

Review Article
Diabetic Peripheral Neuropathy: Navigating Controversies and Pioneering Advances
Saif Khan1*, Saheem Ahmad2, Mahvish Khan3, Mohtashim Lohani4, Mohammad Sajid Khan5, Mohammad Haneef6
Adv. life sci., vol. 12, no. 1, pp. 01-12, February 2025
*– Corresponding Author: Saif Khan (Email: sf.khan@uoh.edu.sa)
Authors' Affiliations
2. Department of Clinical Laboratory Science, College of Applied Medical Science, University of Ha’il, Ha’il-55473 – Saudi Arabia
3. Department of Biology, College of Science, University of Ha’il, Ha’il-55473 – Saudi Arabia
4. Medical Research Centre, College of Applied Medical Sciences, Jazan University, Jazan – Kingdom of Saudi Arabia
5. Department of Biochemistry, Faculty of Life Sciences, Aligarh Muslim University, Aligarh –India
6. Department of Bioengineering, Integral University, Lucknow 226026, Uttar Pradesh – India
[Date Received: 27/10/2024; Date Revised: 02/12/2024; Date Available Online: 31/12/2024]
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
This review examines Diabetic Peripheral Neuropathy (DPN), a significant complication of diabetes affecting nearly half of diabetic patients. DPN is crucial to understand due to its high prevalence and profound impact on patients’ quality of life, causing pain, sensory loss, motor dysfunction, and heightened risks of foot ulcers and amputations. As a leading cause of disability, grasping DPN’s pathophysiology, early diagnosis, and treatment options are essential for alleviating its burden. Key facets of DPN include its complex pathophysiology stemming from chronic hyperglycemia, oxidative stress, inflammation, and vascular problems that damage nerves. The review highlights the rising rates of diabetes and DPN in regions like Saudi Arabia, noting that factors such as poor glycemic control, prolonged diabetes duration, and comorbidities like hypertension significantly contribute to DPN progression. Diagnostic challenges are also addressed; traditional nerve conduction studies are gold standards yet limited in detecting early-stage neuropathy, especially small-fiber damage. Emerging methods, like skin biopsy and corneal confocal microscopy, show promise for earlier detection. Treatment mainly focuses on glycemic control and pain management without reversing nerve damage. Innovative therapies targeting DPN mechanisms include antioxidant treatments, anti-inflammatory agents, and phytomedicine, which utilizes bioactive compounds for their neuroprotective effects. The review concludes by stressing the need for ongoing research into DPN's molecular mechanisms and the development of personalized medicine approaches, which could significantly enhance patient outcomes.
Keywords: Diabetic Peripheral Neuropathy; DPN induced disability; DPN Pathophysiology; DPN treatment; DPN controversies
Introduction![]()
Definition and overview of Diabetic Peripheral Neuropathy (DPN).
Diabetic Peripheral Neuropathy (DPN) is a common and severe complication of diabetes mellitus, affecting the peripheral nervous system, which includes all nerves outside the brain and spinal cord. DPN primarily impacts the sensory nerves, though motor and autonomic nerves can also be involved. This condition is characterized by damage to the peripheral nerves, leading to symptoms such as pain, numbness, tingling, and weakness, particularly in the extremities like the feet and hands. It is often progressive and can result in significant morbidity, including a reduced quality of life due to chronic pain and an increased risk of foot ulcers, infections, and amputations. DPN is classified under the broader term "diabetic neuropathy," which encompasses various forms of nerve damage related to diabetes. However, DPN specifically refers to the peripheral nervous system involvement and excludes other types such as autonomic neuropathy or focal neuropathy. Diabetic Peripheral Neuropathy is particularly concerning because of its insidious onset and the fact that early stages may be asymptomatic, making it difficult to diagnose without regular screening. DPN specifically refers to the damage of peripheral nerves, which are responsible for transmitting signals between the central nervous system (the brain and spinal cord) and the rest of the body1. The development of DPN is multifactorial, with hyperglycemia (high blood sugar levels) being the most significant contributing factor. Prolonged exposure to elevated glucose levels leads to oxidative stress, inflammation, and damage to small blood vessels that supply the peripheral nerves. This impaired blood flow results in a lack of oxygen and nutrients to the nerves, causing degeneration of the nerve fibers. In addition to hyperglycemia, other factors like dyslipidemia (abnormal cholesterol levels), hypertension (high blood pressure), and lifestyle factors such as smoking and obesity contribute to the progression of DPN. Genetics also play a role in determining an individual's susceptibility to developing neuropathy. Insulin resistance, a hallmark of type 2 diabetes, further exacerbates these metabolic disturbances, creating a vicious cycle of nerve damage and impaired nerve function.
Importance of studying DPN-induced disability.
DPN is one of the most common complications of diabetes, yet it remains an under-recognized and under-studied condition. This condition significantly contributes to the global burden of disability among people living with diabetes. The importance of studying DPN and the disability it induces lies in its prevalence, debilitating consequences, and its association with significant impairments in quality of life. Research on DPN is essential not only for understanding the mechanisms of this complex condition but also for developing effective interventions to mitigate the associated disabilities. DPN affects up to 50% of people with diabetes, particularly those who have had the disease for a prolonged period or who have poor glycemic control [1]. It primarily affects the sensory nerves, causing symptoms such as pain, tingling, and numbness in the extremities, particularly in the feet and hands. Over time, this nerve damage can progress to motor dysfunction, leading to muscle weakness, balance issues, and difficulties with mobility [2]. The sensory and motor dysfunctions associated with DPN often result in a progressive loss of function, severely affecting daily activities and overall independence. One of the most severe consequences of DPN is the increased risk of foot ulcers and lower-limb amputations. Due to the loss of sensation in the feet, minor injuries or pressure points may go unnoticed, allowing them to develop into serious infections. Approximately 15% of patients with DPN will develop foot ulcers, and up to 85% of diabetes-related amputations are preceded by a foot ulcer [3]. Amputations not only have a significant physical impact but are also associated with severe emotional and psychological consequences, including depression and anxiety. Moreover, individuals who undergo amputation often experience diminished mobility, dependence on caregivers, and a substantial decline in quality of life. In addition to physical disability, DPN also significantly impacts mental health. Chronic neuropathic pain, a common feature of DPN, is associated with a high prevalence of depression and anxiety. The constant pain can disrupt sleep, exacerbate stress, and limit participation in social and occupational activities, leading to social isolation [4]. The psychological toll of living with chronic pain and functional limitations further emphasizes the need to prioritize research on DPN and its associated disabilities. Studying DPN-induced disability is crucial for developing targeted interventions aimed at preventing or minimizing the long-term effects of this condition. While tight glycemic control has been shown to reduce the risk of developing DPN [2], many patients still progress to severe stages of neuropathy, even with optimal diabetes management. This highlights the need for new therapeutic approaches that address the underlying nerve damage and improve functional outcomes. Furthermore, early diagnosis and management of DPN are critical for preventing disability. Regular screening and timely intervention can help identify individuals at risk for foot ulcers or falls, allowing for appropriate interventions such as foot care education, orthotics, or physical therapy. The socioeconomic burden of DPN-induced disability cannot be overlooked. Individuals with advanced DPN often require frequent hospitalizations for wound care, infections, or amputations, which contribute to the high healthcare costs associated with diabetes. In addition, the loss of productivity due to disability further strains both patients and the healthcare system. Investing in research to better understand the pathophysiology of DPN and develop cost-effective interventions could significantly reduce the financial burden of this condition. Studying DPN and its associated disabilities is of paramount importance due to the widespread prevalence of the condition, its profound impact on physical and mental health, and the substantial economic costs. Research efforts should focus on improving early detection, understanding the mechanisms driving nerve damage, and developing effective treatments to prevent disability and enhance quality of life for people with diabetes.
