham J, Nutt J, Tyler A, et al., SARS-CoV-2 viral load assessment in respiratory samples. Journal of Clinical Virology, (2020); 129: 104439.
- Jones TC, Biele G, Mühlemann B, Veith T, Schneider J, et al., Estimating infectiousness throughout SARS-CoV-2 infection course. Science, (2021); 373(6551): eabi5273.
- Kim Y, Cheon S, Jeong H, Park U, Ha NY, et al., Differential association of viral dynamics with disease severity depending on patients’ age group in COVID-19. Frontiers in Microbiology, (2021); 12: 712260.
- Chan JF, Kok KH, Zhu Z, Chu H, To KK, et al., Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerging Microbes & Infections, (2020); 9(1): 221-36.
- Kissler SM, Fauver JR, Mack C, Tai CG, Breban MI, et al., Anderson DJ, Metti J, Khullar G, Baits R. Viral dynamics of SARS-CoV-2 variants in vaccinated and unvaccinated persons. New England Journal of Medicine, (2021); 385(26): 2489-2491.
- Zorob T, Farooqi MA, Ahsan A, Zaki A, Rathore MA, et al., Prevalence and Trends in Hepatitis B & C Virus among Blood Donors in Pakistan: A Regional Transfusion Center Study. Livers, (2023); 3(2): 271-281.
- Farooqi MA, Ahsan A, Yousuf S, Shakoor N, Farooqi HM. Seroprevalence of hepatitis E virus antibodies (IgG) in the community of Rawalpindi. Livers, (2022); 2(3): 108-115.
- Zahid AS, Farooqi HM, Ahsan A, Farooqi MA, Kausar F, et al., Comparative analysis of antigenic strength and in vivo serum antibodies concentration of tetanus toxoid vaccine adsorbed in Pakistan. Saudi Journal of Biological Sciences, (2022); 29(8): 103337.
- Singanayagam A, Hakki S, Dunning J, Madon KJ, Crone MA, et al., Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study. The Lancet Infectious Diseases, (2022); 22(2): 183-195.
- Levine-Tiefenbrun M, Yelin I, Katz R, Herzel E, Golan Z, et al., Initial report of decreased SARS-CoV-2 viral load after inoculation with the BNT162b2 vaccine. Nature Medicine, (2021); 27(5): 790-792.
- Shoaib N, Noureen N, Faisal A, Zaheer M, Imran M, et al., Factors associated with cycle threshold values (Ct-values) of SARS-CoV2-rRT-PCR. Molecular Biology Reports, (2022); 49(5): 4101-4106.
- Ahsan A, Shabbir CA, Qadeer MA, Rafiq A, Yaseen A, et al., Comparison of Rapid Antigen Test with RT-PCR for COVID-19 Diagnosis: Performance and Limitation. Russian Open Medical Journal, (2024); 13(2): e0210.
- Khan R, Javed H, Fatima W, Ahsan A, Khan MI, et al., The Unspoken Wounds: Understanding the Psychological Impact on Healthcare Professionals Fighting COVID‐19 in Pakistan. Transboundary and Emerging Diseases, (2024); 2024(1): 3364960. John Wiley & Sons, Inc.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0![]()