Methods
![]()
Literature search and selection criteria
Our Literature Search Strategy begins with defining clear research objectives and questions to establish the scope of the search. Utilizing keywords including but not limited to Diabetic Peripheral Neuropathy, Diabetes, Therapies, Controversies, Epidemiology, Pathophysiology, Diagnostics, Risk factors, Prevalence and Boolean operators (AND, OR, NOT) facilitates targeted searches across databases such as PubMed, Scopus, Web of Science. Incorporating synonyms, truncations, and controlled vocabulary like MeSH terms ensured the retrieval of diverse yet relevant sources. Selection criteria, encompassing inclusion and exclusion parameters, are critical to refine the results. Our criteria included publication type (Primarily reviews and Metanalysis), date range (after year 2010 mostly recent, in very rare case older references are included), geographical context: Global with focus on Middle east and Saudi Arabia. Ultimately, a robust strategy involving multiple iterative editing by the authors ensured that selected literature accurately supports the study’s objectives and reflects a comprehensive understanding of the topic.
Discussion![]()
Epidemiology of DPN
The burden of DPN in Saudi Arabia has been rising, parallel to the increasing prevalence of diabetes in the Kingdom. Saudi Arabia has one of the highest diabetes prevalence rates in the world, which consequently places the population at a higher risk for developing DPN. In 2021, the International Diabetes Federation (IDF) estimated that around 18.3% of the Saudi adult population has diabetes, which is significantly higher than the global average. As a complication of diabetes, DPN is expected to affect a considerable proportion of these individuals. The prevalence of DPN in Saudi Arabia varies across different studies, with reports suggesting that between 33% and 66% of diabetic patients are affected by DPN [5-6]. In a study conducted in Jeddah, a tertiary care hospital reported a DPN prevalence of 60% among Type 2 diabetes patients. Other cross-sectional studies confirm the high prevalence rates, especially in patients with poor glycemic control and a longer duration of diabetes [7]. These statistics reflect the growing burden of DPN as a direct consequence of the diabetes epidemic in the Kingdom, highlighting the need for public health interventions to address both prevention and management. Table. 1 summarizes the prevalence and contributing factors of DPN across the globe [5, 8].
Pathophysiology of Diabetic Peripheral Neuropathy (DPN)
Metabolic Factors in DPN
The primary driver of DPN is chronic hyperglycemia, which induces a cascade of biochemical alterations. The polyol pathway, advanced glycation end-products (AGEs) formation, hexosamine pathway, and protein kinase C (PKC) activation are key metabolic pathways involved in DPN [19].
· Polyol Pathway: In hyperglycemic conditions, glucose is reduced to sorbitol by the enzyme aldose reductase, leading to an accumulation of sorbitol and fructose. This accumulation depletes essential co-factors like nicotinamide adenine dinucleotide phosphate (NADPH), which is critical for regenerating the antioxidant glutathione. As a result, oxidative stress increases, contributing to neuronal damage [20].
· AGEs and Receptor for AGEs (RAGE): AGEs are the products of non-enzymatic glycation of proteins and lipids. Hyperglycemia accelerates the formation of AGEs, which accumulate in various tissues, including peripheral nerves. AGEs interact with their receptor (RAGE) to activate pro-inflammatory and pro-oxidant signaling pathways, further exacerbating nerve injury [21].
· Hexosamine Pathway: Excess glucose is diverted into the hexosamine pathway, where fructose-6-phosphate is converted into uridine diphosphate N-acetylglucosamine (UDP-GlcNAc), which modifies proteins through O-linked N-acetylglucosamine (O-GlcNAcylation). This modification affects numerous cellular processes, including transcription and insulin signaling, contributing to neurodegeneration [22].
· PKC Activation: Hyperglycemia activates the diacylglycerol-PKC pathway, which affects vascular flow by increasing vascular permeability and inducing endothelial dysfunction. PKC activation also promotes inflammation and oxidative stress, leading to neuronal ischemia and damage [14].
Oxidative Stress and Mitochondrial Dysfunction
Oxidative stress is a central mechanism in the pathogenesis of DPN. Hyperglycemia-induced overproduction of reactive oxygen species (ROS) disrupts the mitochondrial electron transport chain, leading to mitochondrial dysfunction. This results in impaired energy metabolism and increased apoptosis of neuronal cells. The imbalance between ROS production and the body's antioxidant defenses (e.g., glutathione) exacerbates oxidative damage to DNA, proteins, and lipids within peripheral nerves. This oxidative damage leads to structural alterations in the nerves, including axonal degeneration and demyelination [23]. Mitochondrial dysfunction also plays a significant role in DPN by reducing ATP production, which is critical for maintaining neuronal function. The reduced energy supply impairs axonal transport, contributing to the progressive loss of nerve function observed in DPN patients.
Inflammation and Immune Response
Chronic inflammation is another crucial factor contributing to DPN. Hyperglycemia induces a low-grade inflammatory state by promoting the activation of pro-inflammatory pathways, including the nuclear factor kappa B (NF-κB) and c-Jun N-terminal kinase (JNK) pathways. These pathways upregulate the expression of inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin-1β (IL-1β), and interleukin-6 (IL-6), which further amplify the inflammatory response and contribute to nerve damage. The activation of immune cells, such as macrophages and T cells, within peripheral nerves has also been implicated in the progression of DPN. These immune cells release cytokines and chemokines that promote a pro-inflammatory environment, exacerbating neuronal injury [24].
Vascular Dysfunction
Vascular dysfunction is a significant contributor to the pathophysiology of DPN. Hyperglycemia impairs endothelial function by reducing the availability of nitric oxide (NO), a critical vasodilator. The reduced NO levels lead to vasoconstriction and reduced blood flow to peripheral nerves, resulting in nerve ischemia. In addition, hyperglycemia induces the formation of AGEs, which cross-link with collagen in blood vessels, leading to stiffening of the vessel walls. This vascular stiffness further impairs blood flow, depriving nerves of essential nutrients and oxygen, thereby contributing to neuronal dysfunction [25]. Microangiopathy, characterized by thickening of the basement membrane and reduced capillary density, has also been observed in patients with DPN. This microvascular damage leads to chronic ischemia of peripheral nerves, exacerbating neuronal injury and promoting the development of neuropathic pain [25].
Neurotrophic Factors and Axonal Degeneration
The loss of neurotrophic factors, such as nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), and insulin-like growth factor-1 (IGF-1), plays a significant role in the development of DPN. These neurotrophic factors are essential for the maintenance of neuronal structure and function. In diabetic conditions, the production of these factors is reduced, leading to impaired axonal regeneration and increased susceptibility to nerve damage. The reduced availability of neurotrophic factors also contributes to the degeneration of sensory and motor neurons, which is a hallmark of DPN [9]. Axonal degeneration in DPN is characterized by the loss of both myelinated and unmyelinated fibers. This degeneration leads to a reduction in nerve conduction velocity and impaired sensory perception, manifesting as symptoms such as numbness, tingling, and pain in the extremities [26].
Clinical Manifestations of Diabetic Peripheral Neuropathy (DPN)
Clinical manifestations of DPN, including sensory, motor, and autonomic symptoms, pose a serious impact on patients’ quality of life. Here are the highlights of the underlying mechanisms contributing to these manifestations for DPN.
Sensory Manifestations
The most prominent clinical feature of DPN is the impairment of sensory function, which affects both large and small fibers. Sensory symptoms are typically the first to appear and often present in a "glove and stocking" distribution, affecting the distal extremities.
Positive Sensory Symptoms (Hyperalgesia and Allodynia): Patients with DPN frequently report positive sensory symptoms such as burning, tingling, or shooting pain, collectively referred to as hyperalgesia or allodynia. These symptoms arise from abnormal nerve excitability due to damage to small fibers [27-28]. Hyperalgesia occurs when normally non-painful stimuli, such as light touch, cause pain, while allodynia involves exaggerated pain responses to mild stimuli. The severity of these symptoms varies among individuals and can be debilitating, significantly affecting daily activities. Negative Sensory Symptoms (Numbness and Loss of Sensation): As DPN progresses, patients may experience negative sensory symptoms, including numbness and a loss of protective sensation. These symptoms are due to damage to large nerve fibers, leading to a diminished ability to perceive vibrations, temperature changes, and mechanical stimuli. The loss of sensation predisposes patients to injuries, such as foot ulcers, which can lead to infections and amputations if left untreated [29]. Loss of Vibration and Position Sense: Large fiber involvement also impairs proprioception, or the sense of joint position, and vibration sense. Patients may experience unsteadiness while walking and have difficulty maintaining balance, particularly in low-light conditions. This loss of proprioception is particularly concerning as it increases the risk of falls, further complicating the management of DPN.
Motor Manifestations
Although sensory symptoms predominate in DPN, motor dysfunction can also occur, particularly in more advanced stages of the disease. Motor symptoms are less common but can lead to significant disability.
Weakness and Muscle Atrophy: Damage to motor nerves can result in muscle weakness, particularly in the distal muscles of the lower limbs, such as the muscles controlling ankle and foot movements [30]. Patients may have difficulty lifting their feet (foot drop), which can cause tripping and falling. In severe cases, muscle atrophy can occur, leading to visible wasting of the muscles in the feet and lower legs [31]. Impaired Reflexes: Reduced or absent deep tendon reflexes, particularly the ankle jerk reflex, are common in DPN [3]. This is a sign of large-fiber neuropathy and is often one of the earliest detectable clinical signs of DPN. Reflex impairment contributes to difficulties with balance and gait. Gait Abnormalities: Patients with DPN often develop a characteristic "steppage" gait due to foot drop and loss of proprioception. This gait involves exaggerated lifting of the feet while walking to prevent tripping. Over time, these motor deficits can contribute to further complications, such as foot deformities and joint damage.
Autonomic Manifestations
Autonomic neuropathy is a less recognized but equally important manifestation of DPN. It affects the autonomic nervous system, which controls involuntary body functions, such as heart rate, digestion, and sweating.
Cardiovascular Symptoms: Cardiovascular autonomic neuropathy (CAN) is a common complication of DPN and can lead to resting tachycardia, orthostatic hypotension, and an increased risk of sudden cardiac death [32]. CAN impairs the heart’s ability to adjust to different levels of physical activity, resulting in exercise intolerance and an increased risk of fainting due to orthostatic hypotension (a sudden drop in blood pressure when standing. Gastrointestinal Symptoms: Autonomic neuropathy can affect gastrointestinal function, leading to gastroparesis, which is the delayed emptying of the stomach. Symptoms include nausea, vomiting, bloating, and abdominal discomfort, which can worsen blood glucose control. Constipation and diarrhea, especially at night, are also common gastrointestinal manifestations of autonomic neuropathy in DPN patients [33]. Genitourinary Symptoms: Autonomic neuropathy in DPN can cause bladder dysfunction, including urinary retention, incontinence, and an increased risk of urinary tract infections. Additionally, sexual dysfunction, such as erectile dysfunction in men and decreased vaginal lubrication in women, is a frequent complaint in patients with DPN [33]. Sweat Gland Dysfunction: Autonomic neuropathy affects the sweat glands, leading to abnormal sweating patterns. Patients may experience reduced sweating in the extremities (anhidrosis), which increases the risk of dry skin and foot ulcers. Conversely, compensatory hyperhidrosis (excessive sweating) may occur in other areas of the body [34].
Risk Factors for Diabetic Peripheral Neuropathy (DPN)
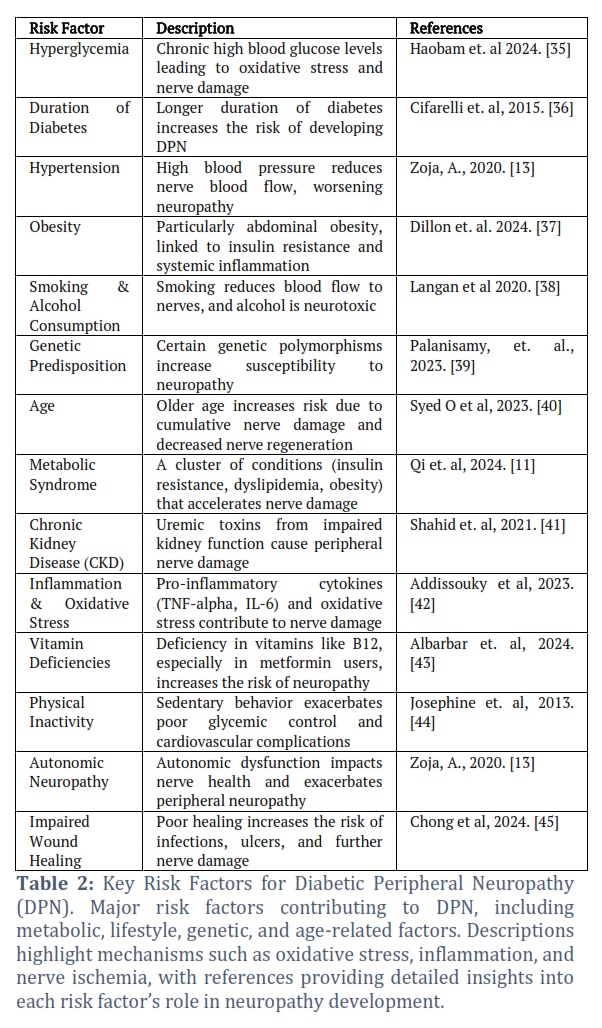
Understanding the risk factors associated with DPN is crucial for early identification and management of at-risk patients, thereby preventing progression to severe neuropathic complications like foot ulcers or amputations. Below we have discussed various risk factors contributing to the onset and progression of DPN, citing key research studies. Table. 2 summarizes the major risk factors for DPN
Advances in diagnosis of DPN
Early detection is crucial to prevent severe consequences, such as foot ulcers, infections, and amputations. This review focuses on the diagnosis of DPN, outlining clinical evaluation, advanced diagnostic tests, and emerging biomarkers.
Clinical Diagnosis
Patient History and Symptom Assessment
The initial step in diagnosing DPN involves gathering a comprehensive patient history and evaluating symptoms. Patients typically present with sensory disturbances, including numbness, tingling, burning sensations, and shooting pains, usually in a "glove-and-stocking" distribution [46]. Sensory loss often begins distally and may progress proximally as the condition worsens.
Neurological Examination
A key component of the clinical diagnosis is a neurological examination, which assesses sensory deficits and motor impairments.
Monofilament Testing: The 10g monofilament test is a widely used method to assess protective sensation, particularly for detecting the risk of foot ulcers in individuals with DPN [47]. Vibration Perception: Vibration perception testing using a 128Hz tuning fork is an essential part of large-fiber neuropathy assessment. A reduction in vibration perception suggests early involvement of large nerve fibers. Pinprick and Temperature Sensation: These tests assess small-fiber function, which is typically impaired in the early stages of DPN. Pinprick sensation and the ability to distinguish between warm and cool stimuli are critical for detecting small-fiber neuropathy [48].
Scoring Systems
Several scoring systems have been developed to quantify DPN severity:
· Michigan Neuropathy Screening Instrument (MNSI): This scoring system combines a symptom questionnaire with a clinical examination to assess both small and large nerve fiber involvement (American Diabetes Association Professional Practice Committee, 2022, [49]).
· Neuropathy Symptom Score (NSS): This tool rates the severity of neuropathic symptoms and helps in grading the condition [48].
Electrophysiological Testing
Nerve Conduction Studies (NCS)
NCS remains the gold standard for diagnosing large-fiber neuropathy. This test evaluates nerve function by measuring conduction velocity and response amplitude. In patients with DPN, reduced nerve conduction velocities and low-amplitude responses indicate axonal damage or demyelination [50]. NCS is particularly valuable in differentiating DPN from other forms of neuropathy.
Electromyography (EMG)
EMG is used in conjunction with NCS to assess muscle activity and differentiate between neuropathic and myopathic conditions. While not always necessary in DPN diagnosis, EMG can be helpful in ambiguous cases [51].
Therapeutic Approaches for DPN
We have explored the various therapeutic strategies for DPN, focusing on current treatments, emerging approaches, and potential future therapies aimed at addressing the key mechanisms involved in the progression of DPN.
Current Therapeutic Approaches
The current management of DPN primarily focuses on glycemic control and symptomatic treatment. These approaches are essential to delay the progression of neuropathy and manage neuropathic pain, but they do not reverse nerve damage or directly target the underlying causes.
Glycemic Control: Tight glycemic control remains a cornerstone in the management of DPN, as chronic hyperglycemia is the primary factor driving nerve damage. Studies have shown that maintaining optimal blood glucose levels can reduce the risk of developing DPN and slow its progression [52]. However, in patients with established DPN, glycemic control alone is often insufficient to reverse nerve damage, highlighting the need for additional therapeutic strategies. Pain Management: Neuropathic pain is a common and debilitating symptom of DPN. First-line treatments for pain include anticonvulsants such as gabapentin and pregabalin, and serotonin-norepinephrine reuptake inhibitors (SNRIs) like duloxetine [13]. While these medications help alleviate pain, they do not address the underlying causes of DPN or prevent further nerve damage. Additionally, opioid analgesics may be used for severe pain, but their long-term use is associated with significant risks, including tolerance and dependence [2].
Emerging Therapeutic Approaches
In recent years, there has been significant progress in understanding the pathophysiology of DPN, leading to the development of novel therapeutic approaches aimed at targeting the mechanisms underlying nerve damage. These emerging therapies include antioxidant therapy, anti-inflammatory agents, neurotrophic factors, and gene therapy [53].
Antioxidant Therapy: Oxidative stress plays a crucial role in the pathogenesis of DPN by causing damage to neurons and Schwann cells. Antioxidants such as alpha-lipoic acid (ALA) have been shown to reduce oxidative stress and improve nerve function in patients with DPN [54]. ALA acts by scavenging reactive oxygen species (ROS) and enhancing mitochondrial function, thereby reducing neuronal apoptosis. Additionally, acetyl-L-carnitine has been investigated for its neuroprotective properties and has shown promise in clinical trials for improving nerve conduction and reducing pain [55]. Anti-inflammatory Agents: Chronic inflammation is another key factor contributing to the progression of DPN. Several studies have investigated the use of anti-inflammatory agents, including nonsteroidal anti-inflammatory drugs (NSAIDs) and cytokine inhibitors, to reduce inflammation and prevent further nerve damage. Drugs targeting the nuclear factor kappa B (NF-κB) pathway, which is a major regulator of inflammation, have shown potential in preclinical studies [56]. Additionally, therapies targeting pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) are being explored as potential treatments for DPN [30]. Neurotrophic Factors: The loss of neurotrophic factors, such as nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF), contributes to neuronal degeneration in DPN. Experimental therapies aimed at increasing the levels of these neurotrophic factors have shown promise in promoting nerve regeneration and preventing further damage. NGF mimetics and BDNF analogs are currently being investigated for their potential to enhance neuronal survival and improve functional outcomes in DPN patients [57]. Gene Therapy: Gene therapy represents a novel approach for treating DPN by targeting the genetic pathways involved in nerve damage and repair. Preclinical studies have demonstrated that gene therapy can increase the expression of neurotrophic factors, enhance mitochondrial function, and reduce oxidative stress in animal models of DPN [9]. Although gene therapy is still in the early stages of development, it holds significant potential as a long-term treatment option for DPN. Stem Cell Therapy: Stem cells have the ability to differentiate into various cell types, including neurons and Schwann cells, making them an attractive option for regenerating damaged nerves. Mesenchymal stem cells (MSCs) and induced pluripotent stem cells (iPSCs) have shown promise in preclinical models of DPN by promoting nerve regeneration and reducing inflammation [58, 42]. Clinical trials are currently underway to evaluate the safety and efficacy of stem cell therapy in patients with DPN.
Mitochondrial Dysfunction and Therapeutic Approaches
Mitochondrial dysfunction contributes to diabetic peripheral neuropathy (DPN) by impairing energy production and increasing oxidative stress. Therapeutic strategies include: Mitochondrial-Targeted Antioxidants: MitoQ reduces oxidative stress, protects mitochondria, and preserves neuronal function in preclinical DPN models. Clinical trials are underway to evaluate its efficacy [39]. Pharmacological Agents for Biogenesis: PGC-1α activators enhance mitochondrial biogenesis, improving ATP production and reducing neuronal damage [59].
Targeting Vascular Dysfunction in DPN
Vascular dysfunction exacerbates nerve ischemia in DPN. Key therapeutic approaches include: Vasodilators: NO donors and phosphodiesterase inhibitors improve blood flow, restoring oxygen and nutrients to ischemic nerves [60]. Anti-Angiogenic Therapies: VEGF inhibitors reduce abnormal blood vessel growth, enhancing vascular function in preclinical studies.
Immunotherapy in DPN
Immune system involvement in DPN progression highlights potential immunotherapeutic targets: Immune Modulation: Therapies inhibiting T-cell activation and modulating macrophage polarization reduce inflammation and promote repair. Checkpoint Inhibitors: Borrowing from cancer treatments, these agents enhance immune-mediated nerve repair by blocking inhibitory immune signals.
Controversies Regarding Diabetic Peripheral Neuropathy (DPN)
Despite widespread occurrence and significant impact of DPN on patients' quality of life, several controversies exist regarding its diagnosis, classification, management, and understanding of its pathophysiological mechanisms. We have delved deep into the various controversies surrounding DPN, drawing on recent scientific discussions and clinical debates.
Controversies in Diagnosis and Classification
One of the major controversies in DPN is the lack of standardized diagnostic criteria. Multiple guidelines recommend different diagnostic tools and thresholds, leading to significant variability in how DPN is identified across clinical settings [61]. Some clinicians rely on nerve conduction studies (NCS), while others emphasize clinical examinations or patient-reported outcomes. The use of NCS is often considered the gold standard, but it has limitations, including its sensitivity in detecting small fiber neuropathy, which is an early form of DPN [61]. In terms of classification, DPN is traditionally divided into two broad categories: painful and painless neuropathy. However, some studies suggest that this dichotomy oversimplifies the condition, as patients may experience fluctuating symptoms, and some may not fit neatly into these categories. Additionally, distinguishing between DPN and other neuropathies (e.g., idiopathic or chemotherapy-induced) remains challenging, particularly in older populations where multiple comorbidities can obscure the diagnosis [61].
Pathophysiological Debates
The underlying pathophysiology of DPN is another area of controversy. While hyperglycemia-induced nerve damage is well-established as a primary driver of DPN, several other mechanisms have been proposed, including oxidative stress, mitochondrial dysfunction, and inflammation. However, the exact interplay between these factors remains unclear. For instance, it is debated whether oxidative stress is a primary cause of nerve damage or a byproduct of hyperglycemia, and whether targeting oxidative pathways would provide substantial therapeutic benefit [61].
Another contentious issue is the role of advanced glycation end-products (AGEs) in DPN progression. While AGEs are known to accumulate in diabetic patients and contribute to nerve damage, some researchers argue that their role may be overstated and that other factors, such as dyslipidemia and inflammation, may play equally significant roles [61].
Moreover, recent evidence points to the involvement of mitochondrial bioenergetics and dysfunction in DPN. This has led to debates about the potential for treatments that target mitochondrial health, although clinical trials have produced mixed results [61]. The lack of consistent findings in this area further complicates the understanding of DPN pathogenesis.
Controversies in Pain Management
The management of pain in DPN is fraught with controversy. The mainstay treatments for painful DPN include anticonvulsants (e.g., pregabalin, gabapentin), antidepressants (e.g., duloxetine, amitriptyline), and opioids. However, there is significant debate over the efficacy and safety of these treatments. For example, while pregabalin is widely prescribed, its effectiveness in real-world settings has been questioned due to issues with patient adherence and its side effects, such as dizziness and weight gain [61]. Opioid use in DPN is especially controversial due to the risks of addiction and overdose. Despite the potential for opioids to provide short-term pain relief, many experts argue against their use for chronic DPN due to the high risk of dependency and the relatively modest benefits observed in clinical trials [61]. This has led to a push for non-opioid alternatives, although finding effective replacements remains a challenge.
Discrepancies in Treatment Guidelines
Another area of controversy lies in the discrepancies between various treatment guidelines for DPN. For instance, while the American Diabetes Association (ADA) emphasizes glycemic control as the cornerstone of DPN prevention and management, other guidelines, such as those from the European Federation of Neurological Societies (EFNS), place more emphasis on symptomatic treatment and pain management [61]. These differences can lead to confusion among clinicians about the best course of action, particularly in patients with complex presentations.
Furthermore, while tight glycemic control is advocated for preventing DPN, especially in type 1 diabetes, there is ongoing debate about its effectiveness in type 2 diabetes. Some studies suggest that intensive glycemic control in type 2 diabetes may have only modest effects on reducing DPN risk, while increasing the risk of hypoglycemia and other complications [61]. This has led to calls for more individualized treatment plans that consider the patient’s overall health and risk profile.
Genetic Predisposition and Environmental Factors
There is also considerable debate about the role of genetic predisposition in the development of DPN. While some studies have identified genetic variants associated with an increased risk of DPN, these findings have not been consistently replicated across different populations (Schreiber et al., 2015). Additionally, the interplay between genetic factors and environmental exposures, such as diet and physical activity, remains poorly understood, further complicating efforts to predict which patients are at highest risk [61].
Personalized Medicine for Diabetic Peripheral Neuropathy (DPN)
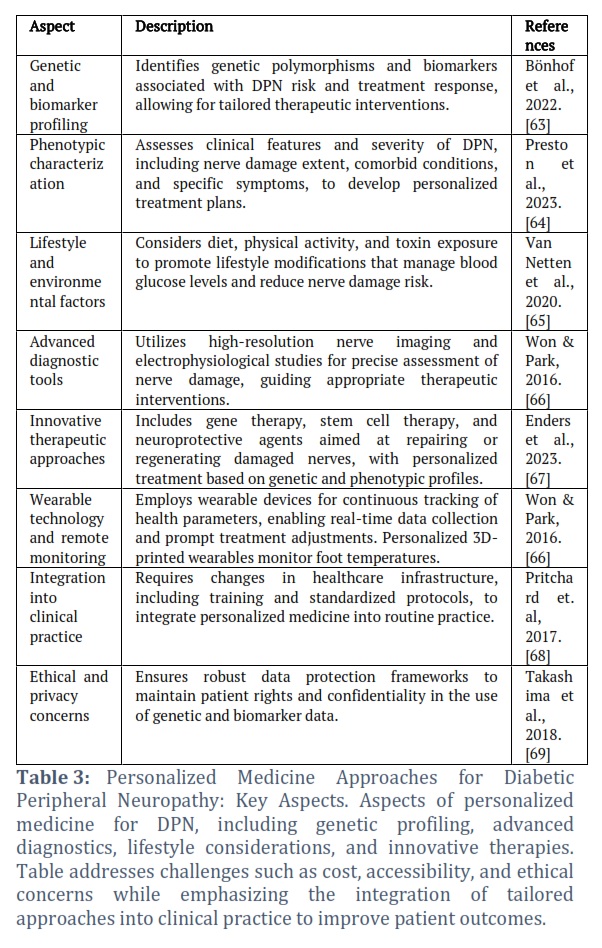
Traditional treatment approaches for DPN have largely been generalized, focusing on symptom management rather than addressing the underlying pathophysiological differences among patients. Personalized medicine, which tailors’ medical treatment to the individual characteristics of each patient, offers a promising approach to improve outcomes in DPN management [42]. The heterogeneity in presentation of DPN underscores the need for personalized treatment strategies that consider the unique genetic, environmental, and lifestyle factors influencing each patient’s condition [62]. Table 3 summarizes the key aspects of Personalized Medicine Approaches for Diabetic Peripheral Neuropathy.
Tables and Figures
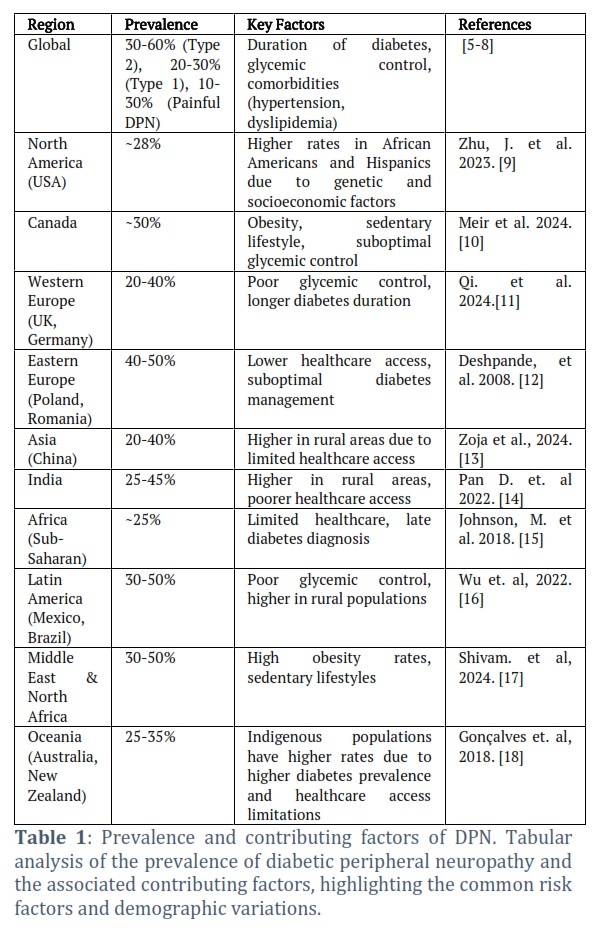
The prevalence of Diabetic Peripheral Neuropathy varies significantly across different regions of the world, reflecting disparities in healthcare access, diabetes management, and lifestyle factors. While North America and Europe exhibit relatively high prevalence rates due to the high prevalence of diabetes and obesity, regions such as Asia and Africa show significant variability, with rural populations being disproportionately affected. The growing prevalence of diabetes globally suggests that the burden of DPN will continue to rise in the coming decades, necessitating targeted public health interventions to improve diabetes management and prevent complications like DPN.
DPN remains a complex and multifaceted condition, with several ongoing controversies surrounding its diagnosis, classification, pathophysiology, and treatment. The lack of standardized diagnostic criteria and the variability in clinical guidelines contribute to confusion among clinicians, while debates about the underlying mechanisms of DPN and the best approaches to treatment highlight the need for further research. Additionally, socioeconomic and healthcare disparities continue to pose significant challenges to the effective management of DPN, particularly in underserved populations. Despite these controversies, progress is being made in understanding DPN, and emerging therapies hold promise for improving the quality of life for patients with this debilitating condition. However, addressing the unresolved questions and disparities in DPN care will require a concerted effort from researchers, clinicians, and policymakers alike. As the global burden of diabetes continues to rise, the need for effective, equitable, and evidence-based approaches to managing DPN becomes increasingly urgent.
Personalized medicine represents a paradigm shift in the management of DPN, offering the potential to improve patient outcomes through tailored treatment strategies. By considering the unique genetic, phenotypic, and environmental factors influencing each patient’s condition, personalized medicine can enhance the efficacy of interventions, reduce adverse effects, and ultimately improve the quality of life for patients with DPN. Continued research and advancements in this field are essential to overcome existing challenges and to make personalized medicine a standard approach in the management of DPN.
Future research in DPN should focus on advancing our understanding of the disease's pathophysiology, improving early detection through novel biomarkers, and developing new therapies, such as stem cell therapy, gene therapy, and anti-inflammatory agents. The integration of personalized medicine and lifestyle interventions will play a crucial role in managing DPN, potentially revolutionizing the way this debilitating condition is treated. However, significant challenges remain in translating these emerging therapies from preclinical studies to clinical practice, requiring continued research and innovation in the coming years.
Acknowledgements
The authors extend their appreciation to the King Salman center for Disability Research for funding this work through Research Group no KSRG-2022-012.
Author Contributions
Saif Khan (SK) conceptualized the review, developed the framework, and provided oversight for the manuscript. Saheem Ahmad (SA) conducted the primary literature search, data analysis, and synthesis. Mahvish Khan (MK) contributed to writing the introduction and background sections, while Mohtashim Lohani (ML) focused on the discussion and future perspectives. Mohammad Sajid (MS) critically reviewed and revised the manuscript, ensuring scientific accuracy and coherence. Mohammad Haneef (MH) assisted with editing, formatting, and finalizing the references. All authors reviewed, edited, and approved the final version of the manuscript for submission.
The authors declare that there is no conflict of interest regarding the publication of this paper.
![]() References
References
- Boulton AJ, Kirsner RS, Vileikyte L. Neuropathic diabetic foot ulcers. New England Journal of Medicine, (2004); 351(1):48-55.
- Schreiber AK, Nones CF, Reis RC, Chichorro JG, Cunha JM. Diabetic neuropathic pain: Physiopathology and treatment. World Journal of Diabetes, (2015); 6(3):432-44.
- Boulton AJ, Vinik AI, Arezzo JC, Bril V, Feldman EL et al. Diabetic neuropathies: A statement by the American Diabetes Association. Diabetes Care, (2006); 28(4):956-962.
- Pop-Busui R, Stevens MJ, Raffel DM, Feldman EL, Ziegler D. Diabetic neuropathy: A position statement by the American Diabetes Association. Diabetes Care, (2017); 40(1):136-154.
- Owolabi LF, Alghamdi M, Adamu B, et al. Magnitude of diabetic peripheral neuropathy in Saudi Arabia: a systematic review and meta-analysis. BMC Endocrine Disorders, (2022); 22:266.
- AlSufyani MH, Alzahrani AM, Aman Allah AA, Abdulla RI, Alzhrani SH, et al. Prevalence of painful diabetic peripheral neuropathy and its impact on quality of life among diabetic patients in Western region. Saudi Arabia. Journal of Family Medicine and Primary Care, (2020); 9(9):4897-4903.
- Alwin RA, Dawish MA. Microvascular complications among patients with diabetes: An emerging health problem in Saudi Arabia. Diabetes & Vascular Disease Research, (2019); 16(3):227-235.
- Dyck PJ, Melton III LJ, O'Brien PC, Service FJ. Approaches to improve epidemiological studies of diabetic neuropathy: insights from the Rochester Diabetic Neuropathy Study. Diabetes, (1997); 46(2): S5-8
- Zhu J, Hu Z, Luo Y, Liu Y, Luo W et al. Diabetic peripheral neuropathy: pathogenetic mechanisms and treatment. Frontiers in Endocrinology, (2024); 14:1265372-82.
- Meir J, Huang L, Mahmood S, Whiteson H, Cohen S et al. The vascular complications of diabetes: a review of their management, pathogenesis, and prevention. Expert Review of Endocrinology & Metabolism, (2024); 19(1):11-20.
- Qi H, Duan S, Xu Y, Zhang H. Frontiers and future perspectives of neuroimmunology. Fundamental Research, (2024); 4(2):206-17.
- Deshpande AD, Harris-Hayes M, Schootman M. Epidemiology of diabetes and diabetes-related complications. Physical Therapy, (2008); 88(11):1254-64.
- Zoja C, Xinaris C, Macconi D. Diabetic Nephropathy: Novel Molecular Mechanisms and Therapeutic Targets. Frontiers in Pharmacology, (2020); 11:586892.
- Pan D, Xu L, Guo M. The role of protein kinase C in diabetic microvascular complications. Frontiers in Endocrinology, (2022); 13:973058-70.
- Johnson M, Davis RJ, Robertson A. Role of oxidative stress in diabetes-related complications. Journal of Endocrinology, (2018); 5(2):143-148.
- Wu H, Norton V, Cui K, Zhu B, Bhattacharjee S et al. Diabetes and its cardiovascular complications: comprehensive network and systematic analyses. Frontiers in Cardiovascular Medicine, (2022); 9:841928.
- Shivam, Gupta AK, Kumar S. Current Concepts in the Molecular Mechanisms and Management of Diabetic Neuropathy by Pharmacotherapeutics and Natural Compounds. Central Nervous System Agents in Medicinal Chemistry, (2024); 24(3):264-80.
- Gonçalves NP, Vægter CB, Pallesen LT. Peripheral glial cells in the development of diabetic neuropathy. Frontiers in Neurology, (2018); 9:268.
- Trieb K. The Charcot foot: pathophysiology, diagnosis and classification. The Bone & Joint Journal, (2016); 98(9):1155-9.
- Zenker J, Ziegler D, Chrast R. Novel pathogenic pathways in diabetic neuropathy. Trends in Neurosciences, (2013); 36(8):439-49.
- Sugimoto K, Yasujima M, Yagihashi S. Role of advanced glycation end products in diabetic neuropathy. Current Pharmaceutical Design, (2008); 14(10):953-61.
- Sun Z, Liu Y, Zhao Y, Xu Y. Animal Models of Type 2 Diabetes Complications: A Review. Endocrine Research, (2024); 49(1):46-58.
- Mao JJ, Cao HJ, Chen X, Yu H. Herbal medicine in neuroprotection. Neural Regeneration Research, (2021); 16(8):1525-35.
- Rais N, Ved A, Ahmad R, Parveen A. Oxidative Stress and Diabetes Mellitus: Unravelling the Intricate Connection: A Comprehensive Review. Journal of Pharmaceutical Research International, (2024); 36(1):13-30.
- Lu Y, Wang W, Liu J, Xie M, Liu Q et al. Vascular complications of diabetes: A narrative review. Medicine (Baltimore), (2023); 102 (40): e35285.
- DiAntonio A. Axon degeneration: mechanistic insights lead to therapeutic opportunities for the prevention and treatment of peripheral neuropathy. Pain, (2019); 160:S17-S22.
- Campbell JN, Meyer RA. Mechanisms of neuropathic pain. Neuron, (2006); 52(1):77-92.
- Baron R, Binder A, Wasner G. Neuropathic pain: diagnosis, pathophysiological mechanisms, and treatment. The Lancet Neurology, (2010); 9(8):807-819.
- Armstrong DG, Tan TW, Boulton AJ, Bus SA. Diabetic foot ulcers: a review. Jama, (2023); 330(1):62-75.
- Ziegler D, Rathmann W, Dickhaus T, Meisinger C, Mielck A; KORA Study Group. Neuropathic pain in diabetes, prediabetes and normal glucose tolerance: the MONICA/KORA Augsburg Surveys S2 and S3. Pain Medicine, (2009); 10(2):393-400.
- Molsted S, Tribler J, Snorgaard O. Musculoskeletal pain in patients with type 2 diabetes. Diabetes Research and Clinical Practice, (2012); 96(2):135-40.
- Eleftheriadou A, Spallone V, Tahrani AA, Alam U. Cardiovascular autonomic neuropathy in diabetes: an update with a focus on management. Diabetologia, (2024); 1-5.
- Maiorino MI, Bellastella G, Esposito K. Diabetes and sexual dysfunction: current perspectives. Diabetes, Metabolic Syndrome and Obesity, (2014); 7:95-105.
- Anastasiou G, Liberopoulos E, Tentolouris N, Papanas N. Diabetic Sensorimotor Polyneuropathy: An Overview on Epidemiology, Risk Factors, Classification, Diagnosis, and Treatment. The International Journal of Lower Extremity Wounds, (2024); 15347346241240513.
- Haobam R, Nongthombam PD, Tongbram YC. Importance of Traditional Medicines in the Treatment of Neurological Diseases. In Traditional Resources and Tools for Modern Drug Discovery: Ethnomedicine and Pharmacology, (2024); pp. 527-550.
- Cifarelli V, Hursting SD. Obesity, Diabetes and Cancer: A Mechanistic Perspective. Int Journal of Diabetology and Vascular Disease Research, (2015); 4:10-20
- Dillon BR, Ang L, Pop-Busui R. Spectrum of Diabetic Neuropathy: New Insights in Diagnosis and Treatment. Annual Review of Medicine, (2024); 75:293-306.
- Langan D, Rose NR, Moudgil KD. Common innate pathways to autoimmune disease. Clinical Immunology, (2020); 212:108361-70.
- Palanisamy CP, Pei J, Alugoju P, Anthikapalli NVA, Jayaraman S et al. New strategies of neurodegenerative disease treatment with extracellular vesicles (EVs) derived from mesenchymal stem cells (MSCs). Theranostics, (2023); 13(12):4138-4165.
- Syed O, Jancic P, Knezevic NN. A Review of Recent Pharmacological Advances in the Management of Diabetes-Associated Peripheral Neuropathy. Pharmaceuticals, (2023); 16(6):801-812.
- Shahid RK, Ahmed S, Le D, Yadav S. Diabetes and Cancer: Risk, Challenges, Management and Outcomes. Cancers (Basel), (2021); 13(22):5735.
- Addissouky T, Ali M, El Sayed IE, Wang Y. Revolutionary innovations in diabetes research: from biomarkers to genomic medicine. Iranian Journal of Diabetes and Obesity, (2023); Dec 28.
- Albarbar B, Aga H. A Review on Autoimmune Diseases: Recent Advances and Future Perspectives. Al-Qalam Journal of Medical and Applied Sciences, (2024); 5:718-29.
- Josephine M. Forbes and Mark E. Coope. Mechanisms of diabetic complications. Physiological Reviews, (2013); 93: 137–88.
- Chong K, Chang JK, Chuang LM. Recent advances in the treatment of type 2 diabetes mellitus using new drug therapies. The Kaohsiung Journal of Medical Sciences, (2024); 40(3):212-20.
- Javed S, Hayat T, Menon L, Alam U, Malik RA. Diabetic peripheral neuropathy in people with type 2 diabetes: too little too late. Diabetic Medicine, (2020); 37(4):573-579.
- Petropoulos IN, Ponirakis G, Khan A, Almuhannadi H, Gad H, Malik RA. Diagnosing Diabetic Neuropathy: Something Old, Something New. Diabetes Metab J, (2018); 42(4):255-269.
- Mooi CS, Lee KW, Yusof Khan AH, Devaraj NK, Cheong AT et al. Using biothesiometer, Neuropathy Symptom Score, and Neuropathy Disability Score for the early detection of peripheral neuropathy: A cross-sectional study. Qatar Medical Journal, (2024); 2024(3):24.
- American Diabetes Association Professional Practice Committee. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2022. Diabetes Care, (2022); 45(1):S125-S143.
- Prashant P, Pal S, Bansal A, Fotedar S. Nerve conduction velocity studies in diabetic peripheral neuropathy involving sural nerve—A meta-analysis. Journal of Family Medicine and Primary Care, (2024); 13(10):4469-75.
- Galiero R, Caturano A, Vetrano E, Beccia D, Brin C et al. Peripheral Neuropathy in Diabetes Mellitus: Pathogenetic Mechanisms and Diagnostic Options. International Journal of Molecular Sciences, (2023); 24(4):3554.
- Pop-Busui R, Lu J, Brooks MM, Albert S, Althouse AD et al. BARI 2D Study Group. Impact of glycemic control strategies on the progression of diabetic peripheral neuropathy in the Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) Cohort. Diabetes Care, (2013); 36(10):3208-15.
- Bouhassira D, Attal N. Emerging therapies for neuropathic pain: new molecules or new indications for old treatments?. Pain, (2018); 159(3):576-582.
- Ratan Y, Rajput A, Pareek A, Pareek A, Kaur R et al. Recent Advances in Biomolecular Patho-Mechanistic Pathways behind the Development and Progression of Diabetic Neuropathy. Biomedicines, (2024); 12(7):1390.
- Lin Q, Li K, Chen Y, Xie J, Wu C et al. Oxidative stress in diabetic peripheral neuropathy: Pathway and mechanism-based treatment. Molecular Neurobiology, (2023); 60(8):4574-94.
- Akbar S, Subhan F, Akbar A, Habib F, Shahbaz N et al. Targeting Anti-Inflammatory Pathways to Treat Diabetes-Induced Neuropathy by 6-Hydroxyflavanone. Nutrients, (2023); 15(11):2552-62.
- Yagin FH, Georgian B. The Role of Genomics in Precision Medicine and Personalized Treatment in Diabetes Mellitus. Journal of Exercise Science & Physical Activity Reviews, (2024); 2(1):114-23.
- Antoniou M, Mateus C, Hollingsworth B, Titman A. A systematic review of methodologies used in models of the treatment of diabetes mellitus. Pharmacoeconomics, (2024); 42(1):19-40.
- Chandrasekaran K, Anjaneyulu M, Choi J, Kumar P, Salimian M et al. Role of mitochondria in diabetic peripheral neuropathy: Influencing the NAD+-dependent SIRT1-PGC-1α-TFAM pathway. Int Rev Neurobiol, (2019); 145:177-209.
- Akter S, Choubey M, Mohib MM, Arbee S, Sagor MAT et al. Stem Cell Therapy in Diabetic Polyneuropathy: Recent Advancements and Future Directions. Brain Science, (2023); 13(2):255.
- Calcutt N, Fernyhough P. Controversies in diabetic neuropathy. Academic Press; 2016 Apr 28.
- Røikjer J, Borbjerg MK, Andresen T, Giordano R, Hviid CV et al. Diabetic Peripheral Neuropathy: Emerging Treatments of Neuropathic Pain and Novel Diagnostic Methods. Journal of Diabetes Science and Technology, (2024); 19322968241279553.
- Bönhof GJ, Herder C, Ziegler D. Diagnostic tools, biomarkers, and treatments in diabetic polyneuropathy and cardiovascular autonomic neuropathy. Current Diabetes Reviews, (2022); 18(5):156-80.
- Preston FG, Riley DR, Azmi S, Alam U. Painful Diabetic Peripheral Neuropathy: Practical Guidance and Challenges for Clinical Management. Diabetes, Metabolic Syndrome and Obesity, (2023); 16:1595-1612.
- Van Netten JJ, Bus SA, Apelqvist J, Chen P, Chuter V et al. Definitions and criteria for diabetes-related foot disease (IWGDF 2023 update). Diabetes/Metabolism Research and Reviews, (2024); 40(3):3654-62.
- Won JC, Park TS. Recent Advances in Diagnostic Strategies for Diabetic Peripheral Neuropathy. Endocrinology and Metabolism (Seoul), (2016); 31(2):230-8.
- Enders J, Elliott D, Wright DE. Emerging Nonpharmacologic Interventions to Treat Diabetic Peripheral Neuropathy. Antioxidants & Redox Signaling, (2023); 38(15):989-1000.
- Pritchard DE, Moeckel F, Villa MS, Housman LT, McCarty CA et al. Strategies for integrating personalized medicine into healthcare practice. Personalized Medicine, (2017); 14(2):141-152.
- Takashima K, Maru Y, Mori S, Mano H, Noda T et al. Ethical concerns on sharing genomic data including patients' family members. BMC Medical Ethics, (2018); 19(1):61.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0